
Introduction
The deep inferior epigastric artery perforator (DIEP) flap has become a mainstay of modern microsurgical breast reconstruction. First described in 1989 by Koshima and Soeda,1 it was later popularised for breast reconstruction by Allen and Treece in 1994.2 This free flap is based on one or more perforators of the deep inferior epigastric artery (DIEA) that penetrate through the anterior rectus sheath following branching from the main vessel as it courses obliquely superomedially from the external iliac artery. Perfusion of the skin ellipse supplied by the perforator angiosomes3,4 of the DIEA has been classified into zones, the definition of which has evolved over time.
The perfusion zones of the DIEP originate from the studies of Scheflan and Dinner5,6 on the transverse rectus abdominis flap that then became known as the Hartrampf zones after his work was published on the TRAM flap.7 Hartrampf zones divide the lower abdominal ellipse of skin into four equal parts based on arterial inflow and set the boundaries for the level of perfusion of each portion of flap tissue that may be used for breast reconstruction. These TRAM flap zones were actually originally based around all cutaneous perforators of the DIEA to supply the skin, with the four parts numbered according to perfusion level, based on the assumption of a centrally perfused skin ellipse with peripherally decreasing supply.
The DIEP flap by contrast is supplied by only one or several perforators of the DIEA, with the zones applicable to the skin perfusion via these perforators.
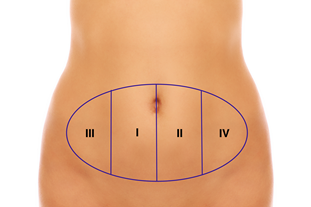
Zone I is the zone of greatest vascularity, with the main perforator underlying the area. Hartrampf, Scheflan and Dinner’s definition of zone II was the contralateral area (across the midline) adjacent to the perforator. Zone III was therefore the ipsilateral adjacent zone to zone I and zone IV the contralateral lateral zone, furthest away from the perforator. The works of Taylor and Palmer8 in 1987 demonstrated that these zones were in fact a variation of the angiosomes of the superficial and deep epigastric artery systems.
These zone assignments were later disputed by Scheflan and Dinner themselves,9 contesting that zone II should in fact be the ipsilateral adjacent zone, as they had noted that ipsilateral perfusion was consistently stronger than that that crossed the midline. The zones would then also correspond with the angiosomes of the ipsilateral and contralateral DIEA (Figure 1). Despite the suggestion that the two zones be switched, the zones continued to be assigned as per their original assignment until 2006 when Holm and colleagues10 revisited the topic demonstrating the DIEA perfusion anatomy using indocyanine green injections in 15 intraoperative specimens.

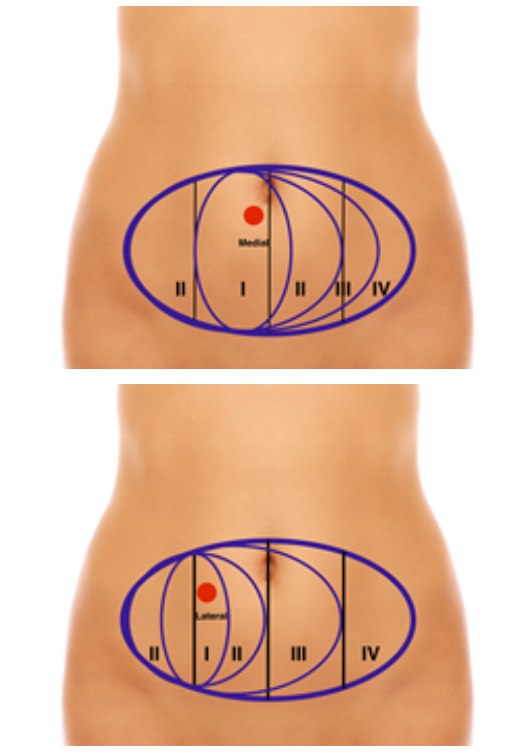
The zone definitions have since been further challenged following studies into perforator angiosome patterns and the identification of medial and lateral row perforators, each with different effects on the perfusion and therefore location and vascular territory of the zones. The works of Rozen and colleagues3 and Wong and colleagues4 identified the characteristics of medial and lateral row perforators through the use of injection studies and computerised tomographic angiography (CTA) thereby defining different zones of vascularity based on their new findings (Figure 2).
