Introduction
It is a privilege to have been asked to contribute to this inaugural edition of the Australasian Journal of Plastic Surgery. In this feature I intend to deal with the issues surrounding the introduction of new technologies into treatment protocols. In doing so I will use as an example the use of distraction osteogenesis (DO) of the mandible in cranofacial microsomia (CM). In an age of rapid technological advancement, easy dissemination of information and aggressive marketing it has become all too easy for the promising discovery of today to turn into tomorrow’s clinical nightmare. This dilemma has attracted the attention of ethicists and clinicians alike.1,2
I intend to trace the history of the introduction of DO of the mandible into the management of CM and using the published literature to trace the clinical outcomes. That these leave a lot to be desired is now well recorded. From the beginning I could not see any reason for the introduction of this technology into the established protocol. I will describe the principles that underpinned that decision.
Fundamental to applying these principles is a thorough knowledge of the pathology and pathogenesis of the condition to which the proposed technology is to be applied. I will describe the complex nature of CM, its variations, its classification, its development with growth and its multiple pathological manifestations; contemplation of which should immediately raise questions about the suitability of DO in this condition.
The use of distraction techniques was most commonly proposed for those varieties of the condition where a functional temporomandibular joint existed, and the application was made during growth. It was meant to replace those protocols that involved orthodontic management during growth3 and end point surgery on both hard and soft tissue at maturity. Noted enthusiasts claimed that this innovation was the end of osteotomies.4 By presenting a review of the literature I will show that a very different picture has emerged, which, when contrasted with the ‘classic’ protocol, casts severe doubt on the usefulness of the technique in this setting.
The discussion centres on the principles for the introduction of this new technology in surgery and the drivers for maintaining its popularity. Inevitably the argument returns to the proposition: ‘How could this be avoided?’ This author tenders the view that a thorough knowledge of the pathology and pathogenesis of CM would have raised the doubts that have taken so long to emerge. As a result there is a much wider problem to be addressed when introducing new technologies into established health care protocols.
The pathology and pathogenesis of craniofacial microsomia
Embryology
The diagnosis, treatment and prevention of developmental disorders are increasingly based on the revelations of genetics and molecular biology as the aetiological basis of dysmorphic syndromes. An understanding of normal development is needed to comprehend the complexities of the disease. Considerations of the very early stages of embryogenesis, sub cellular molecular biological mechanisms, differentiation, cytogenesis, histogenesis and morphogenesis, all of which constitutes a vast and increasing field of study, cannot possibly be covered. However, an appreciation of these underlying developmental phenomena must be borne in mind before framing and embarking on therapeutic regimes.5–11
The ectoderm of the germ disc forms a neural plate that elevates along the axis of the elongating disc to create bilateral neural folds. These folds conjoin at multiple sites in the median plane to form the neural tube. The neural crest is formed as the neural tube rolls up. The neural crest cells (ectoderm) arise in the interface between two separate epithelial cell layers; the roof plate of the neural tube and the overlying surface ectoderm. In the head, most mesenchyme arises from the neural crest cells. Ectoderm cells are located at the margins of the neural folds in the transition zone between the neuro ectoderm and the epidermis. This epithelial mesenchymal transformation is a key factor in the embryogenesis and its control accounts for precision of facial moulding or the lack thereof in malformations. During neural tube closure these crest cells migrate into the underlying tissues as mesenchyme (hence ectomesenchyme), forming potential stem cells that give rise to diverse tissues including the skull and pharyngeal arch cartilages.
The embryonic prominences of the face and neck are formed by the migration and proliferation of neural crest tissue. The cephalic neural crest provides the precursors of cartilage, bone, muscles and connective tissue of the head. The vasculature of the head is derived from mesoderm-derived endothelial precursors while neural crest tissue provides the pericytes and smooth muscle cells of the face and forebrain. The neural crest gives rise to the main proximal portions of the ganglia of the trigeminal (V), facial (V11), glossopharyngeal (1X), and vagus (X) nerves.
