
Introduction
The trapezius muscle is a Type II Mathes and Nahai muscle1 and its vasculature is not routinely preoperatively mapped before raising a myocutaneous flap because it is assumed that perforators will reliably arise from the transverse cervical artery (TCA) or the dorsal scapular artery (DSA). This case report describes the unexpected intraoperative encounter of paraspinal perforators only during reconstruction of an excisional posterior neck defect with a trapezius myocutaneous flap and the freestyle manoeuvres required for salvage. A literature review was conducted to examine the frequency of this variance; however, this is the first reported case of a trapezius myocutaneous flap with dominant paraspinal perforators.
Case
A 67-year-old man with a large, ulcerative, posterior neck, biopsy-confirmed basal cell carcinoma (BCC) presented after five years of slow growth. He was an actinopath, having undergone many previous excisions of non-melanoma skin cancers, all with clear margins.
Initially on review, the lesion in question was situated on the right posterior neck just below his hairline and measured 53 × 40 mm. Clinically, there was an additional non-tender, palpable lump around level VB in the right neck. At the time, this was suspicious of either a nodal metastasis or an extension of the lesion into the adjacent neck muscles.
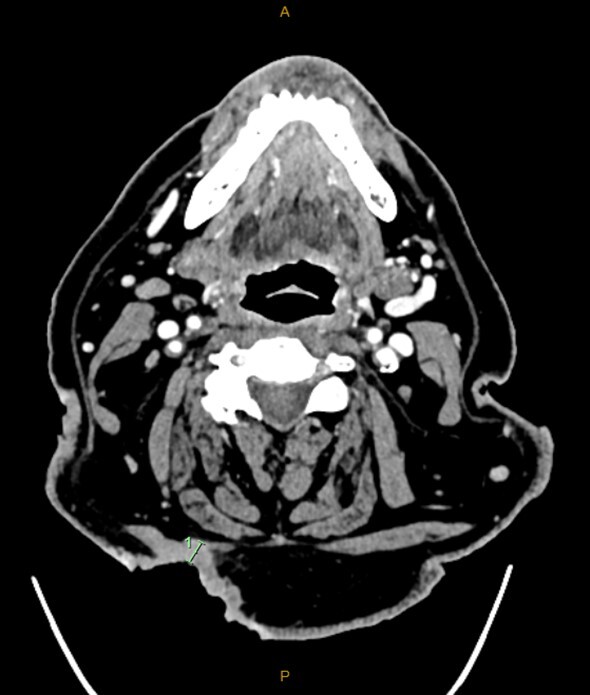
A computed tomography (CT) scan performed to evaluate the extent of the lesion showed the lesion invading the patient’s right splenius capitis and upper trapezius muscles (Figure 1). A radiographically suspicious level VB lymph node correlated with the examination findings, but it was difficult to ascertain whether this was contiguous or lymphovascular spread. Histology from a subsequent ultrasound-guided aspiration of this node was strongly suggestive of metastatic BCC.

The case was discussed in a multidisciplinary meeting and the resulting consensus was for primary surgical excision of the lesion with an ipsilateral level V neck dissection. Due to the site of the tumour and the required intraoperative position for primary resection, the proposed reconstruction was with an ipsilateral pedicled trapezius myocutaneous flap.
The tumour was excised en bloc with the splenius and part of the upper trapezius muscle, along with the level V lymph nodes. The TCA was seen to be protected, entering the patient’s back after travelling deep below the levator scapulae muscle. The completeness of the resection was confirmed from frozen sections.
Preoperatively, the excision margins, flap and perforators were identified and marked using Doppler ultrasound (Figure 2). The trapezius myocutaneous flap was raised as per the markings—around the superior/middle areas of the muscle—with the presumption that this tissue would be perforated by the TCA. Intraoperatively, the vascular supply of the trapezius muscle was seen to predominantly arise from two paraspinal perforators. These were both larger in size and longer in length than typically encountered, measuring about 8 cm each. These perforators originated at the T6 and T8 vertebrae and travelled cranially to supply the entire trapezius muscle. The TCA was found to supply only a few of the most cranial fibres of the trapezius muscle before travelling underneath to supply the rhomboid muscles, with no further caudal tributaries to the trapezius.