_and_lateral_(r)_row_pe.png)
The main characteristics identified have been as follows.
In zone I
-
Medial row perforators
-
Are larger with more extensive branching and are of larger caliber
-
Are centered over the position of the perforators as they emerge from the anterior rectus sheath, with a relatively direct course to the Scarpa’s fascia (at which point branching occurs)
-
Lateral row perforators
-
Have smaller vessels with less extensive branching
-
Are centered lateral to the location of the perforator at the anterior rectus sheath with a lengthy course traversed by the lateral row perforator before reaching the Scarpa’s fascia and branching.
In zones I & II
-
Medial row perforators
-
Routinely cross the midline to perfuse the medial parts of the contralateral hemiabdomen
-
Comprise more than the entire ipsilateral hemiabdomen
-
Lateral row perforators
-
Do not primarily communicate with branches that cross the midline
-
Have a limited maximal territory of perfusion.
Throughout the learning curve and development of extensive clinical experience with DIEP flaps there has arisen the opposing evidence regarding the viability of zone IV and its inclusion in the DIEP flap.11,12 Due to its position furthest away from the perforator supply, it is prone to vascular compromise, which can result in flap failure. Many authors now advocate for routine discarding of zone IV to avoid fat or flap necrosis.13,14
The mechanism and anatomy behind this necrosis is not, however, fully understood, the explanation of which would aid the surgeon in their preoperative planning and technique to improve DIEP flap success.
Methods
A PubMed and Embase search was performed regarding zone IV of the DIEP flap and its perfusion. Search words used were ‘zone IV AND DIEP’, ‘zone IV AND perfusion’, ‘zone IV DIEP AND ischaemia’, ‘vascular anatomy AND zone IV’. These searches revealed two systematic reviews, numerous case studies and experimental research papers, all of which were reviewed for relevant content.
A review of archival injection studies performed by the authors was undertaken to identify the arterial and venous maps of the abdomen. Unembalmed abdominal wall and full body specimens were used for cadaveric studies to demonstrate the arterial anastomotic patterns and venous drainage pathways of the deep inferior epigastric, superficial inferior epigastric, superficial circumflex iliac and intercostal systems.
Results and discussion
On review of the literature there are extensive studies on both the arterial and venous anatomy of the DIEP flap. Both arterial inflow and venous outflow characteristics have been associated with flap vascular compromise, with controversy as to which is the dominant mitigating factor.
Arterial anatomy
As previously stated the DIEP flap is supplied by medial or lateral row perforators that define the position of zone I. The primary zone of perfusion (the perforator angiosome) is therefore limited to the branches of that individual perforator, with wider supply based on anastomosis with adjacent perforator territories. Taylor and Palmer’s work into angiosomes in 1987 demonstrated the presence of ‘watershed’ supply between adjacent perfusion zones through ‘choke’ anastomoses8 allowing a progression of tissue perfusion originating from a single perforator. This was later supported in 201115 where injection studies demonstrated that when a flap is raised on a cutaneous perforator, anatomically, it is possible to safely raise one adjacent perforator angiosome territory in any direction where the supply connection is via choke anastomoses.
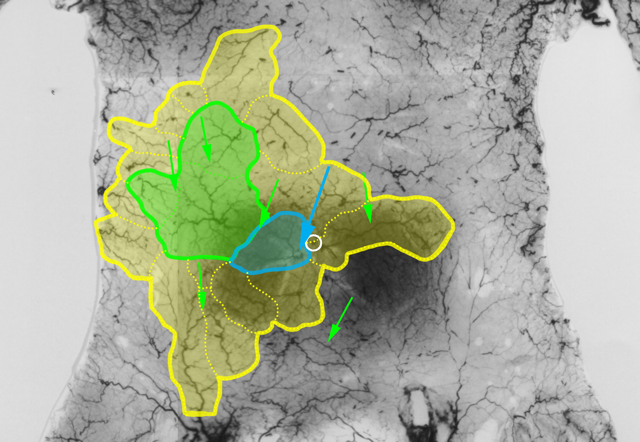
According to the perforator angiosome concept when a flap is raised on a cutaneous perforator, anatomically, one adjacent territory can be captured safely when the connections are choke anastomoses. For zone IV to be perfused adequately for flap transfer there must be a maximum of one set of choke anastomoses. Our review of 20 archival arterial injections studies for the presence of true and choke anastomoses in the anterior abdominal wall demonstrated high variability in the interperforator connections of the anterior abdominal wall (Figure 3).


