













The story
Upon reflecting over the last 50 years of microsurgical free tissue transfer and our various contributions to this exciting period, the free fibula flap has been a highlight. This procedure has revolutionised the management of major congenital and acquired bone defects in the extremities and become the gold standard for jaw reconstruction. It has been a trifecta of original techniques to transfer the bone—at first the diaphysis was transferred on the peroneal vascular pedicle, next the anterior tibial stalk, and finally the proximal growth epiphysis on this latter vessel and especially its recurrent genicular branch.
Russell was the registrar at Preston and Northcote Community Hospital (PANCH) when Graeme Miller, Frank Ham and Ian did the first successful free vascularised bone flap transfer in June 19741 using the fibula. Then, since Russ spent a couple of years at Frenchay in Bristol, we have been ‘Zig and Zag’, working together on nearly every free tissue transfer.
What follows is the chronology of events. The development of our techniques, innovations and pitfalls are highlighted and recommendations are summarised at the end. So settle down with a good red! Watch out for what Russ would call a touch of ‘fulminating metaphoria’ and read on!
Case 1: the peroneal pedicle
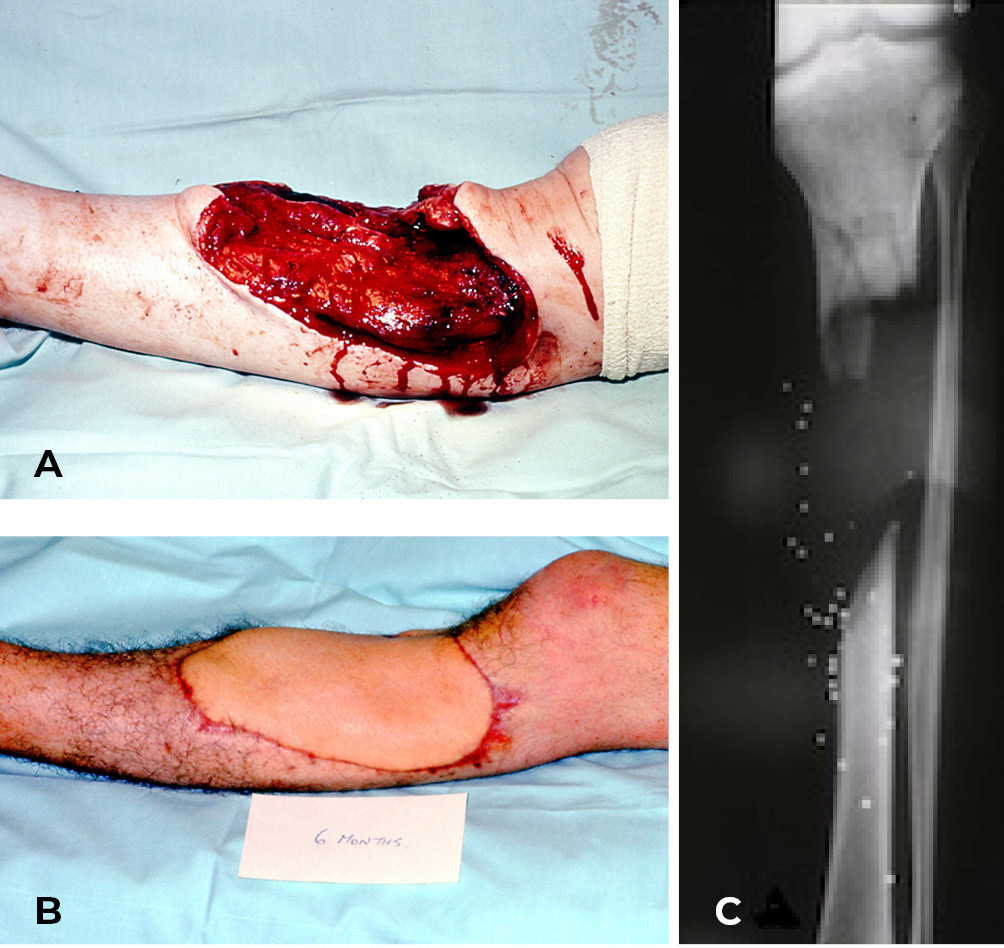
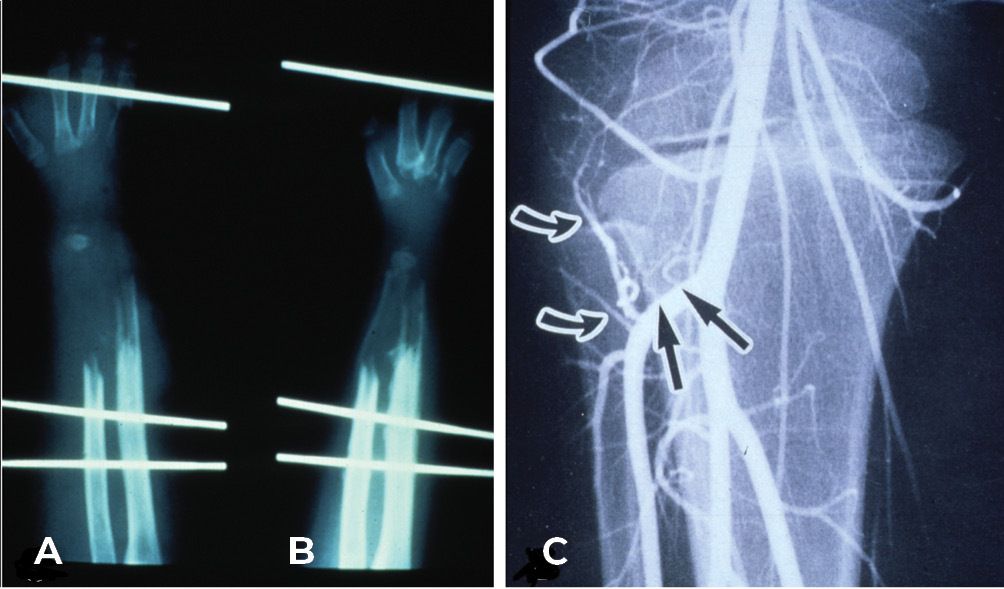
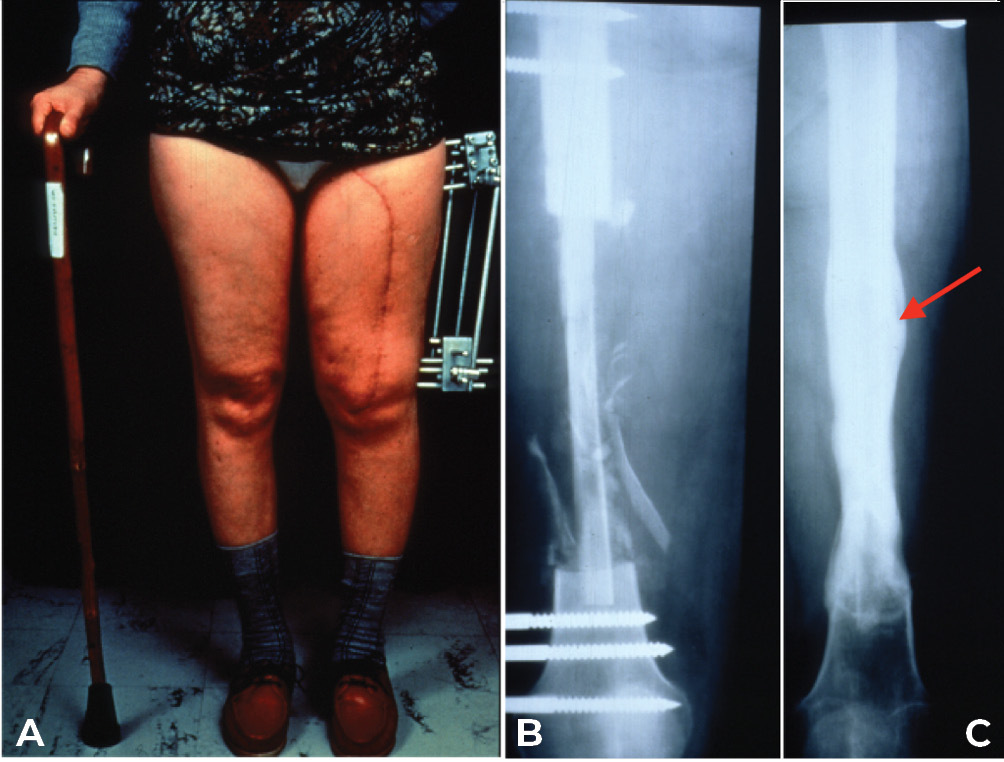
On 20 January 1973 the free groin flap was transferred successfully at PANCH for the first time.2,3 One week later, a 19-year-old young man was admitted to the same hospital with a shotgun injury to his left leg (Figure 1A). The wound included skin, most of the anterior muscle compartment and a 12.5 cm defect of the tibia (Figure 1C).
The foot was sensate and the fibula was intact. So we set about reconstruction. The defect was debrided, healed initially with a split skin graft and then a free groin flap was attempted but abandoned because the groin vessels were very small and the recipient anterior tibial vessels badly damaged. However, because we had performed a lateral to medial dissection of what was now an expanded iliofemoral flap,2 that included the superficial inferior epigastric as well as the superficial circumflex iliac vessels, we were able to tube the flap and transfer it in stages to the leg (Figure 1B).