Most of the skeletal and connective tissue of the craniofacial complex and pharyngeal arch apparatus are dependent on mesencephalic and rhombencephalic neural crest tissue migrating as ectomesenchyme into ventral regions of the future skull, face and neck.6 Any defect in the quantity and quality of migrating ecto-mesenchyme manifests itself in the clinical condition of CM and indeed a wide range of other deformities.7
The derivatives of the brachial arches that are pertinent to this paper are:
-
The first arch (mandibular) goes on to form the mandibular and maxillary processes. Its nerve is the trigeminal nerve, with its maxillary and mandibular divisions, and it gives rise to the mylohyoid muscles, the muscles of mastication, the anterior belly of the digastric muscle, tympani muscle and the tensor veli palatini. It also gives rise to bone and cartilage, namely the Incus muscle, the Incus, the Greater Wing of Sphenoid and the maxillary prominence and the maxilla, zygoma, palatine and squamous temple bones from its maxillary prominence. From its mandibular prominence it gives rise to Meckel’s cartilage, the malleus and mandibular condyles. Subsequently, the mandible forms from around Meckel’s cartilage, which acts as an initial template but ultimately disappears as the mandible is formed by membranous ossification of surrounding tissue.
-
The second arch gives rise to the hyoid muscle and its nerve is the facial nerve (V11 cranial nerve). It forms the posterior belly of the digastric muscle, the muscles of facial expression, stapedius and stylohyoid muscles, the major part of the stapes, the styloid process and the lesser horn and upper portion of the body of the hyoid bone.
It is the brain that drives the neurocranial development and its absence results in an absence of the calvarium.9 This concept is consistent with that of the functional matrix as proposed by Moss.11 The growth, or lack of it, in each region influence that of the adjacent tissue as noted by Enlow.10
The facial skeleton is subdivided into an upper third, which incorporates the orbits; a middle third incorporating the nasal complex maxillae, zygomas, temple bones and ears; and a lower third composed of the mandible. The masticatory apparatus formed by the jaws, temporo-mandibular joint and teeth is interposed between the middle and lower thirds of the face. Growth anomalies occurring in each region influence growth in adjacent regions.10
The total skull is thus a mosaic of individual components, each having different characteristics of growth, development, maturation and function. Despite their individuality, each of the units is so integrated with the other that coordination of their growth is required for normal development.12 The failure of this correlation, aberration of inception, or faulty growth of an individual component results in distortive craniofacial relationships reflected in numerous dysmorphic syndromes including CM.