In Figures 3 and 4, on the basis of either a medial or lateral row perforator, it is theoretically possible to perfuse zone IV of the DIEP flap however, this is reliant on the presence of true anastomoses. This is something which cannot be determined preoperatively at this stage.
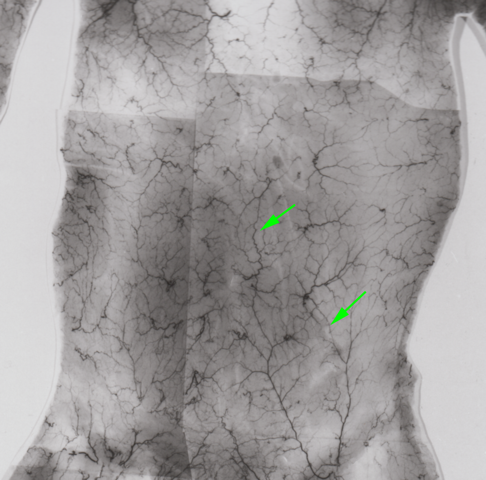
By contrast, in another abdominal specimen (Figure 5), it is possible to see that in some abdominal walls there are very few true anastomoses and so the flap is reliant on only choke anastomoses which will ultimately mean zone IV is not perfused.

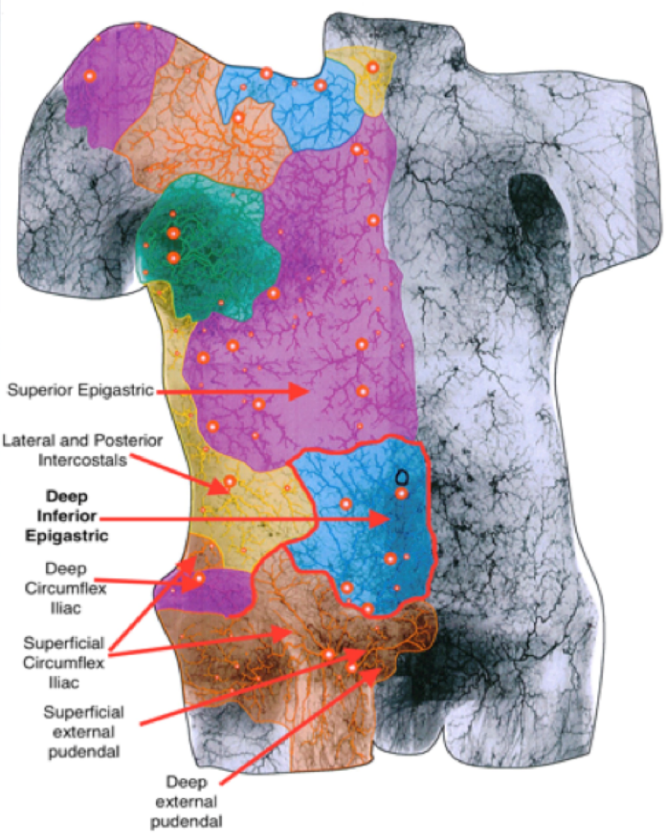
Although limited in number, our cadaveric injection systems do demonstrate the anatomic potential for perfusion of zone IV by the true anastomoses from the DIEA. These studies also demonstrate that whilst zone IV of a DIEP flap may not be perfused by its own medial or lateral row perforator it will receive supply via anastomoses from the lateral and posterior intercostal, deep circumflex iliac, superficial circumflex iliac and superior epigastric arteries. This may in turn reflect the reason why the zone IV area is not supplied by the DIEA as it has sufficient neighbouring supply (Figure 6).

