Introduction
Australian rules football is characterised by high-intensity gameplay and physically demanding actions. The nature of the sport predisposes players to injuries such as fractures, dislocations and ligament sprains. Though sports injuries are widely covered in the literature, research on hand injuries related to the sport’s focus on ball handling remains limited.1–4
Recent data indicates that injury patterns, severity and recovery can differ significantly between male and female players. Female athletes are more susceptible to specific injuries due to anatomical and physiological factors, including ligamentous laxity and hormonal influences.5,6 This trend has also been observed in Australian rules football, where injury profiles between genders differ in frequency, mechanism and outcomes.5,7 However, specific data on hand injuries in Australian rules football, particularly regarding gender differences, is sparse.
Hand injuries can have a profound impact on a player’s ability to participate and perform, as well as on their overall quality of life.8,9 These injuries often require specialised management, ranging from conservative treatments to complex surgical interventions. The limited research on managing hand injuries in Australian rules football players hinders the development of effective prevention strategies and evidence-based treatments.6 A lack of understanding regarding differences between male and female players, especially in injury mechanisms, treatment options and long-term outcomes, complicates care for athletes.
This study aims to describe differences in hand injuries among male and female Australian rules football players through a cohort analysis. By examining injury patterns, operative interventions and complication rates, this research seeks to provide insight into potential differences between the sexes. While not powered to support definitive statistical conclusions or guide gender-specific management, the findings may contribute to a broader understanding of injury profiles in community-level Australian rules football.
Methods
This retrospective cohort study included all patients with Australian rules football-related hand injuries who presented to the emergency department at Frankston Hospital in Melbourne, Australia, between January 2021 and August 2024. The three-year audit covered three Australian rules football seasons, including pre-season training and practice matches. Ethics approval was obtained from Peninsula Health—approval number QA/112259/PH-2024-447217(v1).