The mandible being central to the concept of DO in the management of CM, it is important to briefly reflect on its embryology. The mandible is a derivative of the first pharyngeal arch. Neural crest cells invade the mandibular and maxillary prominences during the fourth week of gestation. Meckel’s cartilage serves as the initial non-ossifying template for early mandibular growth at 41–45 days post-conception. By the sixth week, a single ossification centre appears for each half of the mandible at the bifurcation of the inferior alveolar nerve and artery into its mental and incisive branches. The condyle develops from endochondral ossification. Secondary cartilages of the mental protuberance form ossicles in the fibrous tissue of the symphysis during the seventh month in utero, and conversion of the syndesmosis to a synostosis through endochondral ossification of the symphysis occurs during the first year of life. At birth the mandible consists of two individual bones connected by a non-ossified central portion called the symphysis. The way in which the mandible develops and grows is completely different from that of any other bone.13–16
Pathology
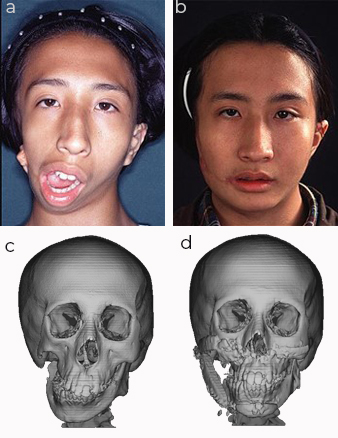
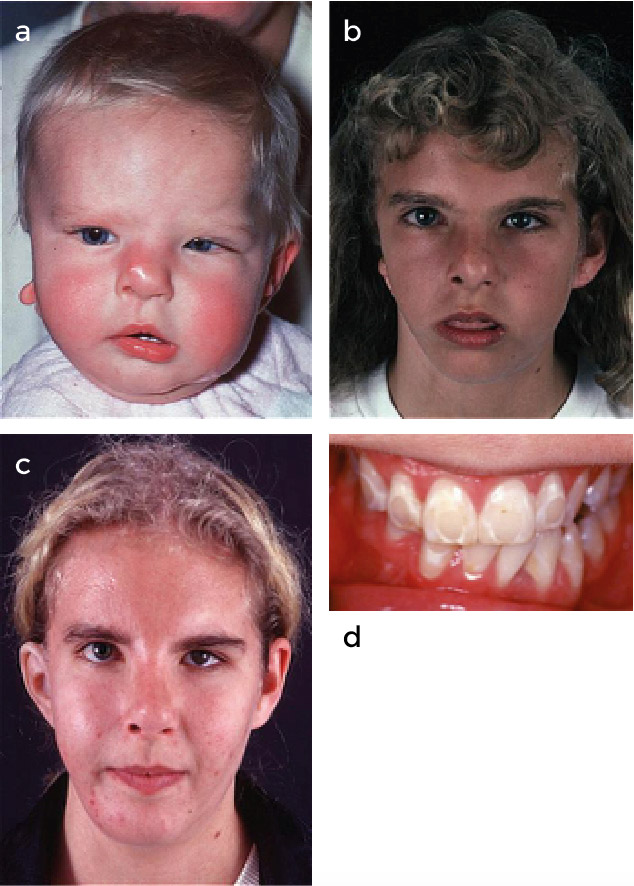
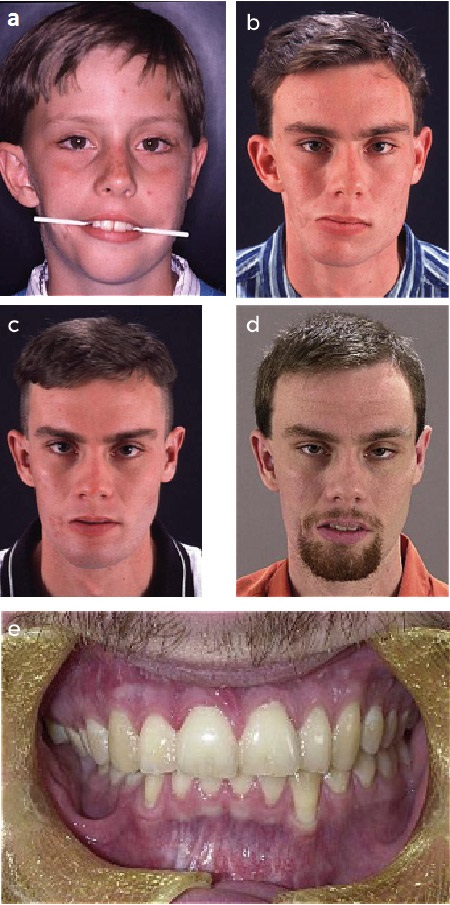
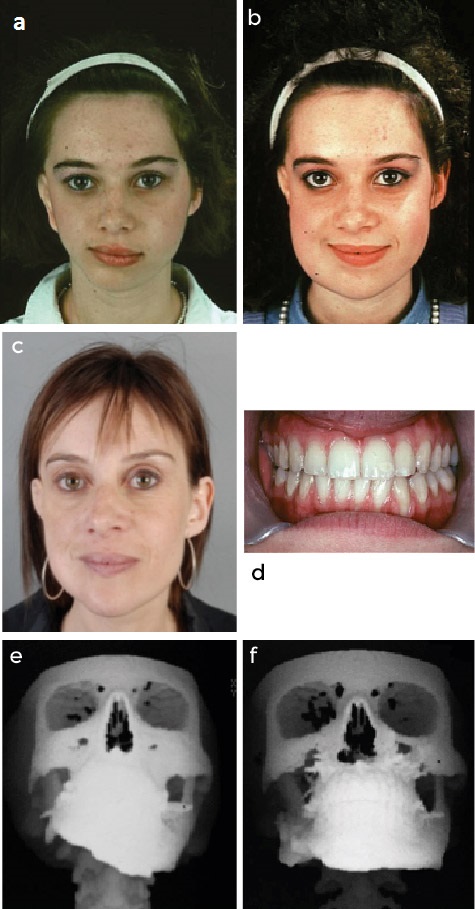
It is important to record the manifestations of the disease in its minimal as well as in its most severe expressions when patients present for clinical management (see Figures 1–4). Close observations of large series reveal a bewildering array of presentations. At one end of the spectrum the facial asymmetry is hardly noticeable with pre-auricular pits and tags, minor abnormalities of the external ear and very slight mandibular asymmetry, which may become more manifest with growth, and even the presence of a weakness in the mandibular branch of the facial nerve. At the other end of the spectrum, there are cases with complete absence of the mandible, the zygomatic arch, hypoplasia of the maxilla, absence of the eye on the affected side, gross macrostomia, palatal clefts, sometimes macrostomia on one side and cleft lip and palate on the other, and even asymmetrical bilateral presentations with the ear abnormality ranging all the way to complete absence. If we note that invariably the innervation of the palate on the side of the pathology is affected, and the presence in very rare cases of paramedian clefts together with the lateral hemi facial problems indicates that the pathology may not be centred around the pharyngeal arches. Hence, we need to account for other details such as the absence of the ocular globe and its secondary effect on the growth of the orbital cavity and adjacent bones.
_mature_patient_with_s4a3t3_deformity_presented_as_an_adult_with_the_macrosomia_treated._(.jpg)
