Whakaari/White Island is an uninhabited active volcano located 48 km off the east coast of New Zealand’s North Island in the Bay of Plenty. It has been a popular tourist attraction for over 30 years with approximately 20,000 visitors annually.
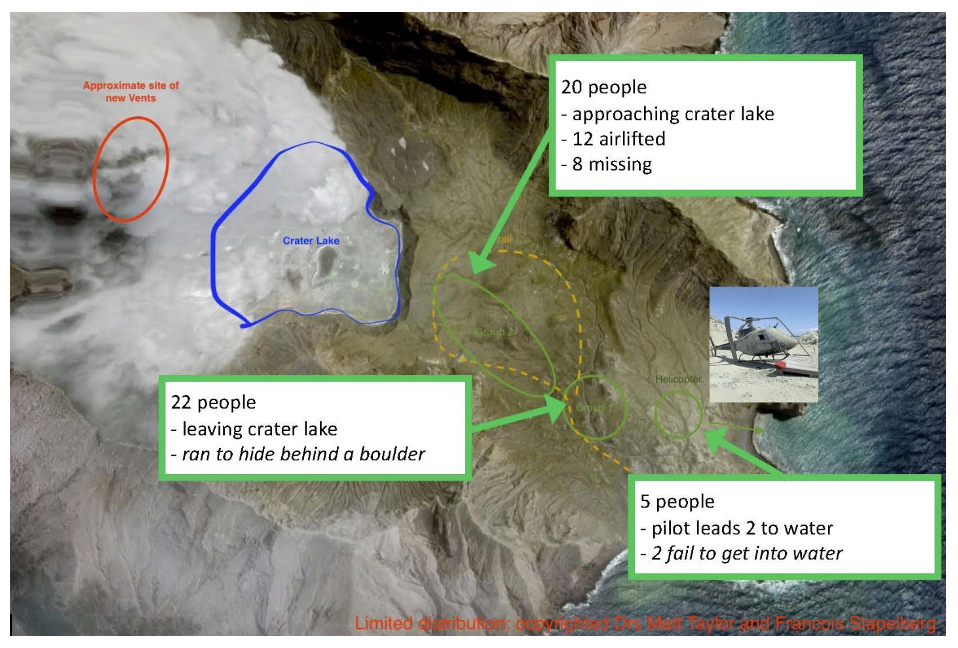
On December 9, 2019 at 14:11 NZDT Whakaari erupted while 47 people were on the island (Figure 1). Eight were missing (and later confirmed dead) while the 39 survivors of the initial eruption were transported back to the mainland. Five died en route and three were largely unscathed, resulting in 31 people needing emergent burn care with an average burn size of 46.3 per cent total body surface area (TBSA).

Burn care in New Zealand is provided in one of four regional plastic surgery units, which are also the regional burn units, located in Auckland, Hamilton, Hutt Valley and Christchurch. The Auckland site also contains the National Burn Centre, which cares for patients with burn injuries greater than 30 per cent TBSA.
There were many lessons gained from this life-changing experience,1 and as the five-year anniversary of this disaster approaches, it is appropriate to highlight some personal lessons from the incident.
Lesson 1—don’t complain—it could get worse
December 9 was the day of the national ‘registrar changeover’ when registrars change specialties, hospitals and often cities. New plastic surgery registrars were being orientated to their hospital and service during the morning. Plastic surgery trainees who had already completed their burn rotation were rotated to a combination of other teams and to other plastic surgery units throughout the country.
On this day the National Burn Centre was already over capacity. For the two months prior to the incident the burn team operative workload varied between 100–200 per cent of the resourced time. In addition, the intensive care unit was full and had no capacity to accept new admissions.
The 31 patients from Whakaari represented approximately a year’s worth of referrals to the National Burn Centre. As the unit was already over capacity, the majority of patients were distributed around the country to the regional burn units, with only four patients being transported to the National Burn Centre.
Over the ensuing days the sheer scale of the disaster became apparent and additional capacity was created at the National Burn Centre and in intensive care. Repatriation of 13 Australian patients to three burn centres across Australia within five days greatly reduced the demand on the New Zealand National Burn Service. In addition to the numerous pre-existing major burn patients, a total of 14 Whakaari patients were eventually cared for at the National Burn Centre.
Table 1 highlights the magnitude of the disaster—a week’s worth of operating was completed on the first day, a month’s worth in the first week and almost half a year’s worth within three months—just in time for the world to become locked down with the global COVID-19 pandemic.
Lesson 2—prepare and plan
New Zealand’s preparation for a major burn disaster began with the establishment of a National Burn Service, consisting of the four regional burn units located within plastic surgery units across New Zealand and the National Burn Centre which opened in 2006 to provide coordinated burn care.
In 2010 a paper from the National Burn Centre was written with the aim to quantify the resource requirements of a major burn patient.2 This paper formed the basis of the 2011 Multiple Complex Burn Action Plan, written as part of the National Health Emergency Plan of New Zealand.3
While these documents highlighted the predicted surge in surgical, nursing and allied healthcare requirements, they failed to take into account the complexity of the patients and the logistical difficulties of caring for multiple concurrent patients. Ultimately, care for Whakaari patients was directed by need rather than being constrained by the predicted model.4
More importantly, in 2018 the training regulations for plastic and reconstructive surgery5 added the requirement for all New Zealand trainees to complete a six-month rotation with the burn team at the National Burn Centre. This meant that via the newly rotated trainees, clinicians with recent experience in managing major burn patients were present in all four centres throughout the country at the time of this incident.
Lesson 3—people are key to success
Success in the coordinated treatment of the 31 patients who entered the New Zealand National Burn Service relied on a diverse team of dedicated people—both clinicians and managers. Although palliation or lowering thresholds of care for those with the most severe injuries would have been an option, the team involved instead went ‘full noise’ on each and every patient—Whakaari and pre-existing—to give each person the greatest chance of survival.
This approach is reflected in the overall survival rate of those who made it into the National Burn Service. Overall, 23 out of 31 survived—74 per cent—the highest reported survival rate for this mechanism of burn injury worldwide.1
Obstacles that normally limited access to theatre and other resources disappeared in response to this disaster. Although there were only four specialist burn surgeons within the department of plastic surgery at Middlemore, all members of the department worked tirelessly to provide care—which was around the clock for the first few days. Support was also recruited from overseas, including not just surgeons, but also nurses and allied health staff. As a result, during this period I had the privilege of operating with both a previous mentor and a previous fellow.
Sir Harold Gillies said in 1926 that ‘the acute burn is not strictly a plastic problem, but to ensure early grafting it was necessary that we gain early control of these patients from the start. This necessitated the development of a team well versed in the physiology and pathology of burns.’6
This philosophy is as relevant today as it was then.
In closing, I am reminded of an inspiring statement that Apple employees receive on day one—‘there is work and then there is your life’s work’.7 On reflection I now realise that my life’s work is not just patient care, but to teach, guide and (hopefully) inspire the next generation of young surgeons to do the most amazing work in the world—to rebuild bodies and to restore lives—and in doing so to become the embodiment of what it is to be a plastic surgeon.