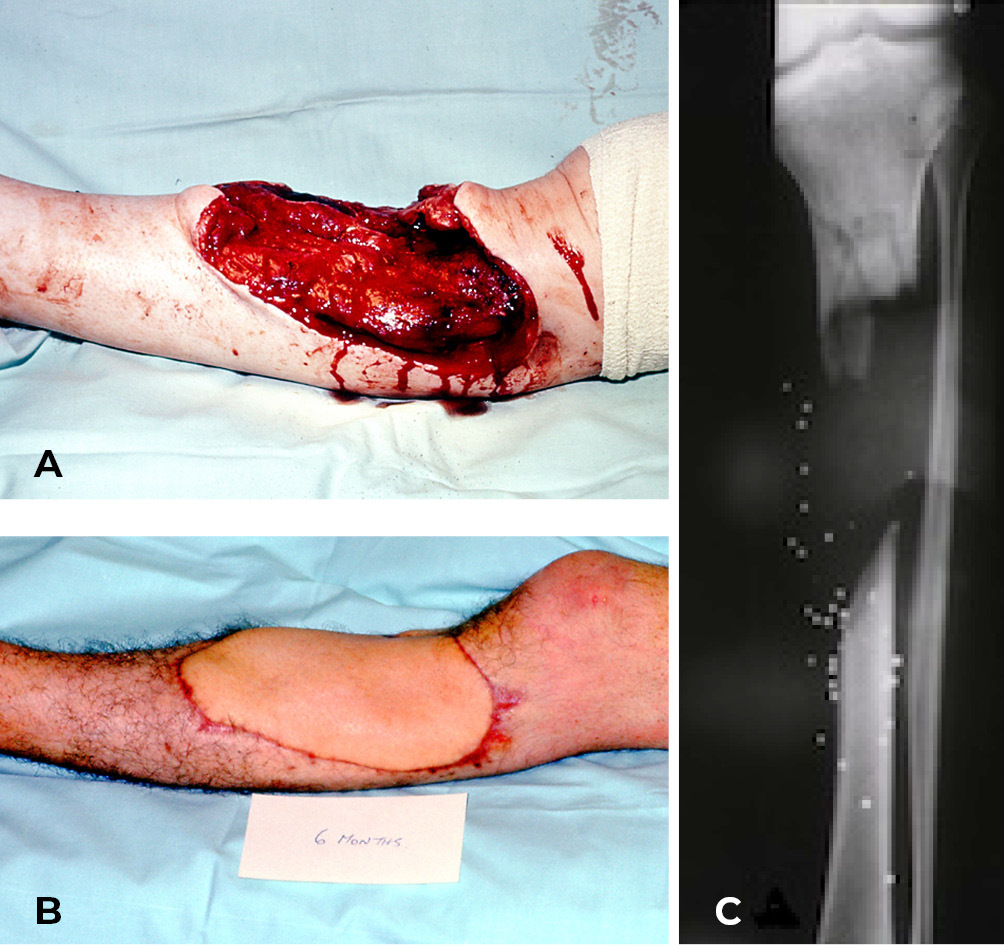
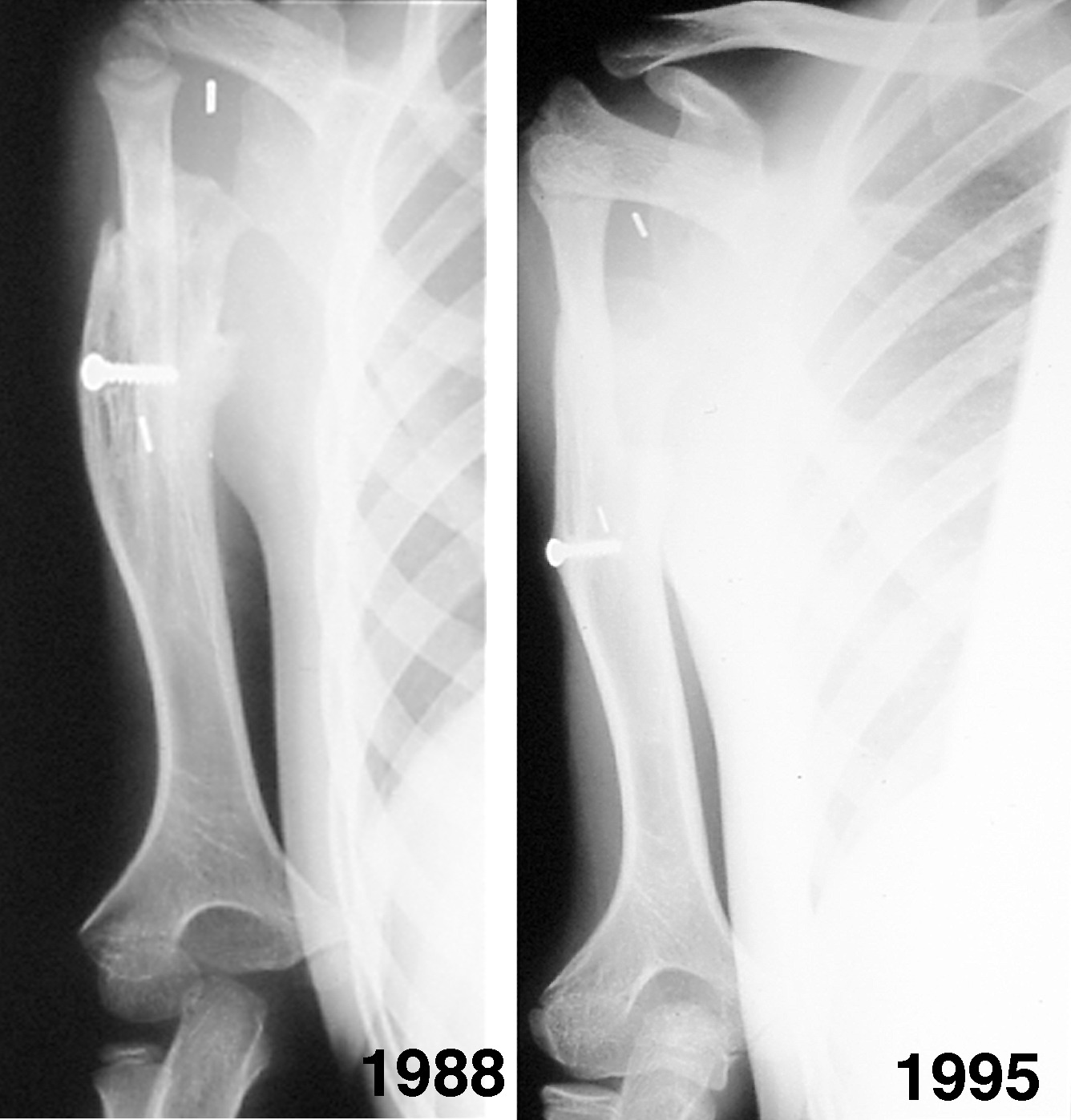
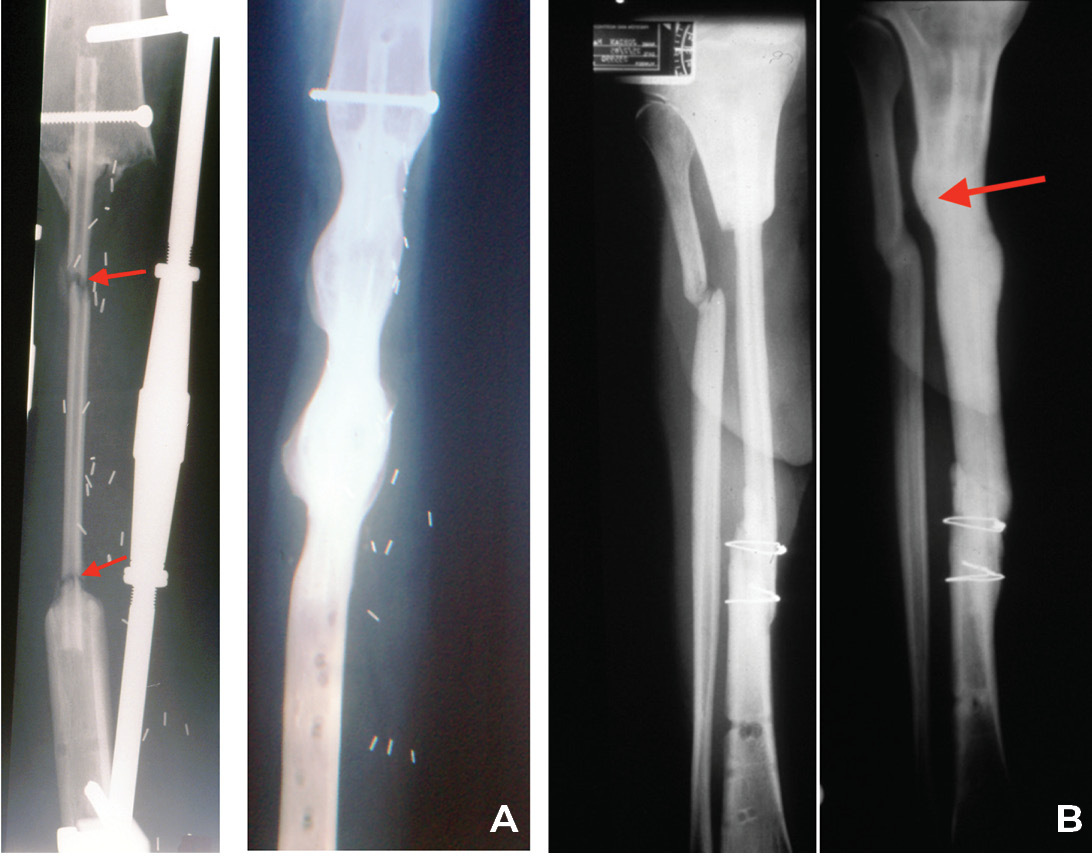
A two-stage transfer of the ipsilateral fibula was then attempted by our orthopaedic team, based on a muscle pedicle and fixed to the tibia with screws. Unfortunately, the bone failed to knit at the upper end. It developed a pseudarthrosis and the patient was left with a flail leg (Figure 2). Amputation was recommended but ‘if a skin flap can be transferred successfully with microsurgery why not bone, and which one?’
Down to the post-mortem room at the Royal Melbourne Hospital where previously we had been able to do our preliminary dissections and redesign the groin flap. First the rib. Long enough but too frail and curved. Next the iliac crest dissected on the deep circumflex iliac artery (DCIA). Good vessels but bone too short. Finally, attention was focused on the fibula. Harry Crock had written a book on the blood supply of the leg bones.4 Ian consulted Harry who said that if the nutrient artery to the fibula could be anastomosed it would be sufficient to nourish the entire shaft of the bone via the upper and lower branches that extended along the full length of the medullary cavity. This was examined but it was tiny (0.5 mm) and short (1.2 cm). However, Ian found that not only (i) did it arise from the peroneal artery paralleled by venae comitantes but (ii) this large peroneal vessel sent branches to the periosteum of the fibula, arising at regular intervals along the shaft, that formed a rich interconnecting lattice that hugged and surrounded the bone. They could be preserved by including a thin cuff of attached muscle. Now we had a long bone with a lengthy pedicle of large vessels. Why not?