_a_patient_with_s1__absent_ear_(a3)__and_absence_of_the_marginal_mandibular_branch_of_vii.jpeg)
_a_patient_with_s2a1_t3_the_latter_being_a_macrosomia_corrected_in_the_first_year._(b)_pri.jpeg)
_skeletal_4_deformity_managed_with_bimaxillary_surgery_at_end_of_growth_and_synchronous.jpeg)
The natural history of the pathology continues through to maturity as parts of the craniofacial skeleton develop normally and others do not. This gives rise to multiple secondary and tertiary effects; for example, the unilateral lack of muscle, and in the case of Goldenhar syndrome, the cervical vertebral anomalies giving rise to secondary muscle pull on the cranial base, producing distortions which in themselves produce added forces distorting the growing face. It is against this four dimensional complexity that appropriate protocols of management need to be put in place so that individuals suffering from these conditions obtain the best possible functional outcome.
Pathogenesis
Given the wide range of presentations of patients with CM, which of the classic theories of pathogenesis is the best fit? The neural crest cells are pluri potential cells derived from the dorsal lateral ectoderm adjacent to the neural tube, and they play a significant role in contributing to the mesenchyme responsible for the skeletal and connective tissue of the cranium and the face. It is generally believed that abnormalities in neural crest cell function, their quality, their quantity, how they migrate, and how they ultimately differentiate are fundamental to the pathogenesis of the formation of craniofacial clefts. The theories can be grouped into four:
-
Failure of fusion
This theory postulates that clefts result from failure of normally merging embryonic facial processes.
-
Incomplete mesodermal penetration and/or migration
This theory promotes the view that the facial processes do not contain free ends that need to fuse. Rather, the neural crests migrate into this envelope along a pre-determined pathway. The deficiency of both quality and quantity of free ends, or the ability of neural crests to migrate as stated above, causes the deformity.17
-
Vascular disturbances
The concept of an inter-uterine vascular event, whether it be causing embryonic hypoxia or producing a haematoma with indiscriminate damage of local cells, provides a particularly plausible explanation for the deformities of CM.18–20
-
Mechanical disruption, for example, amniotic band or other extrinsic mechanical factors do not appear to be directly applicable to CM
It is clear that the understanding of the pathology and the theories of pathogenesis of these complex conditions is being built upon, falsified and verified on a daily basis. It does not take a lot of imagination to understand that these basic four mechanisms are not in any sense mutually exclusive.