Patient medical records were reviewed retrospectively using data from the hospital’s plastic and hand surgery registry, which tracks hand injuries related to Australian rules football. Data extracted included:
-
demographics—age, gender, playing position, hand dominance
-
injury-related information—mechanism of injury, location and type of fracture (single or multiple) or dislocation injury
-
treatment details—type of operative management and rehabilitation protocols, including hand therapy
-
outcome data—postoperative complications (infections, delayed healing), recovery times, duration of follow-up.
All data was deidentified and securely stored in compliance with ethical guidelines. The results aim to assess and identify gender-specific trends in injury and outcomes.
Results
A total of 46 Australian rules football players (36 males and 10 females) were included in the study, with demographic details summarised in Table 1. In examining fractures between males and females, specific differences in frequency are notable, though they often lack statistical significance. For the right ring finger metacarpal, males and females both had one fracture (2.8% and 10% respectively). More notable is the right little finger proximal phalanx fracture, observed in seven males (19.4%) and five females (50.0%). However, for the left little finger proximal phalanx fracture, five males (13.9%) and one female (10.0%) sustained injuries (Figure 1).

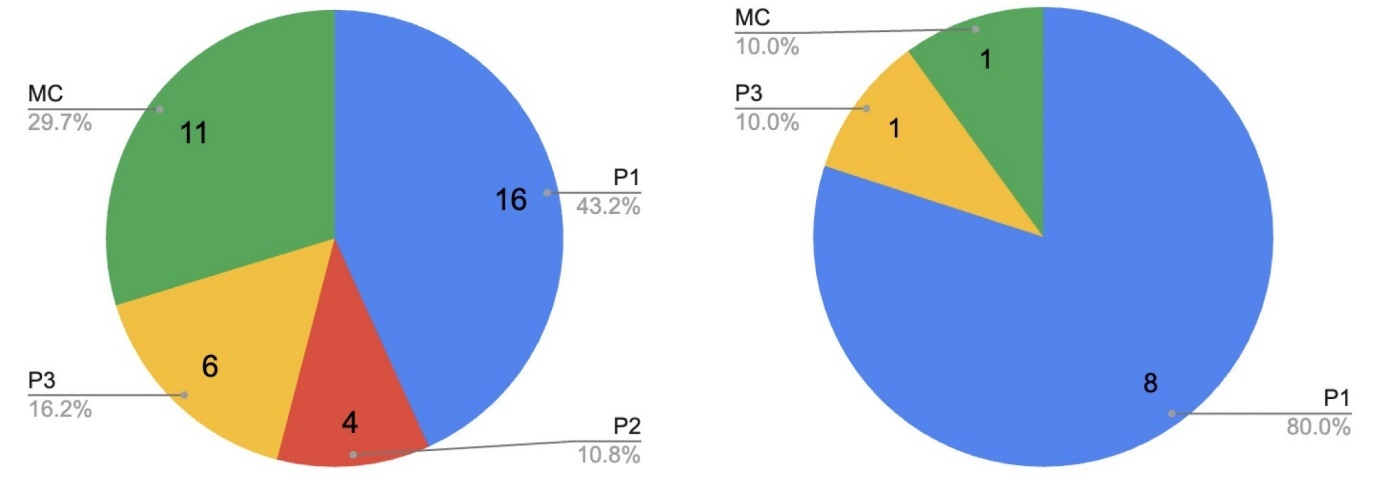
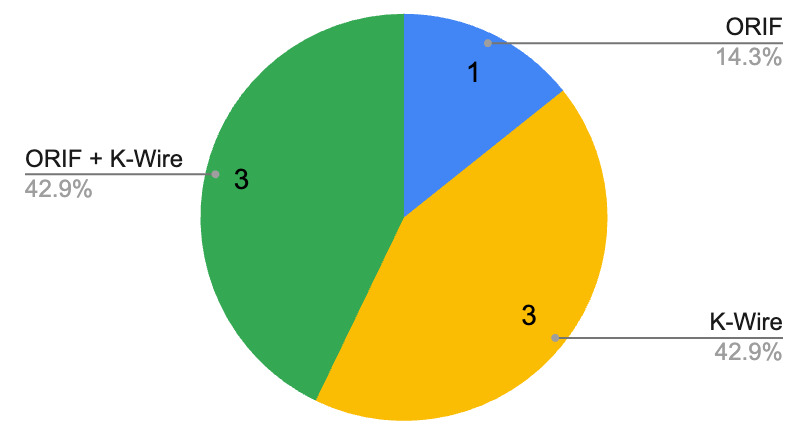
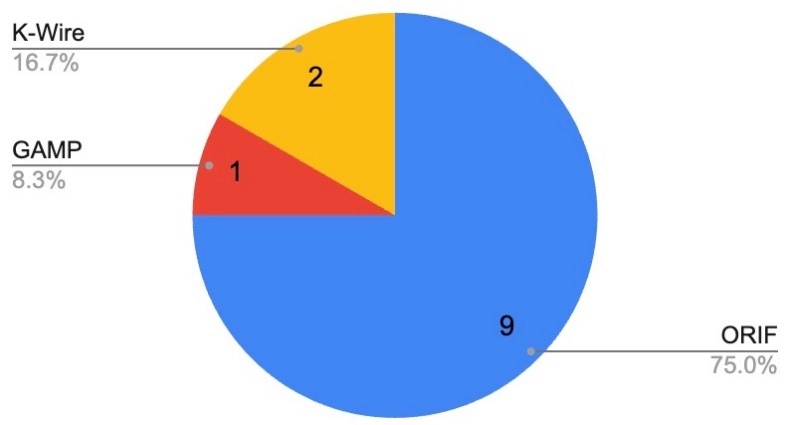
The analysis of surgical operations reveals similar usage rates across genders for standard fracture treatments. Open reduction internal fixation (ORIF) was performed in 20 males (55.6%) and six females (60.0%). General anaesthetic, manipulation and plaster (GAMP), another intervention, was slightly more frequent in females (20.0%) than males (11.1%). Procedures combining ORIF and Kirschner-wire (K-wire) were performed in three males (8.3%) and one female (10.0%), and K-wires alone were used in four males (11.1%) and one female (10.0%).
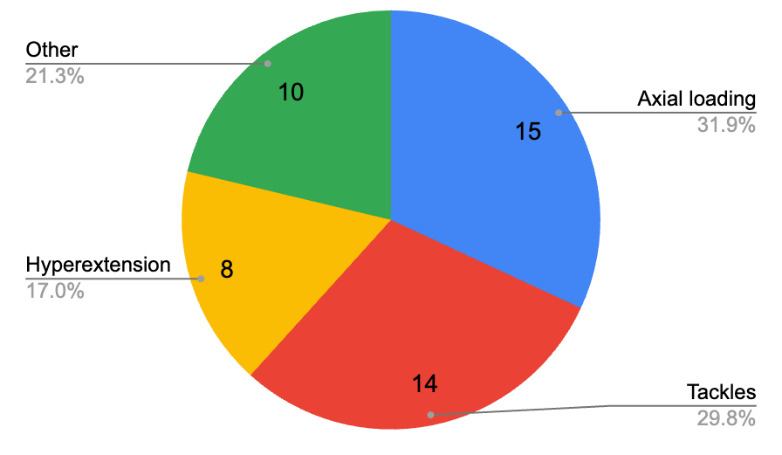
When evaluating mechanisms of injury (Figure 2), males and females displayed varying injury patterns. Tackling was a prevalent cause of injury among males, with 13 cases (36.1%) versus one case in females (10.0%). Axial loading injuries were similarly frequent in males (30.6%) and females (30.0%). Notably, females were more likely to suffer injuries from being trampled, with two cases (20.0%) compared to none in males. Males predominantly sustained axial loading injuries, whereas females more often experienced hyperextension and trampling injuries.

