Introduction
Craniosynostosis is the premature fusion of cranial sutures, resulting in craniofacial dysmorphism and potentially raised intracranial pressure (ICP).1 It is a rare disease, affecting 0.4 to 1.0 per 1000 live births.1,2 At around 60 per cent of cases, sagittal craniosynostosis is the most common form of non-syndromic single-suture craniosynostosis.1,3
Surgical correction in infancy is generally recommended to prevent raised ICP and psychosocial issues arising from a visible facial difference.3 However, the optimal approach remains in contention, requiring consideration of perioperative complications and long-term outcomes. Current surgical approaches can be divided into suturectomy and calvarial vault reshaping procedures. Suturectomy involves removal or osteotomy of the fused sagittal suture accompanied by spring placement, distractor placement or postoperative orthotic helmet therapy.3–5 Calvarial vault reshaping procedures involve removal, remodelling and replacement of large segments of calvarial bone.3–5
The use of springs in craniofacial surgery was first reported by Lauritzen and colleagues in 1998.6 Since then, low complication rates and good surgical outcomes using spring-assisted cranioplasty (SAC) for the management of sagittal craniosynostosis have been reported.3,4,7,8 Since 2008, our institution has preferred to treat all patients presenting with isolated sagittal craniosynostosis before seven months of age with SAC, and patients presenting after seven months of age with vault expansion or distraction osteogenesis. Spring-assisted cranioplasty involves an open sagittal suturectomy, followed by the insertion of metallic springs on either side of the osteotomy that slowly cause bitemporal widening until the springs are removed in a second procedure.1,7
The aim of this paper is to report our experience with SAC in the management of isolated non-syndromic sagittal craniosynostosis, documenting surgical characteristics, perioperative complications and long-term outcomes.
Methods
Study design
Following institutional review and ethics approval from the Sydney Children’s Hospitals Network Human Research Committee (HREC 2021/ETH11396), a retrospective review of consecutive patients with isolated sagittal craniosynostosis managed at our tertiary referral craniofacial centre between July 2008 and December 2021 was performed. Patients with multi-suture craniosynostosis at initial presentation were excluded, but those who developed synostosis of other sutures following treatment of initially isolated sagittal craniosynostosis were included. All medical records available on PowerChart (Cerner, Sydney, Australia), including electronic records and scanned paper records, were reviewed and relevant data extracted using REDCap electronic data capture tools (REDCap, Seattle, Washington).9
All patients referred to our centre with sagittal craniosynostosis were assessed in a multidisciplinary clinic consisting of plastic surgery, neurosurgery and ophthalmology. The presence of sagittal craniosynostosis was confirmed on CT scan and patients were offered surgical correction. For patients aged under seven months, SAC was generally recommended, though some older patients underwent SAC due to parent and/or surgeon preference. For older patients, either distraction osteogenesis or vault expansion was generally recommended and not collated in this study.
Spring-assisted cranioplasty operative technique
Patients were positioned prone. Tumescent solution containing local anaesthetic, adrenaline and steroids was infiltrated into the scalp. A lazy S-incision was made from the anterior to posterior fontanelles and the scalp and pericranium reflected to expose the fused sagittal suture. A 5–7 mm craniectomy was created along the fused sagittal suture from the anterior fontanelle to the confluence of lambdoid sutures. In addition, to facilitate lateral expansion, craniectomies approximately 2–3 cm long were created along the medial lambdoid and coronal sutures bilaterally. Adequate lateral movement of the parietal bones was confirmed with a rib spreader.