Birth to maturity and beyond
Before embarking on formulating a protocol for the management of patients suffering from CM, it is my belief that is it important to restate that the aim of treatment is to produce an individual at maturity whose function and form is as close to normal as possible. It is axiomatic that this cannot be done without an extra understanding of the forces at play from birth to maturity.
The theories of Moss14 concerning the functional matrix which has the muscles and their function stimulating bone growth (not bone lengthening creating new muscle) play a vital role in development and must vary with each individual.
Enlow’s10 observations of growth and development inform the view of the complexity of changes, the timing of growth spurts, and how bone growth is in part affected by the growth of adjacent bones.
The use of distraction osteogenesis techniques
For the purpose of this paper DO techniques for bone lengthening began with Ilizarov21 who described the technique for lengthening the femur. Snyder used the technique successfully in dogs.22 McCarthy and his colleagues from New York University applied the technique clinically to patients with CM and Nager syndrome.3 Since that time there has been an explosion in the use of bone distraction resulting in hundreds of additions to the literature. Special scientific meetings were convened to present results and evaluate outcomes.23
The tentative proposition from McCarthy’s first paper, and from others that followed,4 was that the distraction in young patients ‘can result in expansion (lengthening) not only of the jaw, but also of the attached muscles of mastication and motor nerves’. Implicit in this is that the indications for distraction include the presence of a functional temporomandibular joint.
Since the early 1990s DO has been used at the end of growth as an alternative to regular osteotomies, to augment unsatisfactory costochondral grafts which failed to grow, and to attempt to transport bone into the glenoid fossa to create a joint. The principle use of DO remains in the cases that have a functional temporomandibular joint (Pruzansky type 1 and 11a, or types S1 and S2 of the SAT classification).24 However, my argument involves the use of DO in a growing child in the presence of a functional joint.
The long-term follow-up paper from McCarthy25 deals specifically with those patients with well-developed joints using the Pruzansky classification, types I and IIa. These long-term results contribute to the discussion at hand (see below); it is their 25-year follow-up data that provides a ‘bookend’ to reflect on that period and the implications of the use of DO.
A literature review of the long-term outcomes
Despite over three decades of performing DO, there is limited data on long-term outcomes. I do not claim to have performed a systematic and/or in-depth review but have drawn on those of Shaw and colleagues,26 Nagy and colleagues27 and Pluijmers and colleagues.28 The search was made using PubMed and Embase, using the following terms:
(distraction [All Fields] AND (‘goldenhar syndrome’ [MeSH Terms] OR (‘goldenhar’ [All Fields] AND ‘syndrome’ [All Fields]) OR ‘goldenhar syndrome’ [All Fields] OR (‘hemifacial’ [All Fields] AND ‘macrosomia’ [All Fields]) OR ‘hemifacial macrosomia’ [All Fields])) AND long term [All Fields]
Date searched: 25 September 2017
This resulted in only 28 articles where DO was applied during growth in patients with functional joints. There were six retrospective reviews,25,29–33 two comparative studies,34,35 two prospective studies,36,37 three case reports,38–40 one systematic review,28 three reviews,27,41,42 and one comment supporting a review.43
There were nine articles that were not suitable for analysis:
-
where the long-term outcomes were not clearly described44
-
not about distraction45–47
-
focused on specific outcomes (for example, molar development,48 speech,49 distraction of a graft50)
-
not in English51,52 and
-
full access not available53 in the long term.