The preoperative planning involved three steps:
-
Literature reviews: these found that Leif Ostrup had transferred a rib successfully to reconstruct the jaw in a dog using microvascular surgery.5
-
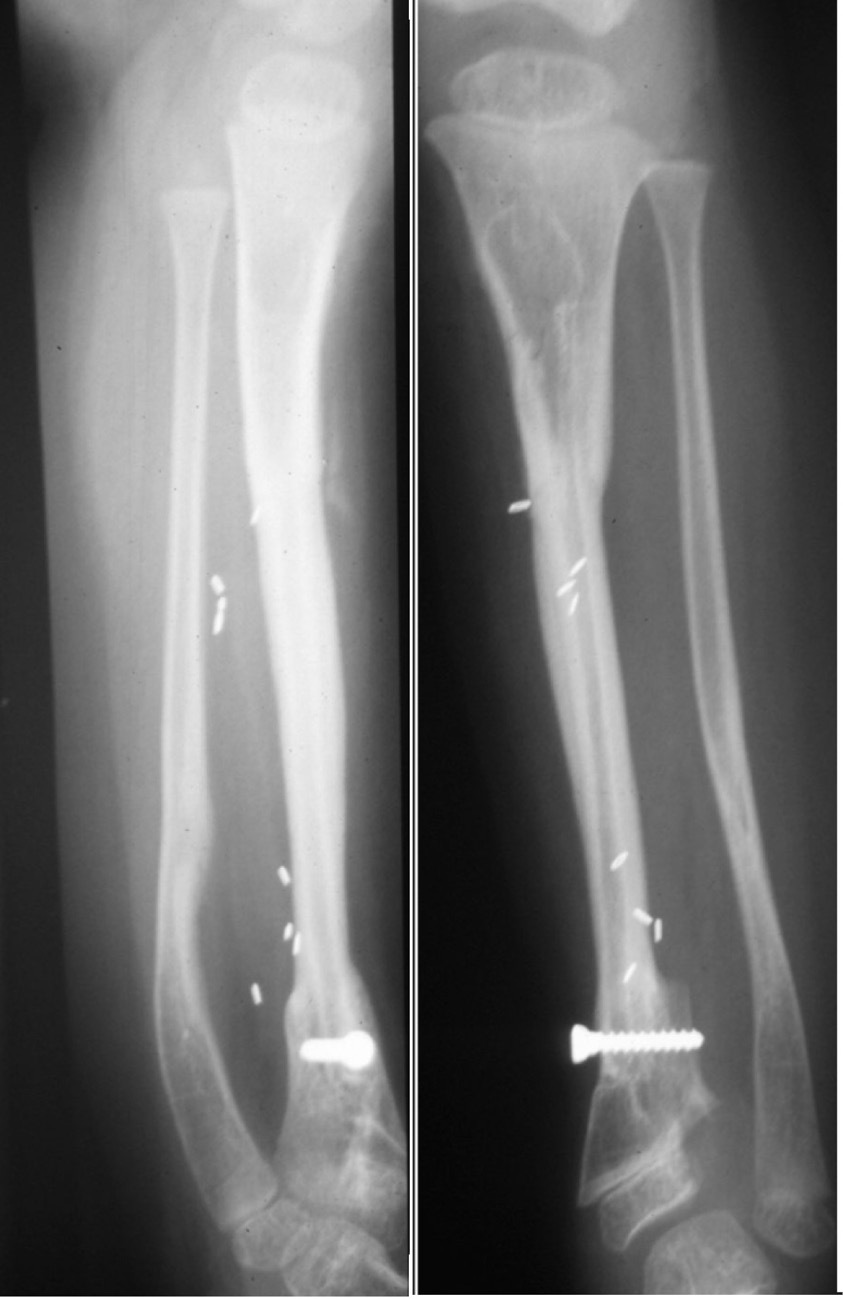
Angiography of the patient’s legs: this revealed suitable vessels for transfer. The donor right leg had a normal three-vessel supply from the peroneal, anterior and posterior tibial vessels. The other leg had intact posterior tibial and dominant peroneal vessels supplying the foot. The former was selected for reanastomosis.
-
Rehearsal in the mortuary: the defect was recreated in the left leg and the fibula was dissected in the other with its peroneal pedicle. We found that if the head of the fibula and the distal quarter of the shaft were left for knee and ankle stability then this would provide a 22 cm length of the fibula diaphysis to transfer, more than enough to repair the tibial defect.
This practice of preoperative angiography and team rehearsal, usually the day prior to surgery, would become the mainstay for all microsurgical procedures.
The operation was performed on Saturday, 1 June 1974. While most of Melbourne was applauding Billy Picken take the ‘Mark of the Year’ for Collingwood against Richmond, our team gathered together quietly in the Victorian Plastic Surgery Unit at PANCH. In one theatre surgeons Ian, Frank Ham, Graeme Miller, and registrar Russ. In the other theatre for reference, right and left cadaver above-knee amputation stumps—one dissected to display the donor fibula, the other the recipient posterior tibial vessels. The anaesthetist was Gordon Leckie—he had ‘volunteered’ after surviving our first free flap. The theatre nurse Jill Storch, our iron lady in charge to control this ‘armful of bullfrogs’.
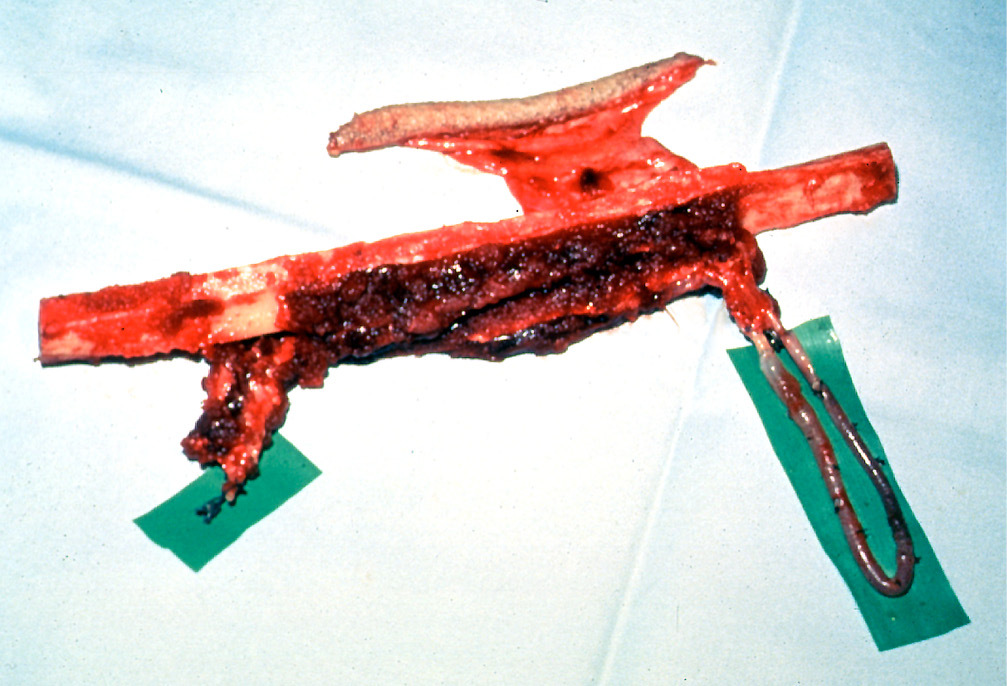
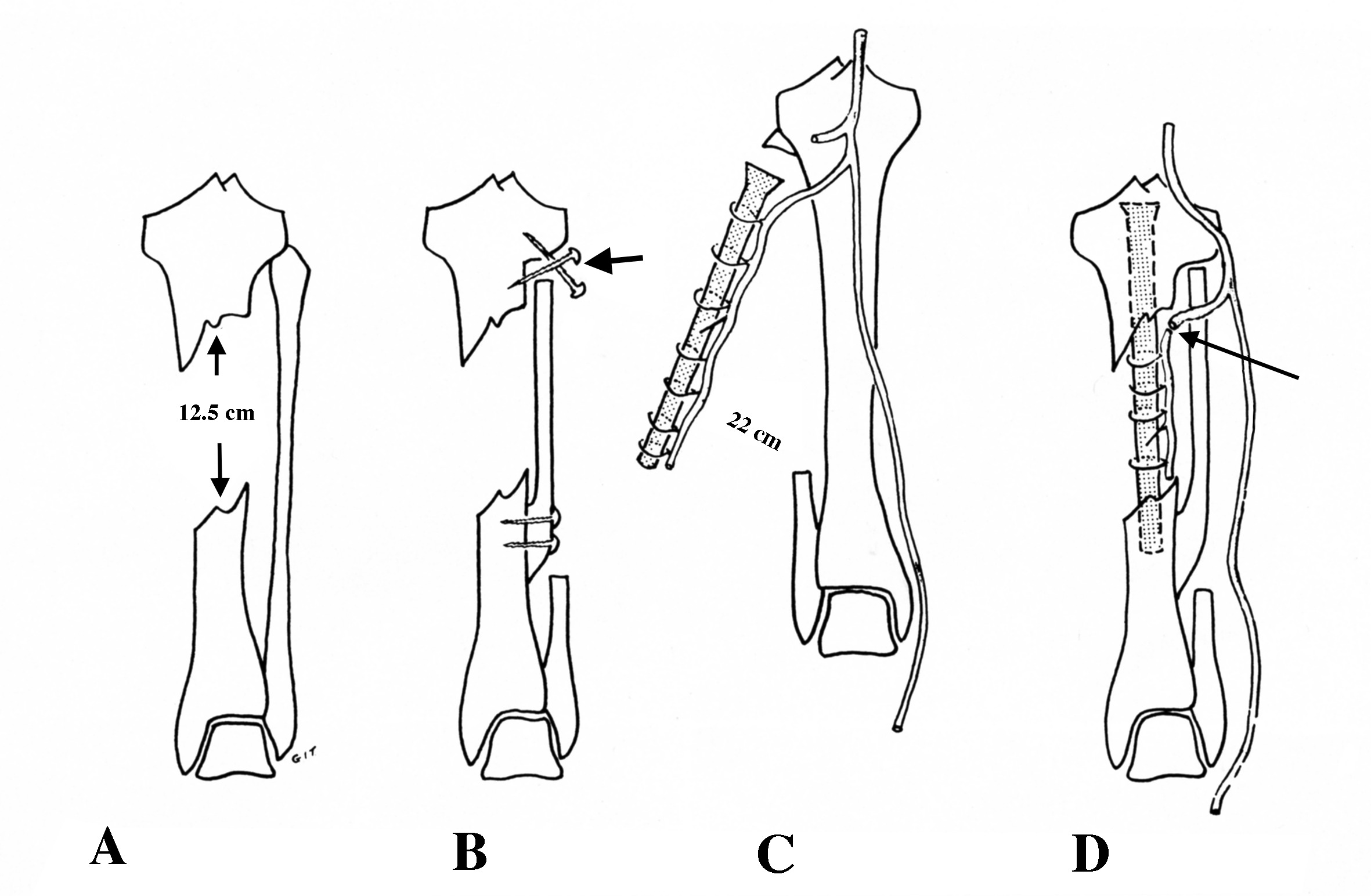
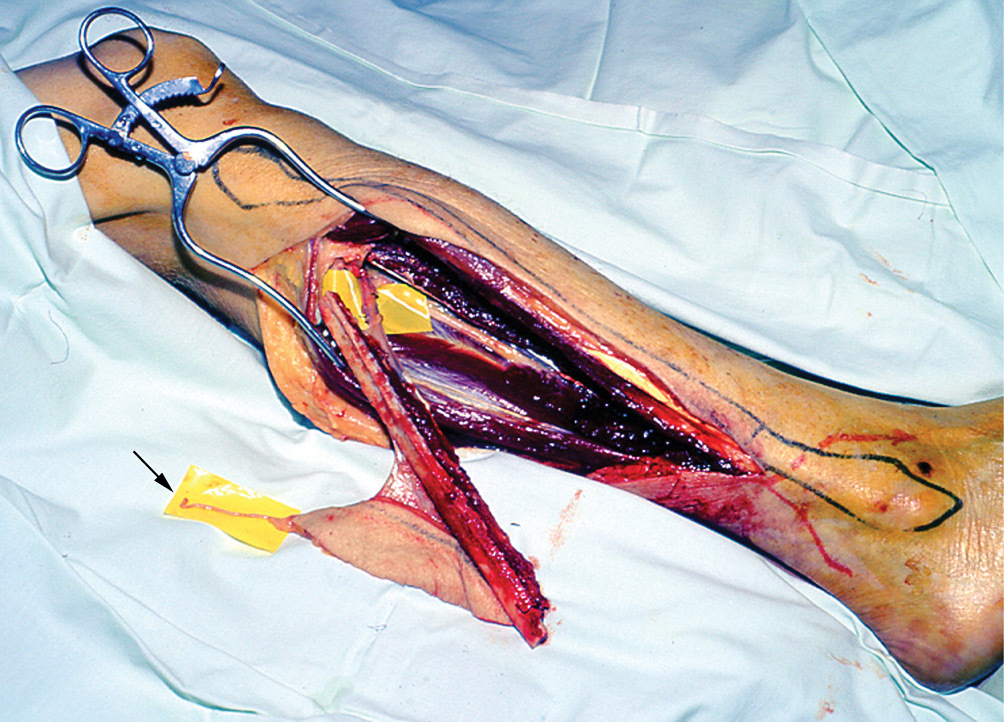
With the patient prone, the legs were dissected simultaneously under tourniquet via posterior incisions. The fibula with a 1 cm cuff of muscle was raised on the peroneal vessels in the right leg. The recipient posterior tibial vessels were dissected in the left leg and a vascular clip was applied to the artery. Tourniquets were released in sequence. Bright bleeding was evident from the muscle cuff, periosteum and medulla of the donor fibula (Figure 3). A normal flow to the foot was noted to the recipient leg, now supplied by just the peroneal artery.

