Art was one of my key subjects to the completion of my schooling and when medicine became my goal, plastic surgery seemed a career path that was aligned to my passion yet what did I really understand about our specialty? The short answer is not much at all. Even as a medical student there was limited exposure to plastic surgery and my knowledge base still failed to develop. It wasn’t until I had my first rotation into a plastic surgery unit that the scope of our field became clearer.
If this represents the degree of understanding that our colleagues have about plastic surgery it is little wonder that there are myths commonly accepted as truths in relation to our craft group. These misconceptions persist because the comprehensive scope of plastic surgery training and the importance of the principles of plastic surgery are not truly appreciated beyond our craft group.
One must look at the origins of our specialty to understand the nature of discovery and scientific pursuit that has led to the development of a craft group at the forefront of medical innovation. From there we can see that there is stepwise learning starting with the acquisition of knowledge and in particular an expert understanding of anatomy, next an understanding of principles and then the development of technical skills. These principles are applied to the unique individual challenges posed by congenital deformity, asymmetry, infection, trauma and tumour. As these skills are honed and the procedures become more reliable the procedures can be applied to lesser and lesser forms of change until they become reliable procedures that are applied to address physiological changes such as the changes associated with massive weight loss, pregnancy, ageing or degeneration. This process of improvement and refinement is a continuum.
Any discussion about the popular historical roots of plastic surgery frequently start with a description of Indian rhinoplasty by Sushruta in 600 BC1 and progress through a convoluted period during the middle ages to the description of the Italian method of nasal reconstruction by Gaspare Tagliacozzi in the 1500s. Tagliacozzi is quoted from his work:
We restore, rebuild, and make whole those parts which nature hath given, but which fortune has taken away. Not so much that it may delight the eye, but that it might buoy up the spirit, and help the mind of the afflicted.2
Plastic surgery developed as a way to assuage the suffering experienced by people whose faces had been disfigured through vengeance or punishment. In a book by Bryan Mendelson, In your face,3 he eloquently describes the impact of facial disfigurement which has been used for millennia as punishment or vengeance. The cover of Time magazine on 9 August 2010 (Vol 176 No 6) illustrates the cruelty and significance of facial disfigurement. Amputation of the nasal tip forces the victim to see themselves as an outcast from the moment of disfigurement.
Gillies and Millard outlined in their book, The principles and art of plastic surgery in 1957,4 the goals in order of priority are healing, the restoration of function and form. Reconstructive surgery has always had the consistent goal to normalise not just function but aesthetics. In fact the quality of our reconstructions are judged not just by function but by how closely the result approaches natural or normal appearances.
Mendelson stated:
Reconstructive surgery was the foundation of plastic surgery, as the procedures became more reliable surgeons were able to turn their skills to help people attain facial improvement beyond the normal, that is, to improve a person’s aesthetic appearance even though they are not actually disfigured by accident, injury or illness. But even then, the patient’s psychological motivation for surgery remains the same: an overly large nose or exaggerated facial feature has the capacity, as we’ve seen, to destroy confidence and alter lives.3
The techniques we use do not arise by chance. Common to all of these great physicians is a grounding in surgical principles, a background of scientific exploration, attention to prior writings and a studious examination of anatomy in particular.
If we fast forward there are innumerable modern examples to demonstrate how an inquisitive plastic surgical mind has helped develop reliable aesthetic surgical procedures on the basis of the very same commitment to the scientific process.
Fritz E Barton’s text on facial rejuvenation published in 20085 outlines his personal process of discovery leading to the evolution of the High SMAS facelift technique. Drawing on a comprehensive understanding of the literature and anatomy he developed a theory regarding an improvement in facial rejuvenation surgery. His group performed anatomical dissections and vascular injection studies to test the anatomical concept. A clinical application validated their theory in facial reconstructive patients using modified Juri-type cheek rotation flaps with his collaborators Tom Spicer, John Tebbetts, Steve Byrd and Mark Zilmer. The next step was to validate the concept clinically in aesthetic patients and subject these results to rigorous peer review for critical appraisal of the outcomes which culminated in a series of publications in the early 1990s.6,7 The high SMAS technique for face lifting remains a workhorse for many plastic surgeons.
The adoption of reconstructive surgical techniques in aesthetic procedures is perhaps most easily demonstrated in breast surgery. Breast reconstruction has long been among the most discussed, researched and captivating areas of plastic surgery. Many of our modern guiding principles have originated from research in association with breast reconstruction. Not simply the artistic elements of imagination or the three-dimensional concept of recreating aesthetics but also the genesis of some of the landmark principles of plastic surgery such as angiosomes,8,9 flap delay,10,11 choke zones,12,13 and microvascular surgery.