Thirteen studies reported long-term outcomes. Of the 145 patients with reported outcomes (Suh and colleagues32 was excluded as it was not clear how many patients had been treated), 91 (63%) patients were reported as having an unsatisfactory outcome, or relapse.31,33–36,38,39 Studies that reported positive outcomes attributed success to patients with lesser deformities,25,30 operated-on adolescents late in growth,29 or used multimodal therapies.37,40 In addition, Weichman25 and Baek30 reported some satisfactory and some unsatisfactory outcomes.
The published data suggest there is a niche population in CM patients, which should be limited to adolescents or adults, and those with moderate Pruzansky classifications (1 and 11a or S1 and S2 using the SAT). However, there is a significant incidence of relapse when used during growth and distraction may need to be complimented with other procedures long term, even in the most promising patient. The lack of success after so long is telling.
When Shaw and colleagues26 reviewed 82 reports on DO in an article entitled ‘Ethical and scientific decision making in distraction osteogenesis’, they made the following observations:
In these reports, mostly describing mandibular lengthening or maxillary advancement, retrospective short-term accounts of a small number of heterogeneous patients without controls has been the rule. Even more important is establishing whether distraction is better than traditional alternatives, like orthognathic surgery, including the obvious alternative of doing nothing.
The vast majority of articles reviewed according to the criteria above concluded that DO in a growing child with CM was unstable, the condition relapsed, the normal side out-grew the affected side and that further surgery was needed. Ow and colleagues,54 in their meta-analysis conclusion called for further clinical trials. Nagy and colleagues27 using the strict inclusion criteria ‘prospective and retrospective case series of infants and adolescents, not older than 16 years of age, who had undergone single stage, early unilateral osteodistraction of the mandible for correction of hemifacial microsomia or its equivalents, and follow-up for a duration longer than the active distraction phase’, found only 13 articles from the analysis from which they concluded that there was no convincing evidence supporting the effectiveness of early mandibular osteodistraction in hemifacial microsomia patients. Pluijmers and colleagues28 undertook a systemic review and concluded they ‘could not find statistical evidence for recommending DO as a single treatment modality in children’. The long-term follow-up article from Weichman and colleagues25 reporting McCarthy’s 25-year follow-up of DO in growing children, reports on 19 cases with 53.2 per cent having satisfactory results and 36.8 per cent unsatisfactory results.
A management protocol without distraction
In most of the presentations reviewed it is stated or implied that the protocols for the management of unilateral CM are well established and that DO has something extra to add by way of improved outcomes. It is therefore necessary to describe the protocol that I, and the team at the Australian craniofacial unit (ACFU), have developed, the basis on which it was developed, and the reasons for not changing the protocol to include DO.
We used the volume edited by Harvold55 as the basic template and applied the principles of scientific falsification56 to develop our approach, which involved describing an alphanumeric classification to provide some clear indicators as to the relevant surgery, as well as taking into account the soft tissue and auricular deformities.57 We adopted the logical approach outlined by Vargervik in Harvold’s monograph to distinguish between patients with a functioning joint and those without.
I presented the ‘end of growth’ findings in 120 cases in 1997 at The International Congress of Cleft Palate and Related Anomalies.58 The argument against DO was presented at the 8th International Congress of Craniofacial Surgery in 1999.2 The ACFU’s results were presented in 2005 in the Proceedings of the 11th International Congress of the Society of Craniofacial Surgery by Johnson and colleagues59 and the philosophy of management outlined.
On what basis did we not introduce DO into the established protocol? In the article presented at the 8th congress, I posed six questions that need to be answered before introducing new technology into clinical care:
-
On what basis are the results likely to be better?
-
Is the burden on the patient reduced?
-
Are traditional interventions made redundant?
-
Are the results achieved in a shorter time?
-
Does DO during development obviate surgery at the completion of growth?
-
Is it cheaper?
Because the complexities of this condition—which is multisystem, three-dimensional and changes with growth and time—it is not realistic to compare prospective controlled studies. To avoid introducing techniques that might harm patients, or at least be no better than the procedures that they displaced, reference was made to the pathology and pathogenesis of CM, and this provided the best guide at the time.