The fibula was detached and dowelled first into the proximal end of the tibia and fixed with screws. A ‘dovetail keystone’ of bone was removed from the tibia distally to obtain access to the medullary cavity for insertion of the fibula, then replaced and fixed with screws. The peroneal vessels were anastomosed end-to-end to the posterior tibial artery and its venae comitantes. Bright bleeding was seen again from the muscle sleeve around the fibula! Bloody fantastic!
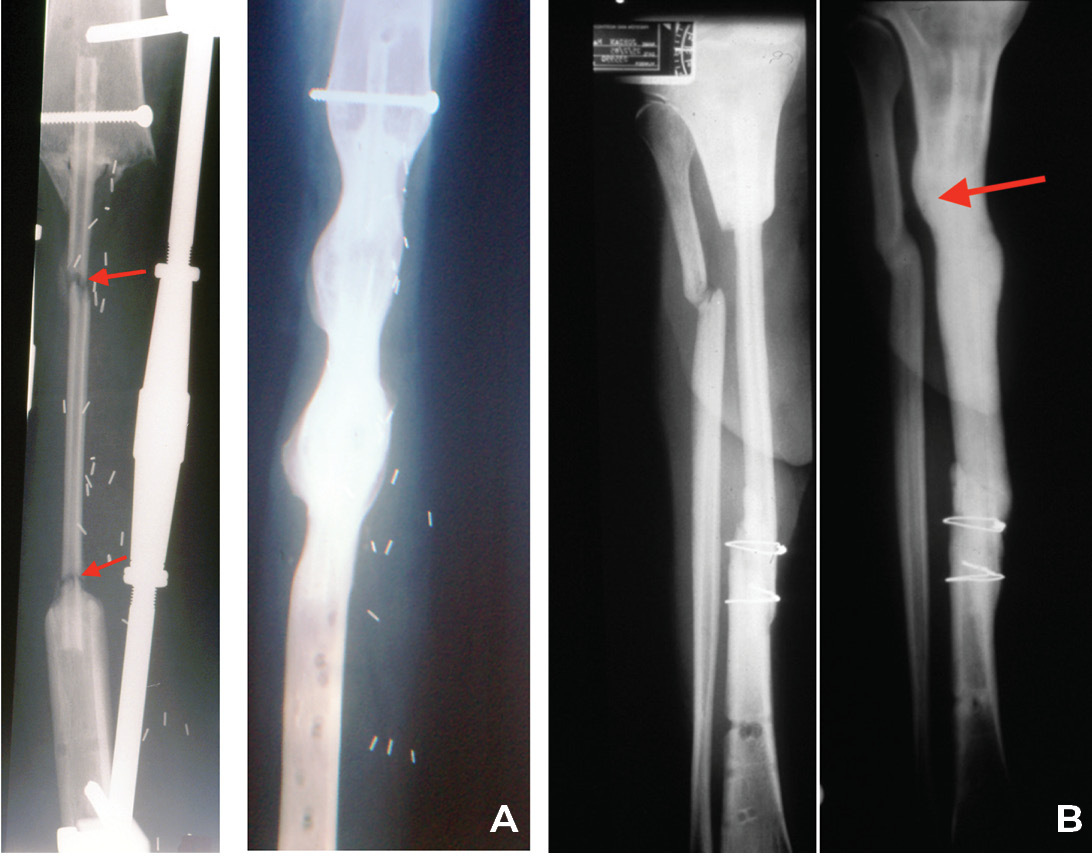
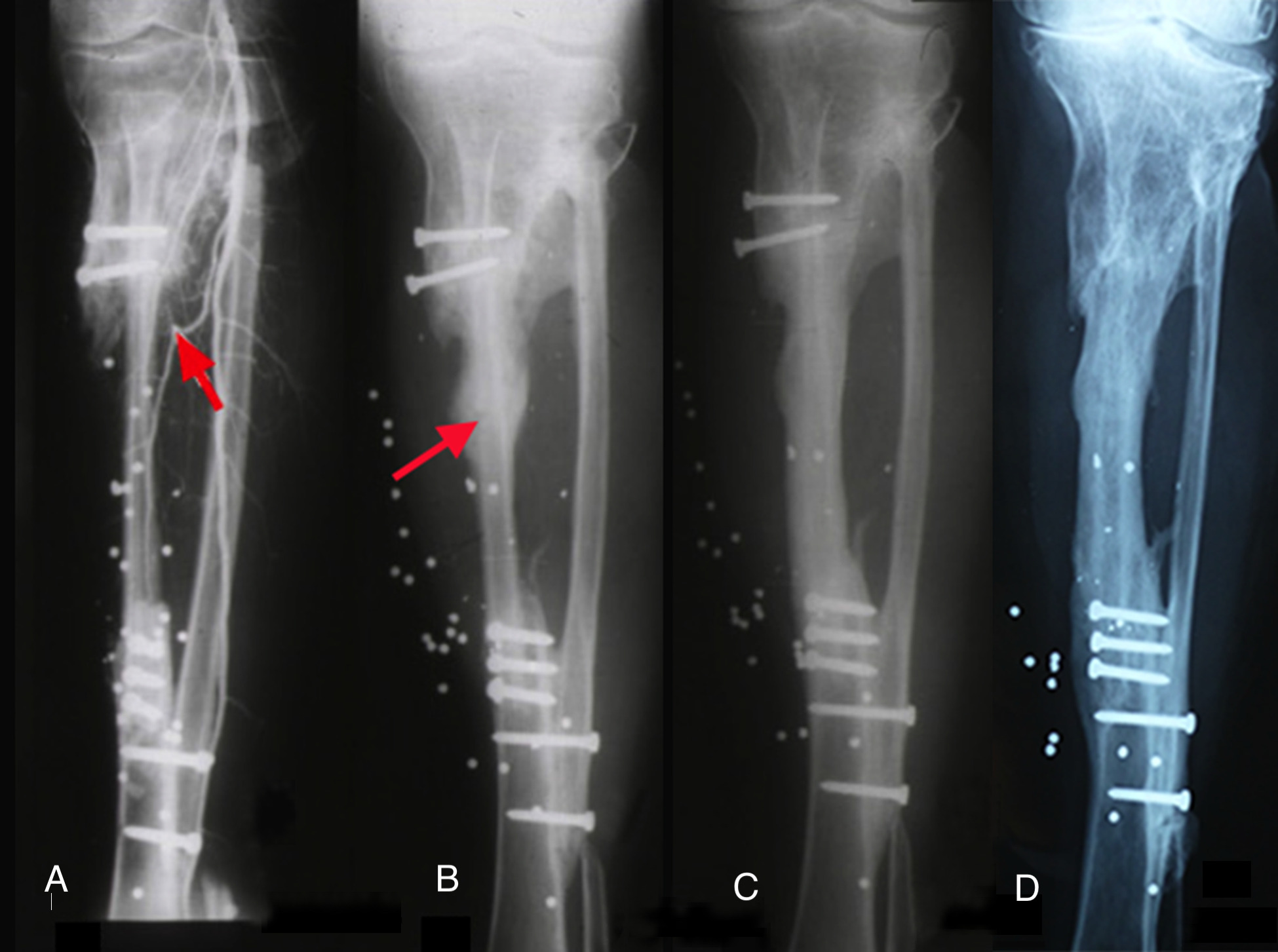
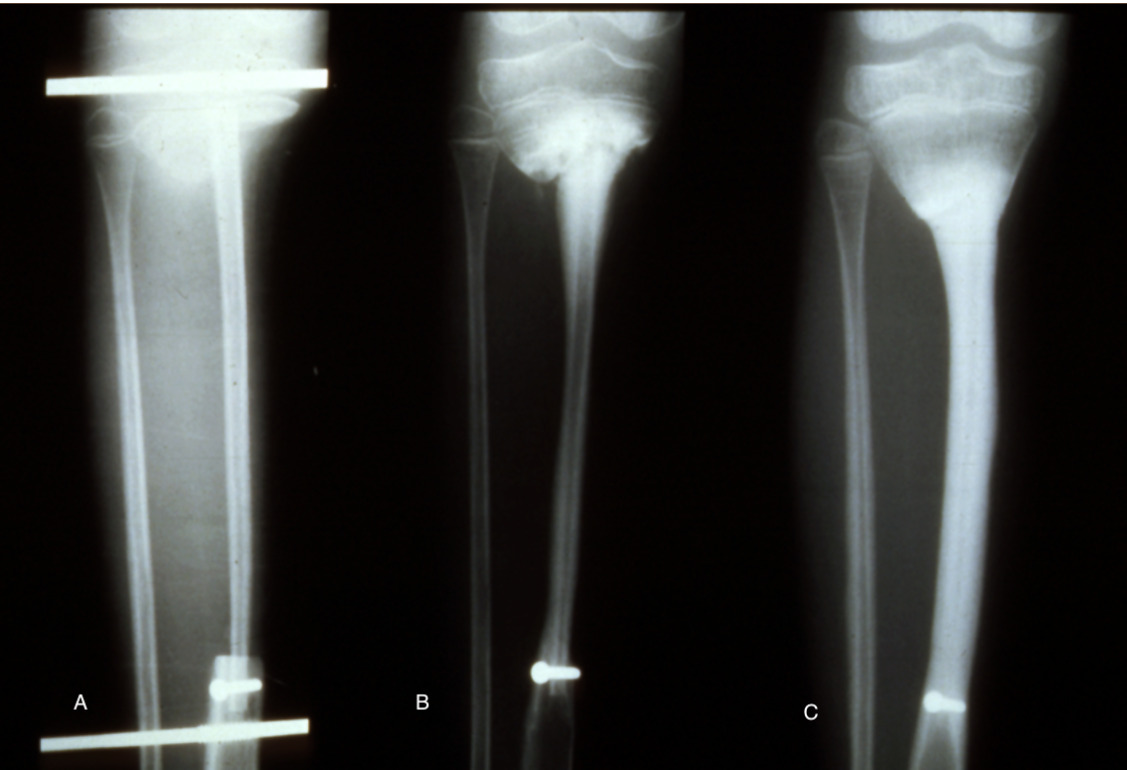
Both legs were placed in above-knee casts and the postoperative course was uncomplicated. The cast was removed from the donor right leg at three weeks and left on the other for six months. At five weeks an angiogram revealed a patent anastomosis (Figure 4A) and a bone biopsy revealed living osteocytes. At nine months the patient received an injury to his transplant when a door of a vehicle was slammed on his leg. The leg was a bit sore but he was able to walk with some discomfort. He presented a month later when an X-ray revealed not only a stress fracture, but showed callus and bony union in this transplanted fibula (Figure 4B)! Thereafter, remarkably in just two months, the fibula doubled its diameter! Subperiosteal thickening had occurred along its entire length, like wax dripping down a candle (Figure 4C). Notably, when reviewed 40 years later the original medullary cavity of the transplanted fibula was still visible (Figure 4D), with normal activity in both legs (Figure 5).6

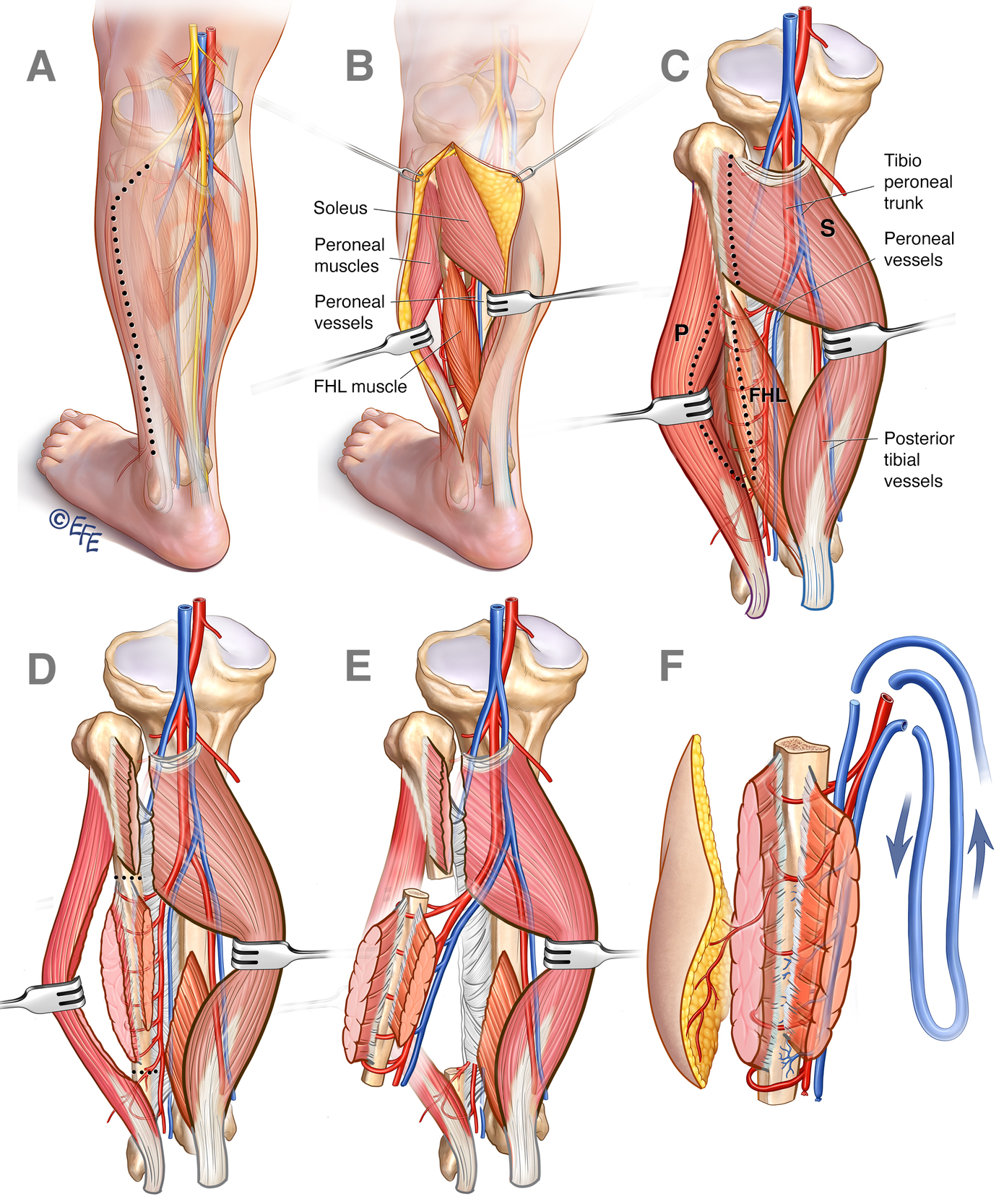