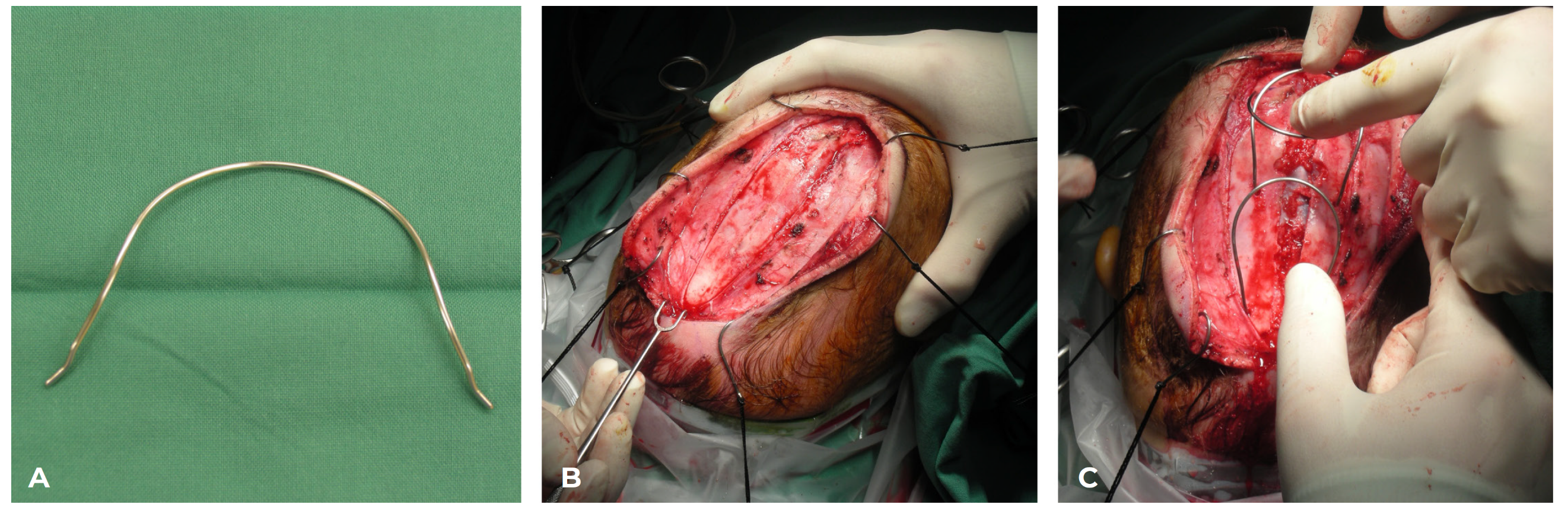
Stabilising burr holes were made in the parietal bones for the spring footplates, approximately 1 cm from the medial cut edge and towards the posterior part of the sagittal osteotomy, in order to differentially flare the parietal bones posteriorly and mimic normal head shape. Spring placement was not varied according to morphology or partial suture fusion. Two stainless steel springs (Biomed Ltd, Auckland, New Zealand) were washed in betadine and positioned into the burr holes (Figure 1). The loops of the springs were sutured down to the calvarium using heavy resorbable sutures passed through burr holes to eliminate dead space. The wound was irrigated with betadine. A drain was placed in the subgaleal space and the scalp closed in layers with resorbable sutures. No suction was placed on the drain. Intravenous antibiotics were continued for 48 hours. The drain was removed two to three days following surgery and patients were discharged with seven days of oral antibiotics. The springs were removed three months later under a second general anaesthetic.
_the_stainless_steel_springs_used_.png)
Data collection
Demographic information included date of birth and sex assigned at birth. Baseline data included type of craniosynostosis (syndromic versus non-syndromic), comorbidities, and raised ICP (pre-operative and postoperative). All comorbidities identified in medical records, whether diagnosed before or after craniosynostosis surgery, were included. Preoperative and postoperative raised ICPs were identified from the results of fundoscopy.
Data collected included date of surgery, age and weight at surgery, follow-up time, procedure performed, operative time (excluding anaesthetic time), performing surgeon, return to theatre, duration of hospitalisation, duration of antibiotic therapy, and intraoperative and postoperative blood transfusion. Blood transfusion was considered separately to complications because it is not an unexpected part of the operative course in craniofacial surgery on young infants. The distance between spring footplates at insertion was also collected. Between 2008 and 2012, two to four springs were inserted; since 2012, uniformly two springs were inserted. Mean footplate distances were calculated only from patients with two springs with available data.
Surgical complications data was collected for both procedures (spring insertion and spring removal). Total complication rate, rates of specific complications and rate of unplanned return to theatre were calculated. Finally, long-term outcomes were assessed by calculating rates of preoperative and postoperative raised ICP, and the rate of revision craniofacial surgery.
Statistical analysis
Descriptive statistics were performed and categorical variables were analysed using the chi-square (χ2) test, while continuous variables were analysed using the Kruskal–Wallis 1-way ANOVA test. Analyses were performed using R version 4.1.2 (R Project, Vienna, Austria).