It was clear that DO could function only, or at least at best, in the presence of a functional joint. Within this S1, S2 (Pruzansky 1 and 11a) there is a wide range of other deformities depending on how much of the neural crest tissue, destined to form the first and second branchial arches, is missing.
Our decision was reinforced by consideration of Moss’s theory of the functional matrix, which has the muscles and function stimulating bone growth (not bone lengthening creating new muscle), together with Enlow’s observations that bone growth is in part affected by the growth of adjacent bones. An even stronger influence was the fact that during growth the ‘normal’ side continued to grow and the distracted side is unlikely to grow at the same rate, necessitating multiple interventions. DO would not remove the need for orthodontic management, and further surgery would inevitably be needed at maturity.
In patients without a joint, the costochondral graft reconstruction during growth has been well documented and is successful.60,61 The suggestion that when the joint is overgrown or inadequate that DO can be used was not considered logical as it is easier and simpler to graft or osteotomise at the end of growth.
My colleagues and I reported our management of severe cases of hemifacial microsomia by osteotomies and composite free flap surgery at the end of growth at the first congress of the International Society of Craniofacial surgery in 1985. There has never been a serious and supported argument for the use of DO in this situation.
Discussion
Rationale of the distraction technique
It has always been hard to determine exactly what the indications for DO in CM are. The airway problems associated with severe unilateral CM are not solved by this technique as there is nothing to distract. Those pathologies that might be considered for DO in this context are not CM.
McCarthy and colleagues’ admirable long-term follow-up paper25 now points out that ‘the indications for elective distraction are not clear’. They also raise the important question of appearance and psychosocial development and correctly note that ‘there is a paucity of data regarding this influence’. Despite multiple scientific meetings dedicated to the techniques of DO, and a massive outpouring of literature on the subject, in this particular disease we may well ask what has been achieved in a quarter of a century?
Limitations of the distraction technique
I first presented my arguments against the use of DO for CM in 19992 (see below). These views were formulated after close attention to the clinical analysis of the individual patients and paying attention to the current knowledge of development of the facial skeleton, to the theories of causation of CM, to the pathogenesis of the condition, and to its natural history through growth to maturity. So what does the literature now tell us?
Conclusions from the literature review (outcomes)
The vast majority of reports point out limitations in success using DO in growing children. Warnings appeared early, and hard data emerged with time. It was always in the mild to moderate cases with a functional joint where the potential success would be realised. However, this has not been shown to be the case. No argument appears at all in the literature to support the view that the ‘traditional’ protocols need to be replaced.
Principles for the introduction of new technology
There are six principles (Table 1) that should be applied before the introduction of new technology to a protocol,62 and I believe that they are more widely applicable than to the condition under consideration. Why change? Shaw and colleagues26 asked the question: ‘Why change a protocol, or indeed why do anything?’ They plead for adequate collaborative trials to avoid controversy and confusion. Added to this should be patient burden and even harm.
With the popularity of DO leading to near orthodoxy of treatment in CM there has been a dearth of reports of the long-term outcomes or those protocols that haven’t adopted DO. This in itself makes collaborative, multi-centre clinical research difficult.
Before the new technology was introduced there should have been a substantial literature review pointing to the inadequate results obtained from the standard protocols. Furthermore, multi-centre studies should have been mounted comparing the new with the old, and reported over time.
The burden of care for the patient was increased by adding long periods of distraction and at least two additional surgical interventions during childhood; manoeuvres that often needed repeating because of uneven and unstable growth.
DO did not (and could not) replace soft tissue, including restoring muscle and fat, and could not replace the need for orthodontic management to produce a functional and aesthetic occlusion. Nor could it rectify the asymmetry of the chin and nose and cheeks to optimise facial symmetry. Could a metallic device replicate the growth and development in four dimensions of the most unique bone in the body?
The final result in CM can only be achieved at the completion of growth, and what should have always been obvious, now supported by the literature. This involves osteotomies, grafts of hard and soft tissue and nasoseptal correction.