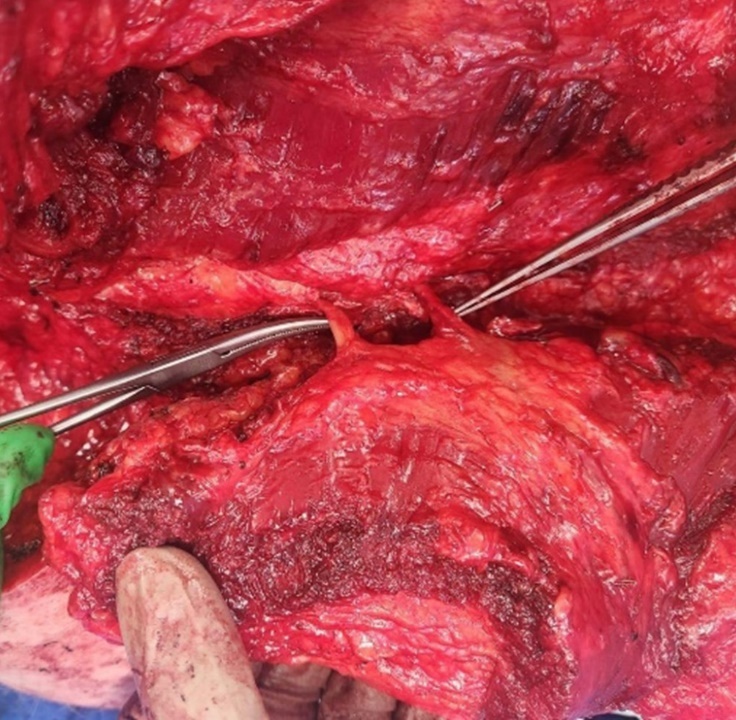
The excised flap was not deliverable to the defect using the traditional pedicled approach. Attempts at a propeller flap modification based on the larger of the two paraspinal perforators resulted in unviable flap congestion, requiring the flap to be straightened back into its original position. This aberrant anatomy required adoption of a free flap design supplied by a dominant paraspinal perforator (Figure 3). The flap was harvested based on the identified larger paraspinal perforator after an on-table revision of the plan. The anomalous TCA and associated vein in the neck were used as the recipient vessels. There was good immediate flow across the anastomoses and the flap was well perfused.

The postoperative course was uneventful with standard postoperative free flap care and the patient was discharged on postoperative day seven.
Discussion
The trapezius myocutaneous flap is a mainstay option available to reconstructive surgeons for defects on the posterior scalp and neck.2,3 Specific advantages offered by this flap are its reliable vascular anatomy, the length of reach achievable with a pedicle, no requirement for an intraoperative patient positional change, and a donor site that is hidden and minimally morbid.1,4,5
The trapezius muscle arises from the superior nuchal line and C7–T12 spinous processes, and attaches to the posterior border of the lateral third of the clavicle, acromial process and spine of scapula. It is classified as a Type II Mathes and Nahai muscle, with the dominant vascular pedicle classically arising from the TCA. It has been noted that the lower part of the muscle is classified as a Type V Mathes and Nahai muscle, due to segmental intercostal perforators permitting a turnover flap.3 Other, minor vascular pedicles arising from the occipital artery and posterior intercostal artery are also described.1
However, over the last few decades cadaveric dissection and data collection has demonstrated that the dominant perforators to the trapezius flap equally and predominantly arise from the TCA or the DSA. The supply from intercostal or paraspinal arteries has always been documented as a minor pedicle for this flap, used only for the inferior half of the muscle itself.1,6
We searched Cochrane, MEDLINE and PubMed library databases using the keywords ‘trapezius flap’, ‘perforator’ and ‘paraspinal’ OR ‘intercostal’ between 1990 and 2024 for English publications. Inclusion criteria were articles detailing the use of a trapezius flap with dominant paraspinal pedicles in human patients.
This search resulted in one case report by Mardini and colleagues in 2004,7 who used a free lower-trapezius flap to reconstruct a lower limb defect based on intercostal perforators. This case, however, described the need to ligate the DSA as well as supplying perforators arising from the TCA. Articles excluded after scrutiny involved two case series that involved trapezius muscle/myocutaneous flaps with a latissimus dorsi component—known to have intercostal perforator dominance—and a cadaveric case series in dogs, due to practical applicability.
Classified as a Type II muscle, the vascular supply of the superior half of the trapezius muscle is not routinely preoperatively radiographically mapped—as was the case here. We organised a postoperative CT angiogram to determine if the contralateral side demonstrated this abnormality and if there would have been any preoperative benefit in radiological vascular mapping. These scans were unfortunately inconclusive, demonstrating postoperative changes that obscured the arteries of interest with poor resolution of these vessels even on the contralateral side.
Conclusion
This report demonstrates the first case of a trapezius myocutaneous flap planned for head and neck reconstruction with a dominant paraspinal perforator and no significant TCA supply. The modified free flap design safely used for reconstruction is also described. While having known segmental supply from the TCA and DSA and, more inferiorly, intercostal perforators, no documented record of a predominant intercostal or paraspinal supply was found after a review of the literature, to the best of our knowledge.
Teams involved in reconstructive efforts need to acknowledge the rare individual anatomical variations within this flap, despite classical dogmatic description, and any subsequent modification to the intraoperative approach that this may require.
This case demonstrates the robustness of the trapezius flap and the potential for its conversion to free flap design as an option, if required, within reconstructive efforts.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship and/or publication of this article.