Other anatomical studies would indicate a similar picture to our cadaveric injections, with Schaverien and colleagues16 showing in their injection studies that lateral row perforator dye did not cross the midline with no perfusion of zone IV. While some perfusion studies have not shown a statistical significance in the perfusion of zone IV in medial versus lateral perforators,17 others have again demonstrated that only some medial row perforator flaps and no lateral row perforator flaps will supply zone IV.18
In a systematic review by Ireton and colleagues19 on the vascular anatomy of the DIEP flap, perfusion territory was assessed through the use of various modalities, all of which demonstrated reduced or absent perfusion of zone IV. Holm and colleagues10 reported a median perfusion index of between 2–55 per cent, with perfusion absent in 33 per cent of patients independent of row perforators. In clinical studies by Blondeel and Heitmann and colleagues14,20 weak or absent perfusion of zone IV was found in 45–100 per cent of flaps and 40 hemiabdomens. Vascular mapping studies compared perfusion of zone IV in different row perforators with 0–22.7 per cent perfusion in medial vs zero per cent in lateral row perforators4,21 and evidence of medial row perforators extending halfway into zones III and IV in 100 per cent of cases and zero per cent of lateral row perforators crossing the midline.18
Schaverien and colleagues16 also noted that injection of the SIEA revealed a perfusion pattern similar to that of a lateral row perforator, with injection dye spreading through the subdermal plexus to ipsilateral medial and lateral row perforators by means of recurrent flow. The lateral row perforators also form choke anastomoses with the lower four intercostal arteries. All these anastomotic connections occur at the level of the subdermal plexus, with midline crossover also present in this layer. Perfusion deep to Scarpa’s fascia however arises from the suprafascial plexus (not part of the perforator angiosome territory). Schaverien noted that in zone IV, perfusion appears to be absent deep to Scarpa’s fascia, which has been clinically observed to be the predominant site of fat necrosis.22 A recent angiographical study has also demonstrated the importance of conservation of an intact dermis and subdermal plexus23 with a mean decrease of 25.9 per cent perfusion in flaps where the dermis was removed. It has therefore been advised that if thinning is required, this should be done meticulously thinning of the flap with preservation of the dermis.
Clinical studies have also supported the concept of choke anastomoses inhibiting flow to zone IV. In his original clinical series in 1999, Blondeel14 noted, that it is not the number of perforators but their distance from the midline that determines the viability of zone IV, stating that a lateral perforator flap will have little or no perfusion due to the fact that blood flow has to overcome an additional set of choke anastomoses compared with medial row perforators to reach zone IV. He therefore recommended that if zone IV was required in the design of a DIEP that the flap must be harvested on medial row perforators. Based on this, Blondeel also adopted the method of routinely discarding zone IV in his practice to avoid fat and/or flap necrosis. This custom has also been recommended by other authors10,11,13,24 based on both clinical and experimental studies.
Venous anatomy
Despite an original interest in the arterial anatomy as the basis of the zone IV unreliability, clinical experience has provoked further investigation into the venous anatomy of zone IV and its role in flap failure.