The costs of instrumentation, surgical time, additional hospitalisation and extra outpatient attendances is in addition to those levied against the traditional protocol procedures, as none of these have been made redundant.
In hindsight it can be said that DO might have been considered a replacement for the active orthodontic protocols that were aimed at strengthening muscle, maximising facial growth and tooth eruption in preparation for final surgical correction at the end of growth. The expectation was that the intervention of DO would obviate this last stage. The evidence is that DO in CM has not replaced the need for orthodontic management nor has it made end of growth surgery redundant.
What were the drivers for introducing distraction in this situation?
Given the difficulties in collecting valid evidence and mounting useful trials, how was it that DO so rapidly dominated the therapeutic approach to CM? There was little evidence that the well thought out protocols similar to that of Harvold55 were obvious failures. However, they, along with most other craniofacial deformity protocols, are complex, require specially organised teams treating a sufficient caseload, and require management extending from birth to maturity and beyond. It would seem that the belief and message that this technique would simplify treatment and relieve both patient and surgeon of the onus of orthognathic surgery was one of the drivers.
The technique had, and has, its heroes who added weight before evidence and gained exposure for their views in the learned literature. Molina and colleagues4 expressed this view in their article ‘Mandibular elongation and remodelling by distraction: a farewell to major osteotomies’; a view that persists.44
The promotion of the uses of DO in the craniofacial skeleton was achieved early on by multiple distraction conferences supported by the instrument manufacturing industry.23 Much good was achieved and many of the applications have withstood scrutiny and have been properly incorporated into the treatment protocols of other conditions. These meetings, however, contributed to hyperbole about use and outcomes with dissenting views taking a back seat.
The relationship between the surgical devices industry and the introduction of new technologies continues to be controversial.63 It appears to have been easy for both established specialists and more casual operators to use these techniques on their patients without knowing the outcomes and without scrutiny by any regulatory body.
How does the pathology and pathogenesis help?
The variations in the expression of the pathology in CM are compounded by growth and the secondary forces that come into play up to the time of maturity and beyond. From the beginning, the problem that I saw was being able to honour the scientifically based principles of clinical research when introducing new technologies and at the same time avoiding the ethical problems which may lead to harming patients.
While I and my colleagues at the ACFU saw a logical pathway for the introduction of DO into the protocols of other complex craniofacial anomalies,64 the same could not be said for the management of CM.
Knowledge of the morphogenesis occurring up to the time of birth, awareness of the theories of growth, together with the arguments surrounding pathology and pathogenesis, were critical in informing the ACFU’s decision to not use DO in the management of CM.
Conclusion
As the manifestations of the pathology develop during growth (pathogenesis), so the abnormal asymmetrical face is subject to the effects of the functional matrix13 and to the growth influences so well described by Enlow.15
Given that there is missing tissue, that a joint is needed for effective DO, that there are growth spurts during development, and that there is an obvious increased burden on the patient, and of course increased cost, we made the decision that there was no logical scientific reason to adopt DO in these cases.
There was no need to ‘do the experiment’ to know that missing tissue would need to be replaced, that there would be relapse of early promising results, and that growth spurts would be unfavourable to outcomes. The literature now shows the limitations of DO in growing children with CM. A greater consideration 25 years ago of the embryology and its drivers, and of pathology and pathogenesis, might have indicated a more considered approach to the management of CM by DO during growth.
Situations such as this point to the value of, and need for, training surgeons in the knowledge of pathology and pathogenesis of the target disease. One should not underestimate the value of the review articles referenced that demonstrate skilled analytical assessment of the literature.
It would seem that there is a greater need for clear guidelines for the introduction of new technology.
Acknowledgements
To all my colleagues at the Australian Craniofacial Unit, past and present. To Dr Jessica Reid, my valued research assistant.
Patient consent
Patients signed informed consent regarding publishing their data and photographs.
Disclosure
The authors have no conflicts of interest to disclose.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Revised: December 8, 2017 AEST