Results
Demographics
In the 13-year study period, 122 patients with isolated sagittal craniosynostosis confirmed on CT scan were treated at our centre. Overall, 104 patients were treated with SAC (male = 73, female = 31; mean age 6.5 months, range 4–16 months; mean weight 7.9 kg, range 5.7–12.6 kg). In addition, nine patients were treated with vault expansion (male = 6, female = 3; mean age 29.7 months, range 10–55 months; mean weight 13.1 kg, range 9.5–16.7 kg) and nine patients were treated with distraction osteogenesis (male = 7, female = 2; mean age 21.7 months, range 14–37 months; mean weight 12.0 kg, range 10.1–16.8 kg). Patients who underwent vault expansion or distraction osteogenesis were excluded from further analysis.
Additional craniofacial issues were present in 12 (11.5%) patients, including micrognathia, malocclusion and cleft palate. Moreover, three (2.9%) patients were subsequently diagnosed with an identifiable syndrome (Mainzer–Saldino, Pierre Robin sequence/4q deletion and 7q11.23 duplication/6q27 microduplication). One additional patient had clinically suspected Noonan syndrome. Finally, five patients had a family history of sagittal craniosynostosis, with three patients having an affected first-degree relative and two patients having an affected third-degree relative.
Surgery characteristics
For spring insertion surgery, mean operative time was 63 minutes, followed by mean hospitalisation of 4.3 days with mean antibiotic length of 10.0 days. This excludes one patient who underwent spring insertion overseas and presented for spring removal. For spring removal surgery, mean operative time was 39 minutes, excluding one patient who had revision vault surgery performed simultaneously due to interval development of left unicoronal craniosynostosis.
Mean time from spring insertion to spring removal was 93.8 days (range 7–252 days). The shortest period was due to surgical site infection requiring emergency spring removal, while the longest period was due to skeletal abnormalities associated with Mainzer–Saldino syndrome. Mean spring expansion (increase in distance between the spring footplates) was 2.89 cm anteriorly and 3.12 cm posteriorly (Table 1).
During spring insertion, 55 (52.9%) patients required a blood transfusion. During spring removal, three (2.9%) patients required a postoperative blood transfusion. There were no complications associated with blood transfusion.
Perioperative complications
At spring insertion surgery, 23 patients (22.1%) experienced a complication (Table 2). The most common was surgical site infection (n = 9), which was managed with early spring removal (n = 4), incision and drainage (n = 1) and antibiotic treatment (n = 4). Moreover, two (1.9%) patients had exposed springs, with early spring removal in one patient and close monitoring with spring removal as planned in one patient. Finally, six patients (5.8%) had an unplanned return to theatre, with one patient requiring exploration and evacuation of a haematoma, four patients requiring early spring removal due to surgical site infection and one patient requiring early spring removal due to spring exposure.
At spring removal surgery, seven patients (6.7%) experienced a complication. The most common was superior sagittal sinus injury due to a lack of ossification across the midline defect between the two parietal bones (n = 3). Additionally, one patient (1.0%) had an unplanned return to theatre for drainage of scalp collection.
Long-term outcomes
This patient cohort had a mean follow-up of 3.9 years (range 1–11.5 years). Out of all patients, one had preoperative raised ICP as the indication for surgery which was resolved by the procedure.
Four patients required revision vault expansion surgery. The first patient (aged 6.5 months at first surgery) developed papilloedema and raised ICP on transcranial monitoring four years following SAC, which was treated with biparietal vault expansion. This patient was later determined to have 7q11.23 duplication syndrome and 6q27 microduplication syndrome.
In the second case, the patient (4 months) developed early postoperative asymmetrical vault expansion, confirmed by CT scan though no coronal craniosynostosis was found. At spring removal, osteotomies were performed to out-fracture the right parietal bone, which was then fixed with dissolving plates and screws. Since occipital positional plagiocephaly was detected on CT scan, the patient was treated with an orthotic helmet. Another scan performed 12 months after initial SAC confirmed new left unicoronal craniosynostosis, but no further surgery was performed due to good facial symmetry and increasing head circumference.
In the third case, the patient (5 months) had deteriorating head shape with increasing irritability, headbanging and headaches six months after SAC. Fundoscopy, CT and MRI were unremarkable, but transcranial pressure monitoring demonstrated raised ICP. Total calvarial vault remodelling was performed at two years of age. His behaviour and headaches improved following this procedure, with no recurrent symptoms at three years of follow-up.
In the fourth case, the patient (5 months) developed forehead asymmetry four years after SAC and a CT scan confirmed left unicoronal craniosynostosis. Fronto-orbital remodelling was performed.