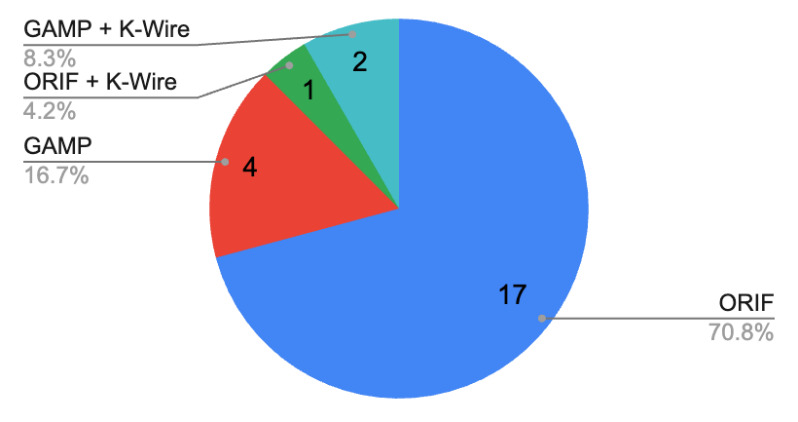
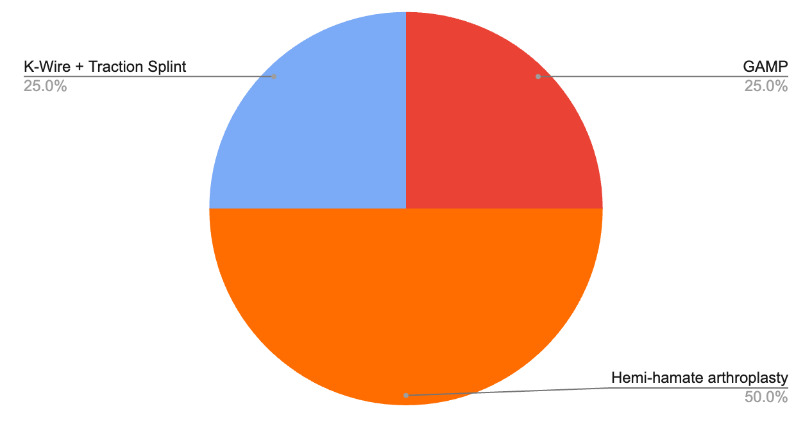
Although infrequent, hyperextension-related injuries from kicking and smothering also appeared slightly more common in females. These variations highlight certain injury mechanisms that may disproportionately affect each gender within this context. See Table 2 for a breakdown of injury locations and their management. The treatment patterns by bone are shown in Figures 3, 4, 5 and 6.




Discussion
Our results demonstrate that males frequently sustain injuries from axial loading forces, typically caused by high-impact events such as tackling or ball handling. In contrast, female players were more prone to hyperextension injuries, likely associated with less direct impact but more overstretching of hand structures. These gender-specific differences are consistent with previous studies in other sports, such as basketball and soccer, where male athletes are more susceptible to high-energy trauma. In contrast, female athletes are prone to injuries related to joint laxity and overextension.10–12 This aligns with studies that highlight female athletes’ increased susceptibility to hyperextension injuries due to anatomical differences, such as ligamentous laxity and hormonal influences.10–14
The decision to proceed with ORIF in both males and females appeared broadly similar. However, operative decision-making is multifactorial and may reflect factors such as fracture configuration, patient compliance, preferences and surgeon discretion rather than injury severity alone.15,16 However, slightly more females were found to require ORIF in our cohort, which aligns with Grawe and colleagues’ study, highlighting that factors other than trauma severity, such as fracture type and the use of locked plating, may influence surgical decision-making.17 While males encountering more direct trauma often present with more displaced fractures that require surgical correction for proper alignment and functional recovery, the decision to use ORIF may be driven by fracture complexity rather than gender or trauma severity alone.18,19
The overall complication rate was slightly higher in females (10.0%) compared to males (5.6%), though complications like osteomyelitis and ulnar numbness were relatively rare. Despite differences in management strategies, complication rates were similar between genders, indicating that surgical and conservative approaches were practical when applied appropriately. While none of the ORIF patients in this cohort experienced complications, the sample size is small, and this finding should be interpreted with caution. In contrast, three cases with complications occurred in those who had K-wire fixations, a result that differs from most findings in the existing literature.20–22
Recovery times and the need for hand therapy varied, with females generally requiring longer rehabilitation. This may reflect physiological differences such as bone density or ligament healing properties, although this was not directly assessed in our study. Prior research has shown that female athletes often experience longer recovery times due to factors such as lower muscle mass and slower ligamentous healing, which can impact rehabilitation protocols.23 Additionally, the smaller bone size and lower bone density in females might contribute to the need for extended therapy to achieve optimal functional recovery.23 The younger average age in the female cohort may also reflect differences in experience, which could influence injury mechanisms; however, this relationship requires further exploration.24,25
Regarding injury location, the proximal phalanx was most frequently fractured, followed by the distal and middle phalanges. This distribution aligns with previous studies indicating that fractures in the proximal phalanx are more common due to its exposure to impact forces. The treatment and complication rates reflect the severity of injuries, with ORIF being favoured for its effectiveness in managing complex fractures.