Following his recommendations regarding the arterial anatomy of zone IV, Blondeel and colleagues noted that venous congestion occurred in approximately two per cent of flaps and that the viability of zone IV may in fact be related to its venous anatomy.25 In a systematic review of 17,096 DIEP flaps from 1989 to 2011,26 there were 67 (out of 152) with a reported cause for flap failure, of which 40 per cent were venous compromise. A significant subset of these were cases of inadequate venous outflow despite a patent venous microanastomosis. Many of these reports of venous congestion that underwent venous re-exploration were found to have patent venous anastomoses but required a second venous anastomosis for decompression and establishment of adequate venous outflow. The clinical risk of fat necrosis is twice that in DIEP flaps versus TRAM, whereas arterial perfusion studies are similar, indicating the venous compromise may be the main determinant of flap necrosis as opposed to arterial.17
Anatomical and clinical studies detail the DIEP venous anatomy which comprises of superficial (superficial inferior epigastric vein—SIEV) and deep (deep inferior epigastric vein—DIEV) drainage systems connected by venae communicantes that drain the majority of the anterior abdominal wall.16 This main system is supported by the presence of a smaller network of venae comitantes which drain also to the deep DIEV system and whose territory generally matches the perforator artery angiosome which they accompany.27 The territories of these venae comitantes can be referred to as ‘cutaneous venosomes’ and, similar to their angiosome counterparts, communicate with adjacent territories via small caliber avalvular ‘oscillating’ veins that allow bidirectional flow and therefore drainage via more than more venous route.28
In the recent article by Lie and colleagues,27 hydrogen peroxide was used to define the venous architecture of the anterior abdominal wall, with its intravascular decomposition rendering venous valves incompetent and therefore allowing retrograde filling. The deep venous network travel as paired venae comitantes on either side of the DIEA and its branches which course vertically cephalad to the arcuate line and obliquely downwards to the external iliac vein below. Avalvular communicating branches are present between the paired venae comitantes, but no major midline connections were found, although lateral connections have been shown to exist with both the deep circumflex iliac vein (DCIV) and the posterior intercostal veins.
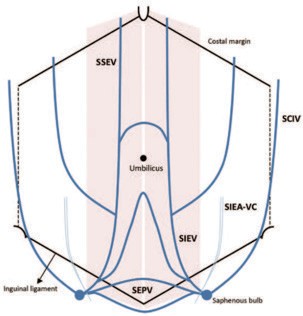
The superficial network of SIEV, superficial circumflex iliac vein (SCIV) and superficial external pudendal vein (SEPV) drain to the saphenous bulb or paraumbilical region with venae comitantes of the SIEV draining directly into the femoral vein. A major point of discussion of Blondeel and colleagues has been the presence and location of midline communication of the SIEV. Lie and colleagues defined two medial avalvular midline crossover branches; one in the supraumbilical region (midway between the xiphoid process and the umbilicus) and the other an infraumbilical connection, typically 2–4 cm below the umbilicus. This has also been previously noted by Rozen and Ashton who stated that the SIEV consistently lies superficial to Scarpa’s fascia with a large medial branch which crosses the midline in 86 per cent of cases (routinely below the arcuate line) (Figure 7).29

The works of Lie and colleagues further demonstrated the dominant venous drainage of the abdominal wall is through the large caliber primary superficial venous trunks (SIEV, SCIV) as they have the least resistance to venous outflow. During DIEP flap elevation, venous outflow is redirected from the superficial system to the perforator venae comitantes.30 This drainage via small caliber vessels cannot match the arterial inflow due to smaller vessel size (leading to higher flow resistance) and number (as many are sacrificed during flap harvest). This results in a global venous congestion, which has lead to the technique of ‘supercharging’31 or ‘life-boating’32 the DIEP with an additional SIEV anastomosis, which in turn relies on the degree of midline crossover and therefore contralateral drainage as found in the anatomical studies.
Indeed, experimental rat studies by Chang and colleagues33 have shown that augmentation of the venous system is effective in increasing flap survival. As has been observed in many clinical studies, most of the DIEP flaps suffer venous congestion as opposed to clinical arterial insufficiency. Arterially supercharging the flap would therefore worsen the venous congestion whereas increased venous drainage would alleviate it. The study showed that addition of ipsilateral SIEV, contralateral SIEV or DCIV drainage improved flap survival with the contralateral veins conferring a higher success rate. The authors also noted that all venous superdrainage flaps showed dilatation of the choke vessels in distally drained flaps (contralateral SIEV or DCIV) and those that survived showed venous dilatation as well. This would suggest that both a high arterial inflow is required to open the choke anastomoses and therefore consequently load the venous system to achieve both adequate perfusion and drainage for flap success.