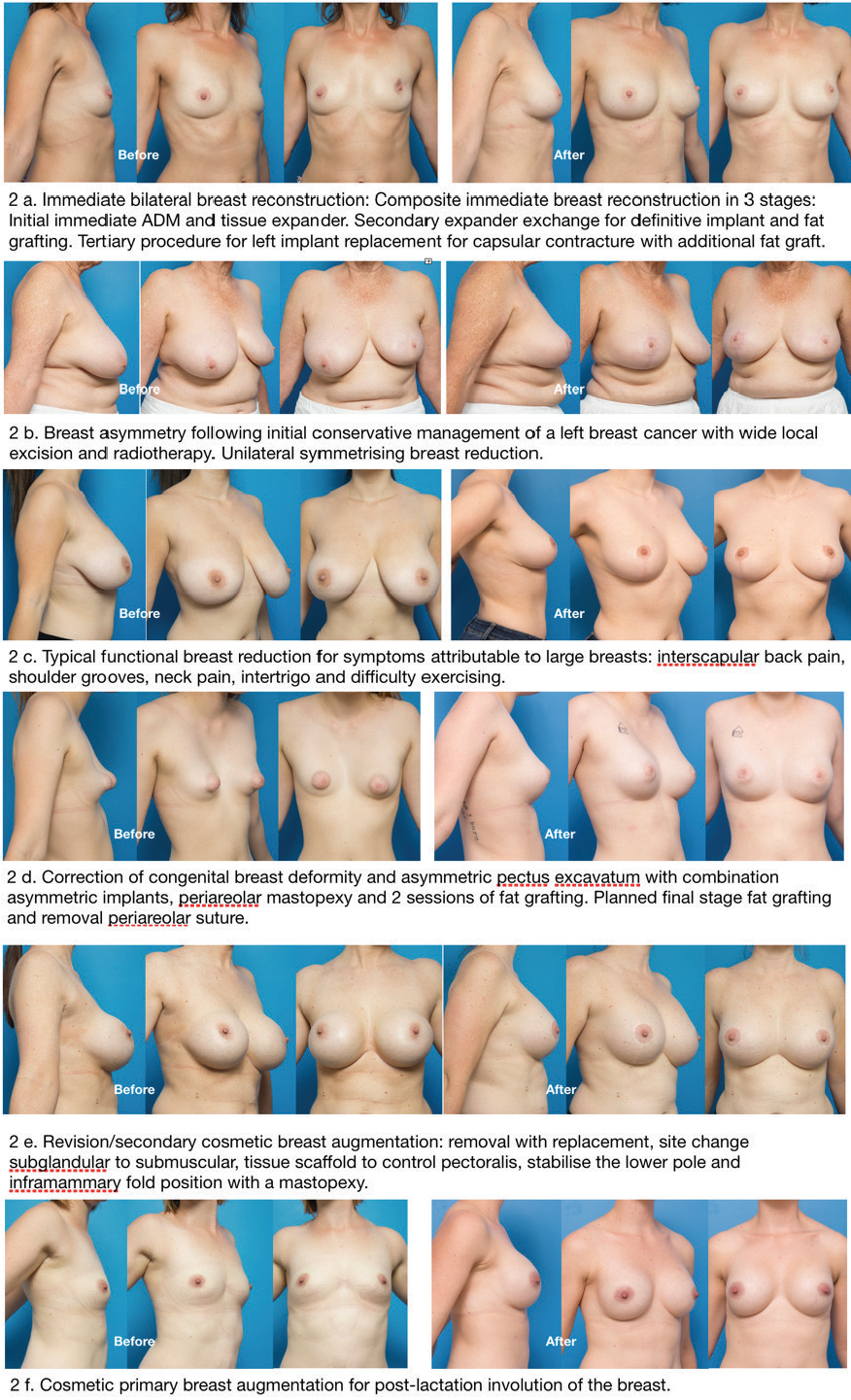
In the new millennium breast reconstruction continues to embody the nature of our specialty at the research coalface helping to advance the field of tissue engineering and improving our understanding of the application of fat grafting which are applied in composite breast reconstruction. In fact, as these techniques have become not just experimental but reliable, it is not surprising that these techniques have now become incorporated in aesthetic procedures such as the management of congenital deformity such as the tuberous breast and revision breast augmentation (Figure 1). Reconstruction, basic research and innovation are not divorced from aesthetic surgery but they are integrally linked.
In Australia and New Zealand the Royal Australasian College of Surgeons is the principal body responsible for training surgeons. The Royal Australian and New Zealand College of Obstetricians and Gynaecologists and the Royal Australian and New Zealand College of Ophthalmologists are the only colleges accredited by the Australian Medical Council (AMC) to train surgeons (excluding dental surgeons) as listed on the Medical Board of Australia (MBA) website.14 The AMC is responsible for accrediting education providers and their programs of study for medical practitioners on behalf of the MBA. The training programs are rigorously and transparently assessed to ensure that minimum standards are met and maintained. They are designed to provide trainees with clinical and operative experience in order to become competent in techniques related to these individual and specific disciplines.15
Plastic surgery training covers a broad scope of practice designed to provide a comprehensive understanding of surgical science and the principles of plastic surgery.16 The various areas of plastic surgery practice include management of the facial skeleton, facial soft tissues, chest, breast, trunk, perineum, skin and integument. Within each of these areas the management of the whole range of processes that occur are taught including the procedures and techniques associated which include aesthetic, congenital, degenerative, inflammatory, neoplastic and traumatic.