The notable age difference between the male and female groups likely influences the variation in injury patterns observed. Males, with an average age of 22, benefited from more experience, which may explain their higher rates of tackle-related injuries. In contrast, females, with an average age of 17, were more susceptible to hyperextension injuries, potentially due to being less experienced.26–29 Additionally, this age gap may reflect the increasing participation of younger females in sports. However, it also highlights a drop-off in involvement as they age, resulting in comparatively few 22-year-old females playing. Thus, age-related physiological and experiential disparities may help explain the observed differences in injury types between the two groups.
The literature on Australian rules football injuries has predominantly focused on lower limb issues, especially anterior cruciate ligament tears, which are more common in female athletes. However, hand injuries, crucial for tasks such as ball handling, passing, and tackling, have received less attention. This study underscores the importance of understanding gender differences in injury mechanisms for sports that require significant hand use, like Australian rules football. Hand injuries can severely impact a player’s performance (affecting core game aspects such as marking and tackling) and quality of life. Our findings highlight the need to balance attention between lower and upper limb injuries, emphasising the importance of prioritising hand injury prevention and rehabilitation in Australian rules football research.
While differences in injury patterns and recovery times were observed, the small cohort size limits the ability to draw firm conclusions. These preliminary findings may prompt further investigation into whether sex-specific prevention strategies are warranted in larger, more representative samples. For male players, focusing on strength and conditioning programs that reduce the risk of high-energy trauma may be beneficial. In contrast, female players could benefit from neuromuscular training to enhance joint stability and minimise the risk of hyperextension injuries. Comparisons with previous literature on gender-specific injury prevention strategies support the notion that such interventions should be sport-specific and account for the distinct biomechanical demands placed on male and female athletes. It is important to note that treatment differences between male and female athletes in the literature may also reflect systemic biases in clinical decision-making rather than purely biological differences. Our study did not explore provider-level factors, and future research should consider this important dimension.
Although this study provides valuable insights into gender differences in hand injuries among Australian rules football players, it has limitations. As a retrospective analysis, the study relied on the accuracy and completeness of medical records, which may introduce some selection bias. Additionally, while we adjusted for factors such as age and hand dominance, other potentially influential variables, such as player position and level of competition, were not accounted for. Future research with larger, prospective cohorts could help validate these findings and provide a more comprehensive understanding of the factors contributing to gender-specific injury outcomes in Australian rules football.
Conclusion
This study demonstrates significant gender differences in the mechanisms, management and recovery outcomes of hand injuries in Australian rules football players. These findings highlight the need for gender-specific injury prevention and rehabilitation programs to optimise player safety and recovery. By tailoring treatment approaches based on gender, sports medicine professionals and hand therapists can improve outcomes and help athletes return to optimal performance levels more effectively. This study adds to the growing recognition that injury prevention and management in contact sports must consider gender as a critical factor.
Practical implications
-
Gender influences the mechanism, management and recovery outcomes of hand injuries.
-
Prevention strategies for male players should focus on strength and conditioning programs that reduce the risk of high-energy trauma.
-
Prevention strategies for female players should focus on neuromuscular training to enhance joint stability and minimise the risk of hyperextension injuries.
-
Interventions should be sport-specific and account for the distinct biomechanical demands placed on male and female athletes.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship and/or publication of this article.
Revised: June 9, 2025 AEST