Venous outflow studies have attempted to quantify the efficacy of SIEV in venous drainage. Van Landuyt and colleagues34 noted that DIEP flaps can be reliably extended to four zones on a single arterial pedicle provided a secondary venous outflow from the contralateral superficial inferior epigastric vein is connected (reliant on midline crossover drainage). Rothenberger and colleagues35 demonstrated that, by alternately clamping and declamping the contralateral SIEV, there was a significant difference (p <0.05) in venous outflow in the two contralateral zones (III and IV), demonstrating its role in venous drainage of the DIEP.
However, localised zone IV congestion likely results from a combination of factors. Zone IV is most susceptible to this due to reduced arterial pressure as a result of increased distance from the pedicle. In addition to this, small caliber communication between the (lateral) SCIV and (medial) SIEV territories leads to higher resistance to blood flow and venous drainage. The combination of reduced arterial pressure and increased venous pressure leads to localised decreased perfusion of zone IV. Zone IV is also similarly affected by the morphological variability of the SIEV and potential lack of crossover found in some patients as noted by Blondeel25 and Schaverien.16 The lack of crossover and therefore contralateral drainage implies that all drainage must follow the perforator venae comitantes system which is not large enough to accommodate the level of outflow, thereby potentially causing localised congestion. Venous variability also affects the degree of communication between the SIEV and the perforator venae comitantes, with small caliber vessels (oscillating veins) between adjacent venous territories then becoming the limiting factor in adjacent venosome territory drainage.
Pre- and peri-operative predictors of venous congestion have been examined by authors. Rozen and Ashton29 in 2012 stipulated that it is possible to see both superficial and deep aspects of the abdominal venous architecture via CTA and the communications between them but this communication between the SIEV and vena comitantes of the arterial perforators was only identifiable in 90 per cent of patients. This does not necessarily equate to being able to identify a system dominance. Clinically, intra-operative decisions made on the basis of a subjectively enlarged or engorged SIEV suggested it is the dominant drainage system following isolation of the flap on its pedicle. This has also been shown by Smit and colleagues36 in 2010 where preliminary results indicate that a higher venous pressure measured in the SIEV may correlate with a superficial venous system dominance and therefore a need to preserve and include the SIEV in flap drainage.
Conclusion
While anatomical vascular imaging and studies do appear to underestimate the true clinical vascular perfusion area, arterial and venous anatomical studies demonstrate clearly the vascular compromise potential in zone IV of the DIEP flap. The decreased perfusion studies and choke anastomotic supply demonstrate the relative hypoperfusion of zone IV and reliance on a medial row perforator harvest. This, however, is unlikely to be the main cause of flap compromise as clinical observations support a venous deficit which is anatomically multifactorial. The combination of inadequate perforator venae comitante drainage, high venous resistance of oscillating veins and variability of SIEV crossover would appear to underlie the venous compromise of zone IV.
From an arterial perspective, zone IV perfusion is reliant on medial row perforators and at maximum one set of choke anastomoses. On the basis of our abdominal injection studies, we have demonstrated that although true anastomoses are present in the abdominal wall they are highly variable and will not consistently supply zone IV. Additionally, there is currently no pre-operative options for identifying the type of anastomotic interperforator connections.
Conversely with the venous system, zone IV drainage is reliant on high resistance oscillating veins to carry venous drainage across venosomes to a small calibre venae comitante resulting in decreased drainage and congestion. When venous drainage is inadequate this can be salvaged by the addition of the SIEV however only if midline crossover is present. This can be visualised preoperatively with the use of CTA/MRA.
The authors therefore suggest that the failure of survival is a combination of both arterial and venous insufficiencies. On the basis of the literature and clinical and anatomical evidence, strategies for zone IV preservation can be proposed. The authors propose the following:
-
Thinning of the DIEP flap prior to inset with preservation of the dermis and subdermal plexus. This would preserve the subdermal connection channels between perforator angiosomes important for skin perfusion while also minimising the perfusion load of the plexus by removing unnecessary fat (which would require a portion of the blood supply and potentially compromise the overall perfusion of the flap).
-
Preservation of the SIEV to allow supercharging of the venous system if necessary.
-
Use of (when possible) medial row perforators for greater perfusion of zone IV.
Disclosure
The authors have no conflicts of interest to disclose.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Revised: December 13, 2017 AEST