Additional non-technical skills are equally important such as collaboration, communication, health advocacy, clinical decision-making, professionalism, ethics and research. Non-maleficence is derived from the Latin phrase primum non nocere (first do no harm). It reminds the trainee that we must always consider the harm or risk inherent in a procedure and not simply the potential benefits. In short, we also learn when not to operate.
Trainees are taught the management of the newborn, paediatric, adult and geriatric patients both well and critically ill. Plastic surgery training is both comprehensive and difficult and we make no excuse for this. A competent and ethical surgeon helps ensure patient safety.
In contrast, in Australia and New Zealand, cosmetic surgery is not recognised as a separate specialty. There is no defined minimum standard qualification and consequently it can be used by any practitioner without requiring any additional training part from completing an internship. As a result it is ambiguous and misleading for the patient who is unable to clearly identify recognised surgical training amongst a jumble of fancy certificates with impressive titles received for participation in short and often commercial/ industry courses.
Within the plastic surgery community we aim to promote a culture of patient safety and the pursuit of excellence in all aspects of patient care. We foster innovation, research and collaboration both locally and abroad. The Australian breast device registry was developed by Australian plastic surgeons in collaboration with Monash University to enable the real time collection of epidemiologically sound data on device performance to improve patient safety by the early identification of adverse trends in relation to breast implant surgery.17–19 It is now rolled out through 13 countries through the international collaboration of breast device registry activities (ICOBRA). International collaboration in which Australian plastic surgeons also play a key role has also been vital to rapidly increase our understanding of breast implant associated-anaplastic large cell lymphoma.20–22
The ongoing commitment to the advancement of our craft through evidence based medicine, basic and clinical research are key elements for the continuing advancement of our specialty. In 2013, Zhang23 wrote about the classic citations in plastic surgery. He revealed that Australia is the second most prolific country in regards to the 100 most cited articles in plastic surgery. He also revealed that G Ian Taylor is the single most cited plastic surgery author.
Sugrue24 looked at the quality aesthetic surgery research published over the last 20 years and found that since the requirement for authors to report the level of evidence of their submissions, the number of high quality publications has significantly increased. As with other fields aesthetic surgery is based upon evidence based medicine. So who are the contributors?
If we compare plastic surgeons with the contribution of non-core cosmetic surgeons on a global scale we find very disparate contributions. A google search of cosmetic surgery journals yields three titles. The International Journal of Cosmetic Surgery and Aesthetic Dermatology had its last edition in 2003. The Journal of Cosmetic Surgery and Medicine’s last edition was in 2013. The American Journal of Cosmetic Surgery is the only one persisting that is non-core and it does so only as a quarterly journal. It isn’t easy to identify the specific number of plastic surgery journals, however in 2015 globally there were reportedly 62 medical journals entirely or partly dedicated to the various fields of plastic surgery.25
Plastic surgery is based on principles and doesn’t exist within an anatomical area. We have seen that various aspects of our discipline have crossover with other specialties. We have seen the emergence of the oculoplastic surgeon, the oncoplastic breast surgeon and the otolaryngology trained facial plastic surgeon. What does bind us is comprehensive surgical specialty training. There needs to be a recognised minimum qualification for surgeons and the scope of practice for individual practitioners needs to be clearly defined by their training. The nomenclature used to describe individual surgeons should be consistent and accurately reflect accredited training, qualification and experience.

Why does a patient want their facial naevus to be removed by a plastic surgeon? There is an unwritten public perception that the nature of plastic surgery training creates individual practitioners with such a broad skill set that they are the most capable of identifying the nuances of presenting problems and delivering favourable outcomes for their patients.
No one requests a bad scar or a visible deformity after trauma or tumour. No one asks for a breast reconstruction that isn’t recognisable as a breast. In reality, aesthetics is an integral part of every plastic surgery procedure.
Reconstructive surgery and well planned and executed aesthetic surgery are different sides of the same coin. The suggestion that plastic surgeons perform only reconstructive surgery and that cosmetic surgeons only train in cosmetic surgery makes a good sound bite in a day where headline news needs a short catchy snippet. In reality, a cosmetic surgeon has no defined minimum standard of training, it is an undefined term and not recognised as a specialty.
It is the complexity and rigour of the full spectrum of plastic surgery training that creates a practitioner with the broadest repertoire to manage even the simple cosmetic cases well. The complex and technically demanding elements of a difficult reconstruction following trauma, cancer or congenital deformity provide the fertile ground to develop and refine the necessary knowledge and skills for well executed aesthetic surgery. In the absence of comprehensive training, a little knowledge can be one of the most dangerous things.
The newly born Australasian Journal of Plastic Surgery gives fully qualified plastic surgeons a new option to explore thoughts, expand ideas and share knowledge. Let us begin.
Consent to publish
Patients signed informed consent regarding publishing their data and photographs.