Discussion
Although sagittal craniosynostosis is the most common form of craniosynostosis, there is no consensus regarding optimal surgical technique for correction. Surgical approaches have come full circle.4 The pioneering strip craniectomy, comprising open removal of the fused suture, had unpredictable long-term results and a high incidence of persistent sagittal craniosynostosis.3–5 Invasive total calvarial vault remodelling yielded superior and more durable results at the expense of increased morbidity.3–5 More recently, there has been a rediscovery of suturectomy procedures, usually with spring insertion, distraction osteogenesis or postoperative helmet orthosis.10 This single centre study assessing the outcomes of SAC in over 100 consecutive cases of isolated sagittal craniosynostosis demonstrates that it is safe and effective with a low revision rate. Our mean total operative time of 102 minutes, including both spring insertion and removal surgery, is longer than a previous study which found a mean time of 49 minutes, but still shorter than that study’s mean time of 143 minutes for vault expansion. Our mean hospital stay of 4.3 days is longer than previous reports of less than 24 hours.7 This is explained by our hospital’s protocol of 48 hours of intravenous antibiotics, followed by oral antibiotics on discharge. Following four consecutive cases of spring infection early in the study period, our protocol was altered to align with that of ventriculoperitoneal shunt insertion.
The need for blood transfusion in 52.9 per cent of patients is high, as previous studies have reported blood transfusion in 0 to 8 per cent overall,4,7,11 29.8 per cent intraoperatively and 9.2 per cent postoperatively.12 One study did report blood transfusion in 92.3 per cent of patients due to the hospital’s protocol,8 and our high rate may be similarly explained, since we do not use cell savers, erythropoietin, preoperative iron supplementation or other specific measures to reduce bleeding. Our mean total volume of transfusion of 80.3 mL is lower than a previous report of 143 mL,11 likely due to a smaller volume of transfusion in a larger number of patients, again reflecting protocol.
Unlike previous large series, there were no life-threatening or permanently disabling complications.11 The most common complication was surgical site infection (n = 9, 8.7%), which has been previously reported at a rate of 1.3–2 per cent.4,7,13 Exposed springs occurred in two patients, which has previously been reported in the literature with management varying from close observation, to skin undermining and closure, to early spring removal.4,7,13 In our study, one patient had early spring removal, while one later patient had close monitoring, reflecting the centre’s experience and recognition that early spring removal is not necessary if cellulitis, undesirable head shape or other complications are not detected. In our study, spring removal was associated with superior sagittal sinus injury requiring repair in three patients. Spring removal surgery can be associated with significant bleeding from the superior sagittal sinus and great care must be taken to protect this structure.
Finally, in regards to long-term outcomes, mean spring expansion of 2.89 cm anteriorly and 3.12 cm posteriorly is slightly less than previous reports of 4.8 cm and 4.9 cm.4 This could be due to variation in measurement technique. Our springs were custom made by a biomedical engineering service in Auckland, New Zealand, whereas other centres use springs made onsite (Wake Forest University, Great Ormond Street Hospital and Nicolae Testemitanu State University of Medicine and Pharmacy).1,3,4 The differences in spring expansion may be due to differences in spring design, manufacture and force.
Patients with isolated sagittal craniosynostosis treated in infancy may require subsequent surgery due to poor cosmesis, further craniosynostosis or raised ICP. In our study, vault expansion was required in three patients due to the development of new craniosynostosis and in one syndromic patient due to postoperative raised ICP, comprising 3.8 per cent of the cohort. This is similar to another study, where 5 per cent of patients required revision surgery due to postoperative raised ICP or residual head shape concerns.11
This study had several limitations. Our analysis of long-term outcomes was not comprehensive, with no objective or subjective evaluation of aesthetic outcomes or quantitative measures of calvarial vault expansion such as cephalic index or ratio of anterior to total cranial volume. Although 3D photography was performed preoperatively and at multiple time points postoperatively, that data is the subject of an ongoing study. Moreover, there was no randomisation and the number of patients who underwent the different procedures was very different, preventing direct comparison between SAC and other procedures.
Conclusion
Isolated sagittal craniosynostosis can be safely and effectively managed using SAC, with short operative times and hospital stays, manageable associated complications and acceptable long-term outcomes.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data. Consent was not otherwise obtained due to the retrospective and historical nature of the included data. Only data that is routinely collected as part of clinical care was analysed.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.
Revised: June 1, 2024 AEST