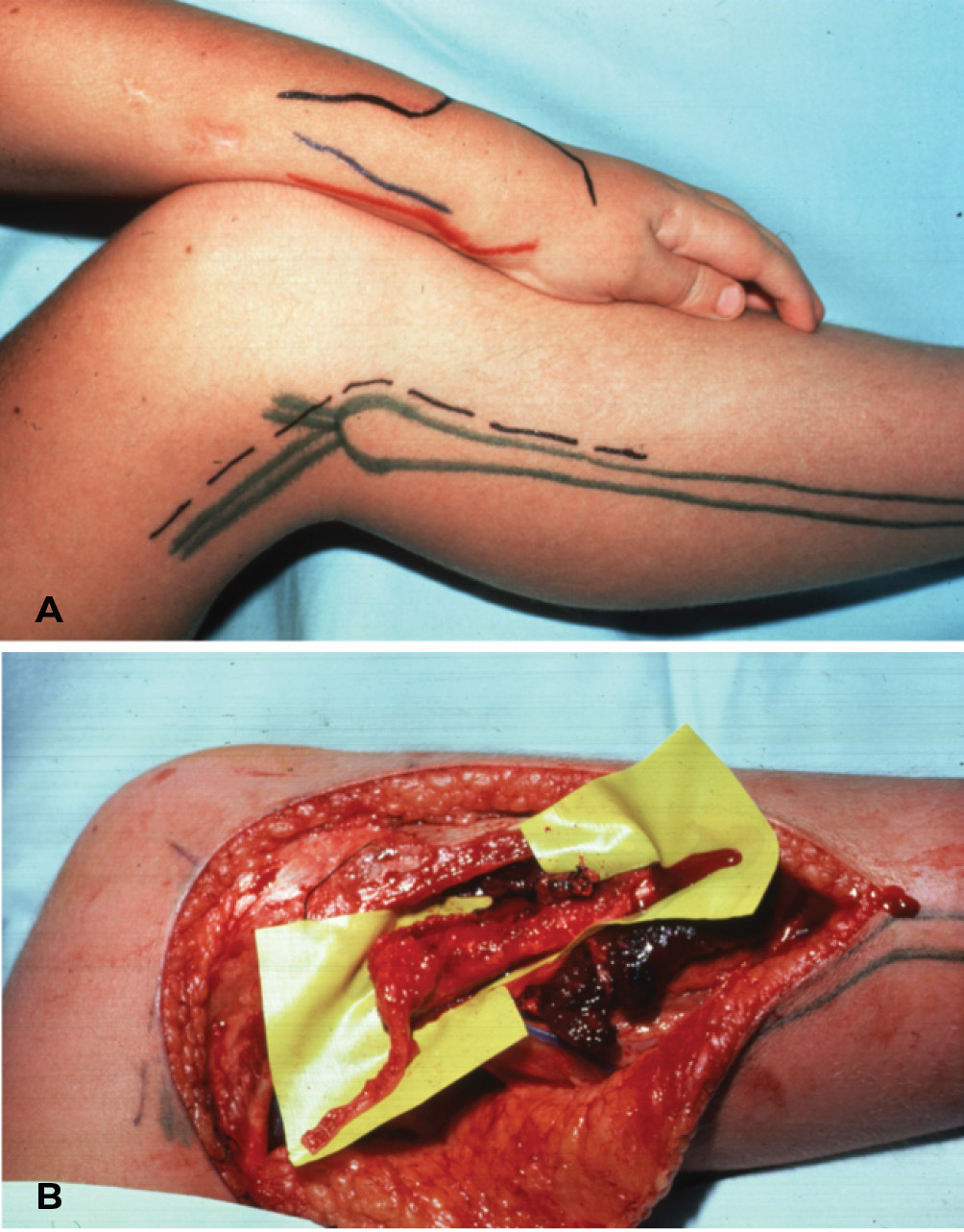
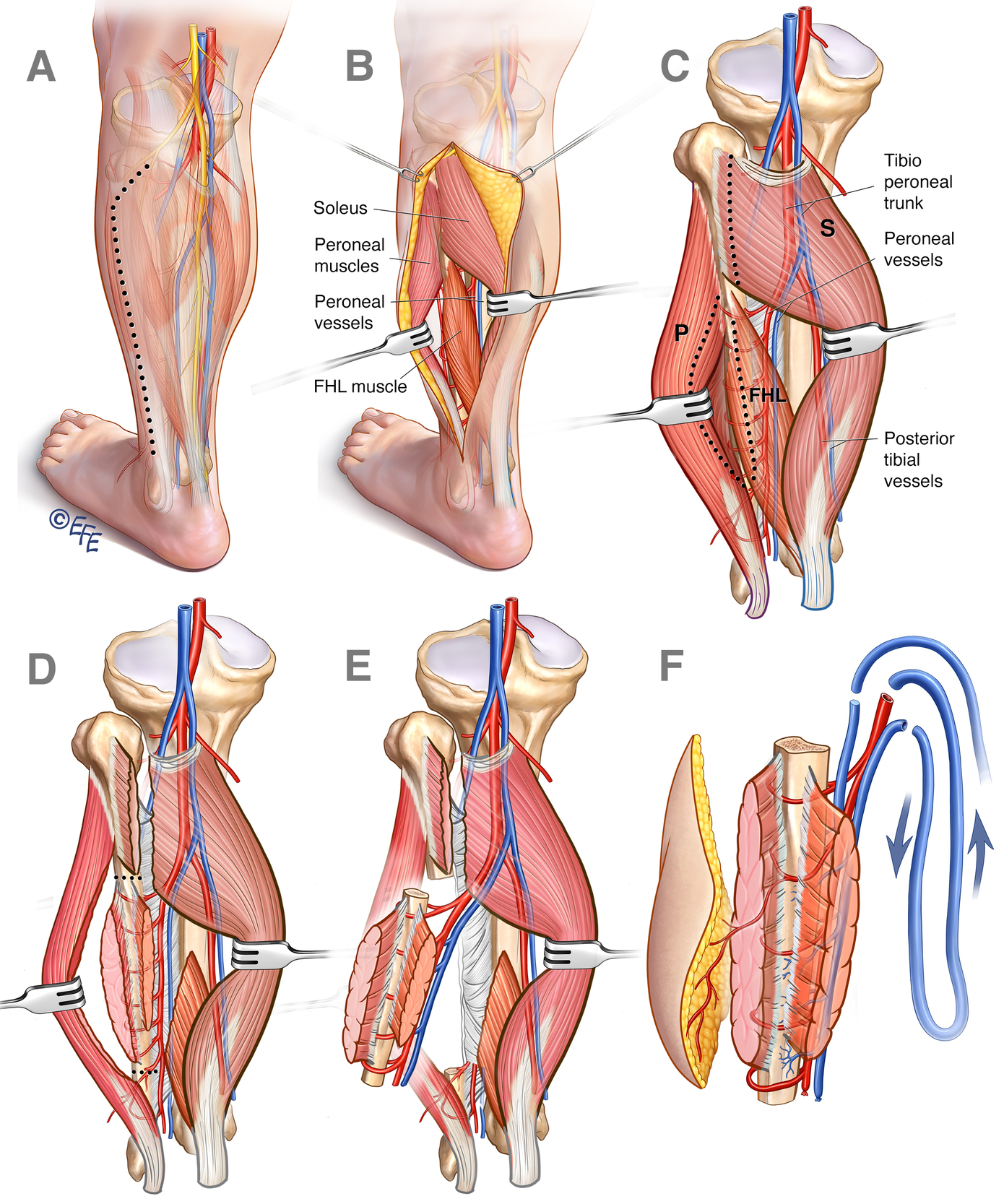
The reader will note that a posterior approach was used for both limbs. Since then we have raised the fibula via an anterolateral dissection with the patient supine, necessary to allow simultaneous dissection of other recipient sites, especially the head, torso and upper extremity (Figure 6).6
The anterolateral dissection
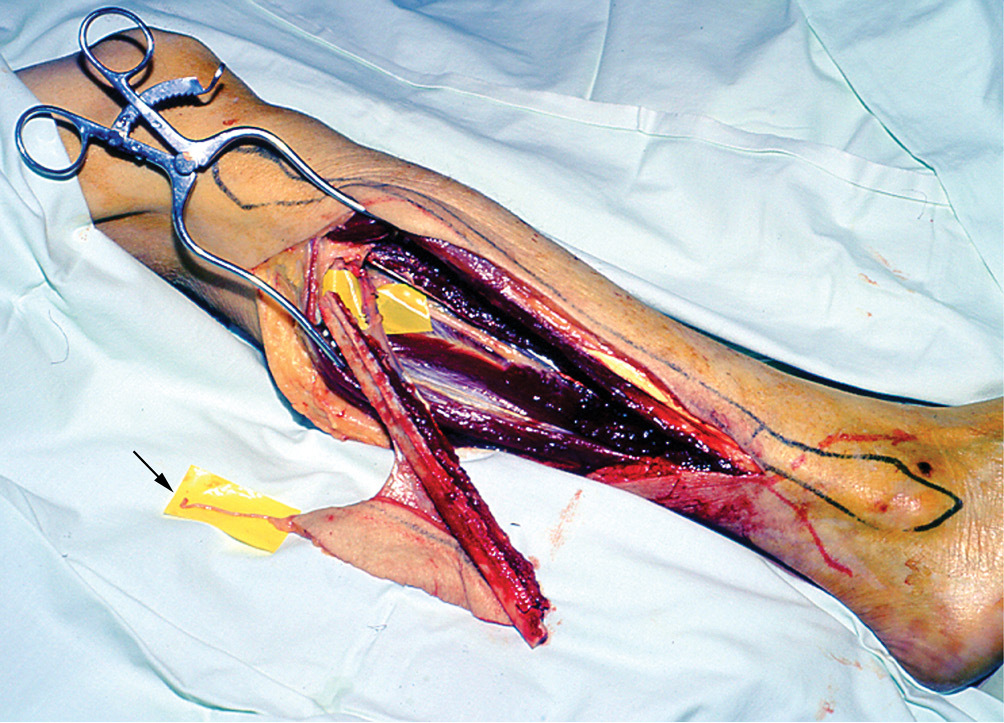
With the limb flexed at the knee and internally rotated at the hip, a sandbag is placed beyond the foot to steady the limb. If a skin flap is required it is planned before surgery using the Doppler to identify the location of the cutaneous perforator. It is important to make sure that this is done with the patient’s limb in the same attitude that it will adopt on the operating table—otherwise the location will move! The flap is usually planned distally in the leg where the perforators are septocutaneous, skin is thinner and the upper lateral cutaneous nerve of the calf can often be included for sensation (Figure 7). The most reliable perforator usually arises from the peroneal artery in the vicinity of its passage from the posterior to the anterior compartment of the limb.
The dissection is performed under tourniquet and discussed in detail elsewhere.6,7 The essential steps (Figure 6) are:
-
Longitudinal lateral incision between the peroneal and soleus muscles, passing around the anterior border of the skin flap if included in the design to identify the perforator, then curved posteriorly at the proximal end to identify and preserve the lateral popliteal nerve as it crosses the neck of the fibula.
-
Detach the tibialis anterior, peroneus longus and brevis from the fibula, leaving a sleeve of muscle along the bone and avoiding anterior tibial vessels and nerve.
-
Identify the cutaneous perforator(s) that arise from the peroneal vessels and emerge between the soleus and flexor hallucis longus (FHL).
-
Then identify the peroneal vessels themselves between the FHL and soleus. Commence distally by blunt finger dissection and proximally using scalpel. Take great care here to avoid the large veins draining the soleus as it is detached from the fibula.
-
Divide the fibula distally, leaving at least the distal quarter for ankle stability. Divide fibula proximally near the upper border of the FHL. This provides the option for a long vascular pedicle if needed, by discarding unwanted fibula proximally using a subperiosteal dissection.
-
Divide the interosseous membrane between the tibia and fibula. Ligate and divide the peroneal vessels distally.
-
The fibula is now more mobile. Trace the peroneal vessels with a sleeve of muscle as they course from distal to proximal, either adjacent to the septum separating the tibialis posterior and FHL, or within the latter muscle. Define their origin from the tibioperoneal bifurcation.
-
Release the tourniquet.
Fibula blood supply
In 1982, we decided to re-evaluate the blood supply to the fibula together with the adjacent soft tissues.7,8 This was fortuitous as the following case reports will reveal. Various functioning muscles such as the soleus9 and FHL10 had been included in the transplant, as well as the overlying skin.11 The upper growth plate had been transferred on the peroneal vessels and combined with a separate lateral inferior geniculate pedicle. However, results were poor and the epiphysis fused early.12 Finally, vessel anomalies were common in the leg and rarely the peroneal artery, the developmental artery of the limb, was the only vessel supplying the foot13 (the peronea magna).
The study was performed in 66 fresh cadaver limbs. The contribution to the fibula, skin and adjacent soft tissues from the peroneal and anterior tibial vessels was examined using (i) India ink injection and bone histology, and (ii) lead oxide radiography of their vascular anatomy.8
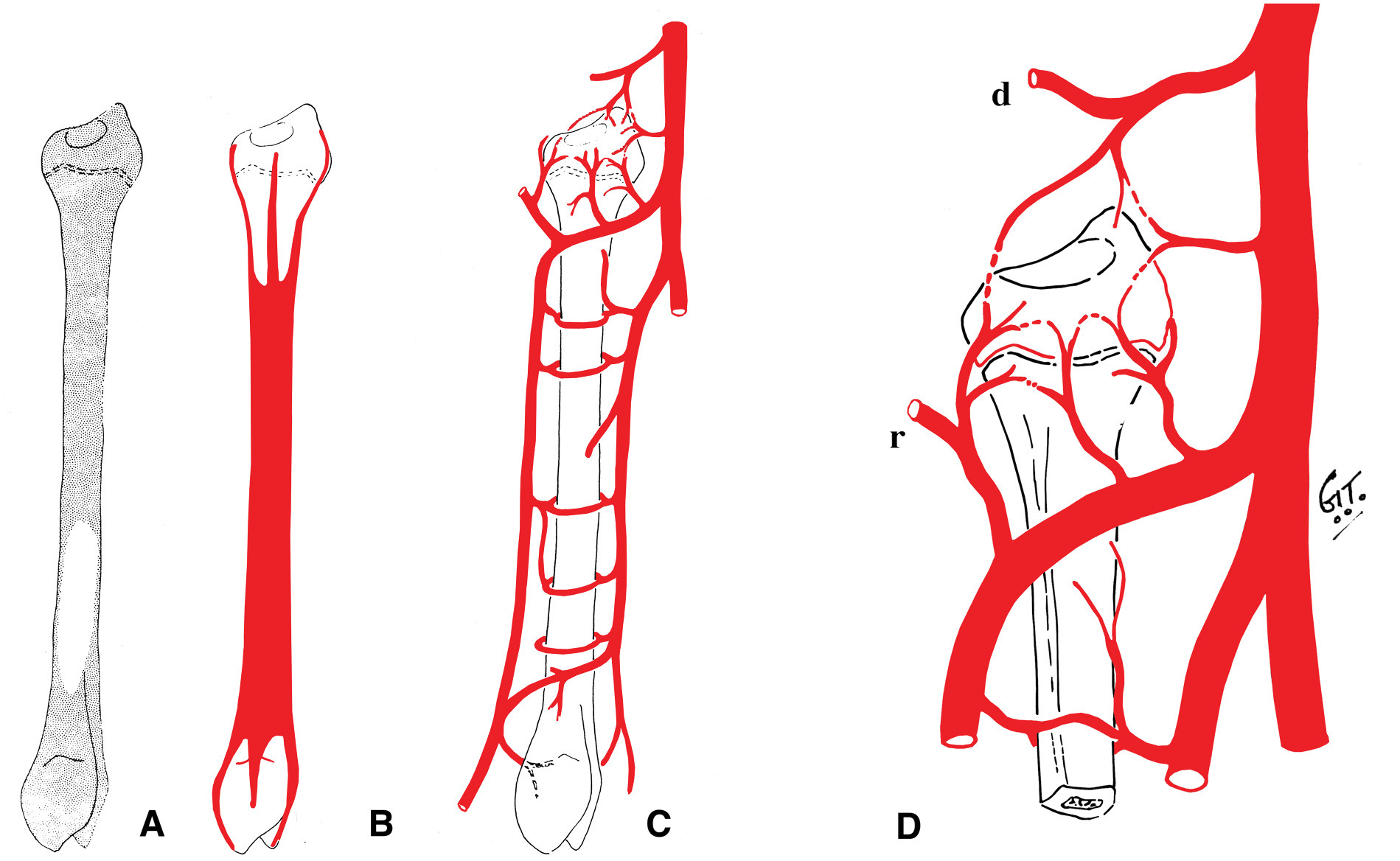
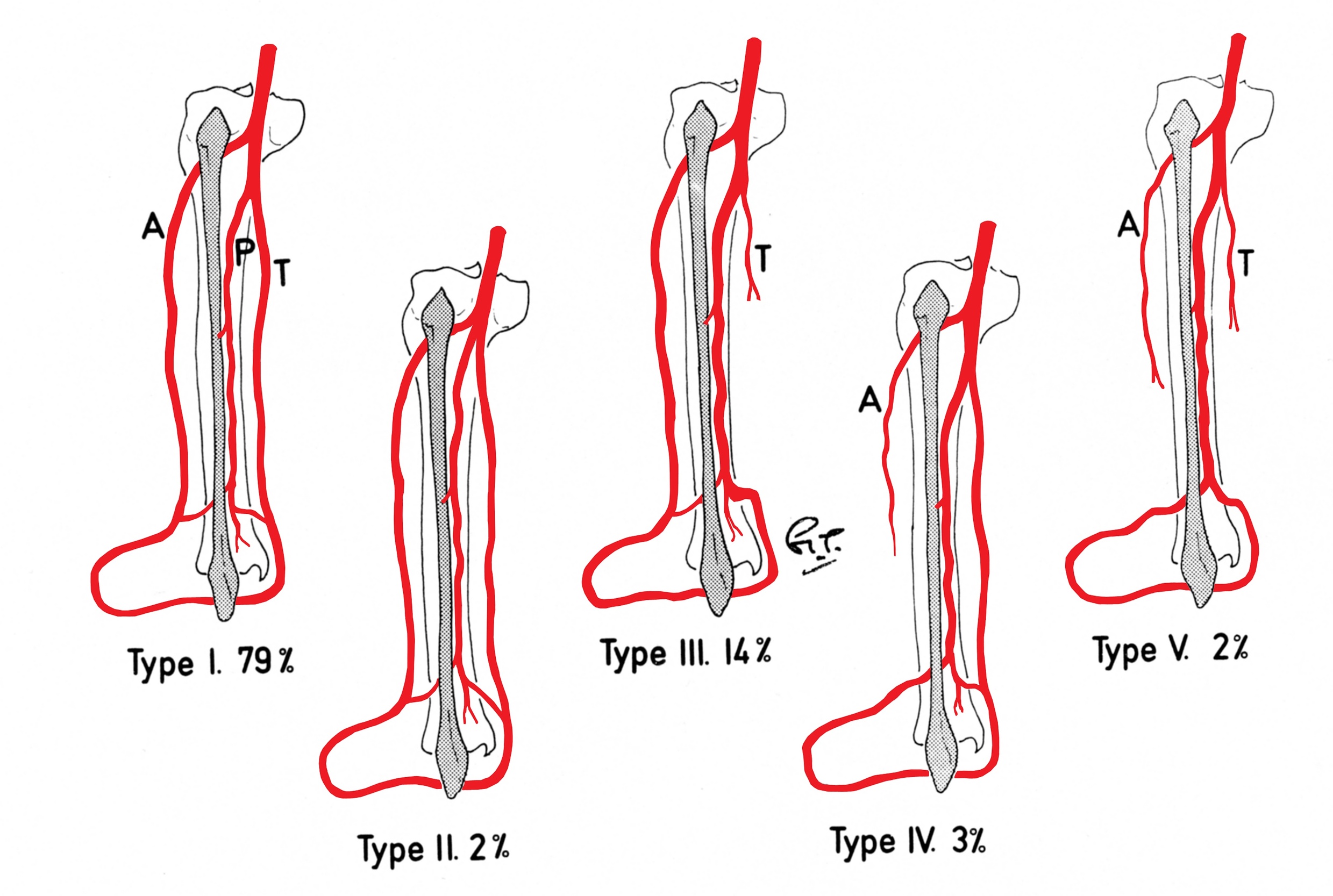
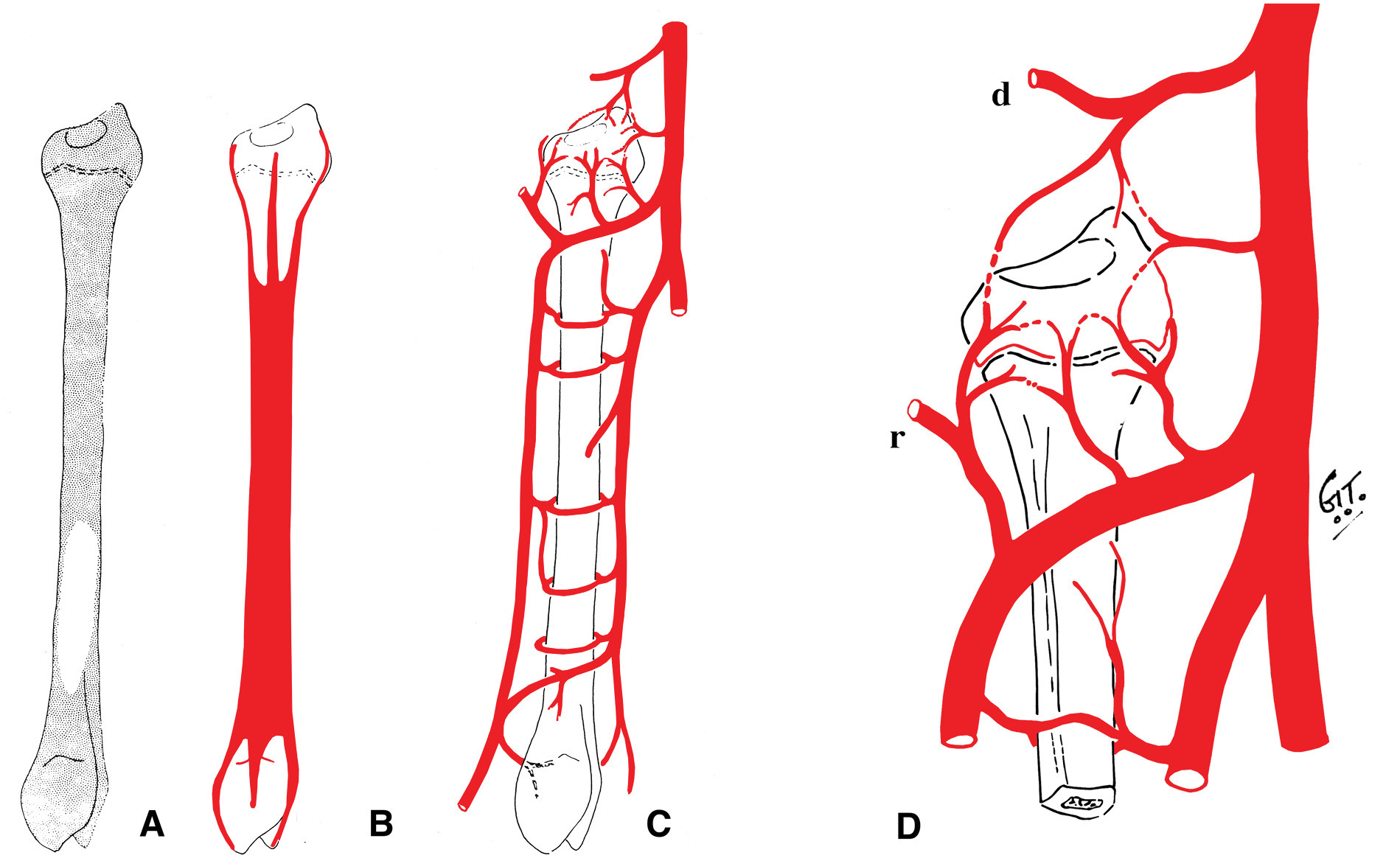
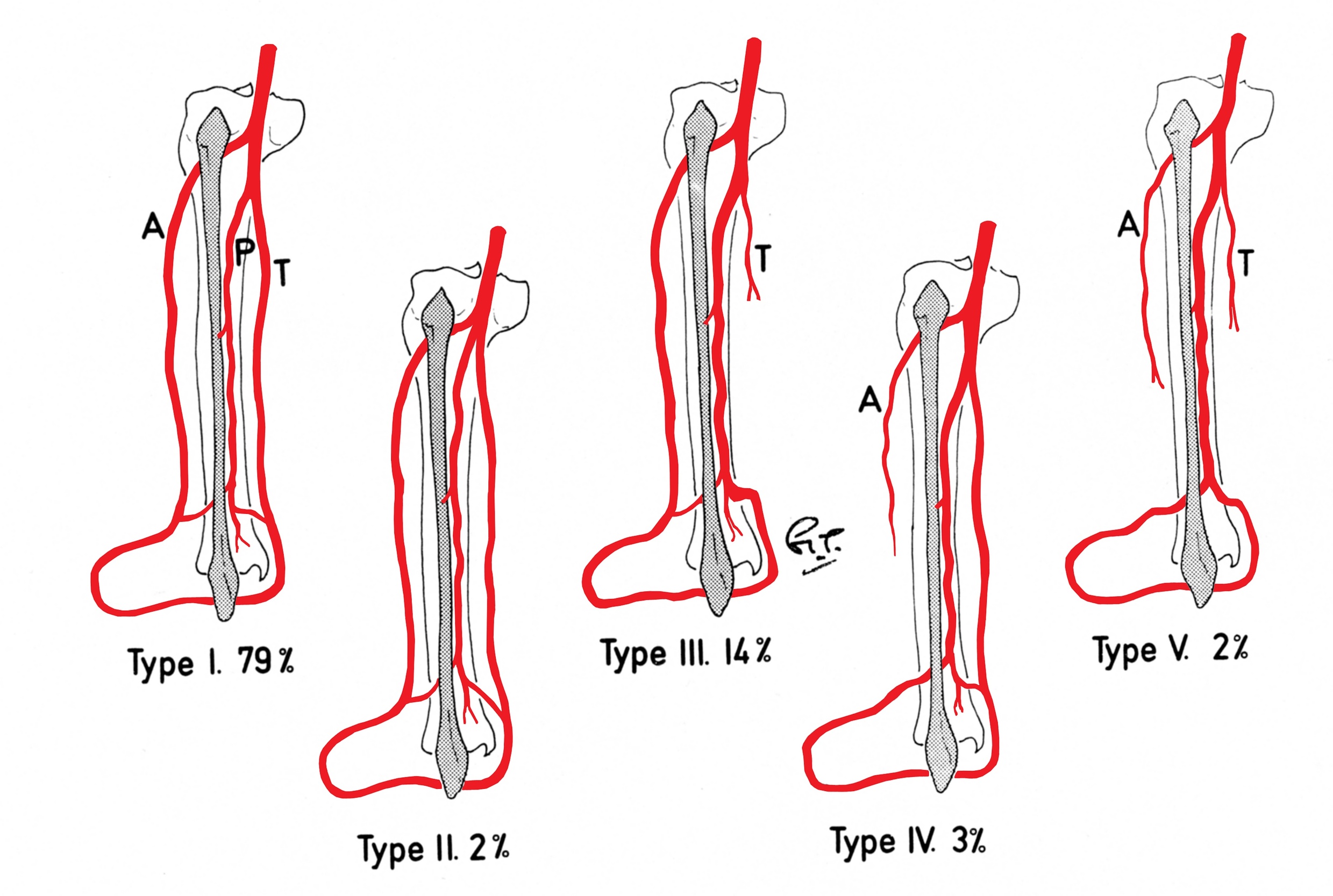
These studies revealed a reliable blood supply to the proximal epiphysis and the proximal two-thirds of the diaphysis from the anterior tibial artery (Figure 8A). The branches to the epiphysis from this artery were provided by the recurrent genicular artery and several short vessels arising from the anterior tibial as it passed forward beneath the tibiofibula joint (Figure 8D). Although the peroneal artery provided the dominant supply to the shaft of the bone via its nutrient and musculoperiosteal branches, its contribution to the head of the fibula was scanty (Figure 8B). Finally, the vascular anatomy to the leg was examined in 100 clinical angiograms revealing 21 limbs with anomalies, including two cases with a peronea magna (Figure 9).
Case 2: the anterior tibial pedicle
In 1983, a nine-year-old girl presented with a Ewing’s tumour of the right tibial diaphysis (Figure 10 left). She was treated initially with chemotherapy for 12 months with a good result. Segmental resection of the tibia was contemplated and we were invited by Ian Torode and Bob Dickens to consider a fibula reconstruction at the Royal Children’s Hospital Melbourne. Preoperative angiography however, revealed a single peronea magna supplying the foot in the other donor leg. The anterior tibial artery was diminutive (Figure 10 right) but was considered to be of a sufficient size to nourish the fibula transplant.

The operation was performed on 29 November 1983. The tumour was resected from the right leg between the underside of the upper growth plate and the shaft of the tibia distally (Figure 11). The fibula shaft was dissected from the left leg by the other team to bridge the 15 cm tibial defect. In addition to Russ and Ian was one of the greatest characters and contributors to our profession—the inimitable and forever missed Ian Carlisle.
The dissection of the fibula is described in detail elsewhere.7 Briefly, under tourniquet:
-
A longitudinal anterior incision was made just lateral to the tibialis anterior and curved laterally at the proximal end to identify and preserve the lateral popliteal nerve.
-
Commencing distally, the anterior tibial vessels and nerve were identified as they were crossed by the tendon of extensor hallucis longus (EHL).
-
The vessels were traced proximally, between the muscle bellies of EHL and tibialis anterior. Then between tibialis anterior and extensor digitorum longus (EDL).
-
The anterior tibial nerve was separated and preserved from its vessels, as well as skin perforators when a flap is required.
-
Branches of the lateral popliteal nerve to the peroneal muscles, tibialis anterior, EDL and EHL were identified and preserved as they entered the proximal end of the muscles.
-
These muscles were then separated from the fibula, leaving a 1 cm sleeve of muscle. The anterior tibial vessels were divided distally. Next the fibula was sectioned at each end leaving the distal quarter, and finally the interosseous membrane was divided.
-
The fibula was then mobile. The distal end of the bone was retracted, the tibialis posterior, FHL and soleus were detached with a sleeve of muscle, and finally the proximal pedicle of anterior tibial vessels was isolated and the fibula was divided. Bleeding from both ends of the fibula was confirmed after releasing the tourniquet.
An 18 cm length of fibula was detached and transferred to bridge the 15 cm defect in the tibia. Periosteum was stripped from the distal end, dowelled into the tibia and secured with a screw. The proximal end was abutted against the underside of the growth plate of the tibia, balanced like a saucer on the end of a pole, and stabilised with an external fixateur (Figure 11A).
At three months the distal end of the fibula graft had united to the tibia. The fixateur was removed leaving behind the transfixing pins that were fixed into an above-knee plaster cast. At eight months the cast was removed, the limb placed in a caliper and weight bearing commenced. Union was noted at the upper end (Figure 11B). By two years dramatic hypertrophy of the transplanted fibula was noted together with growth from the proximal epiphysis (Figure 11C). The limbs had almost identical length (Figure 12), the knee and ankle joints were normal and the only disability was temporary weakness of the EDL in the donor leg.

Case 3: the growth plate transfer
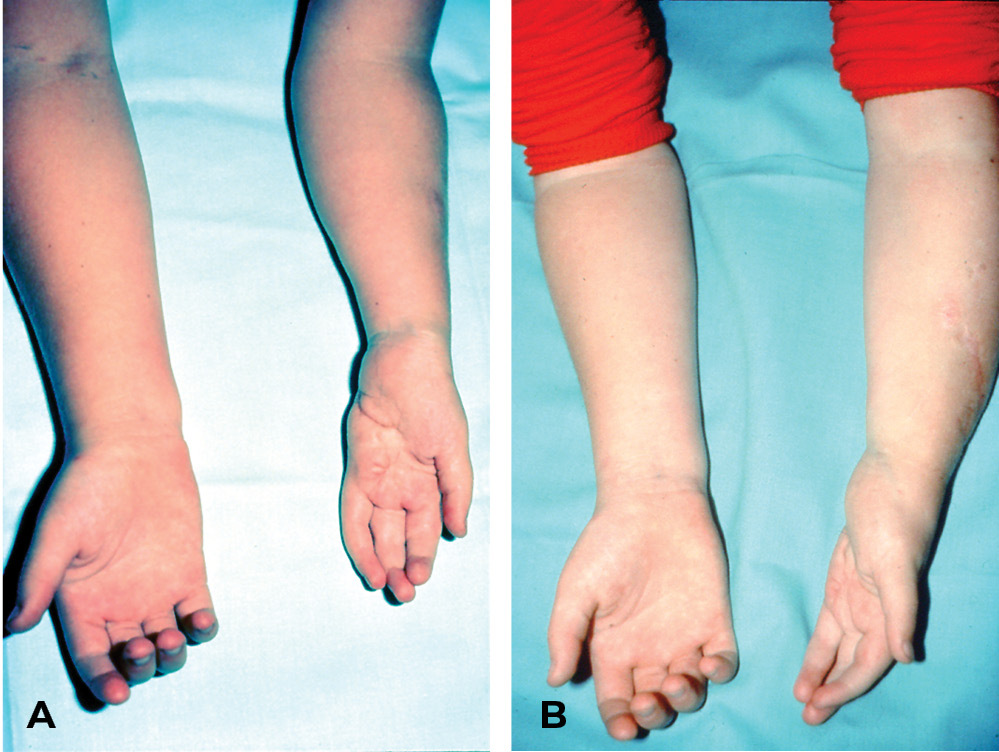
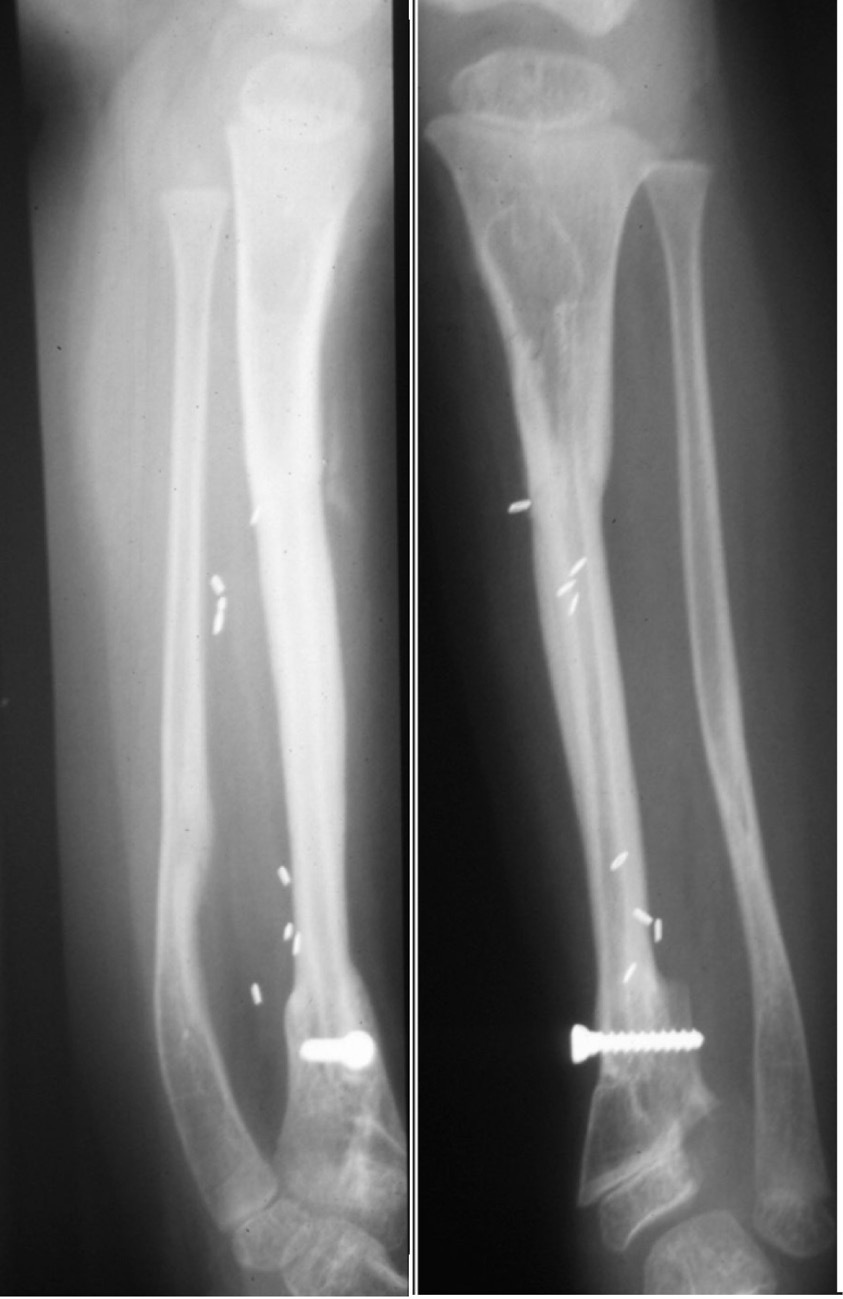
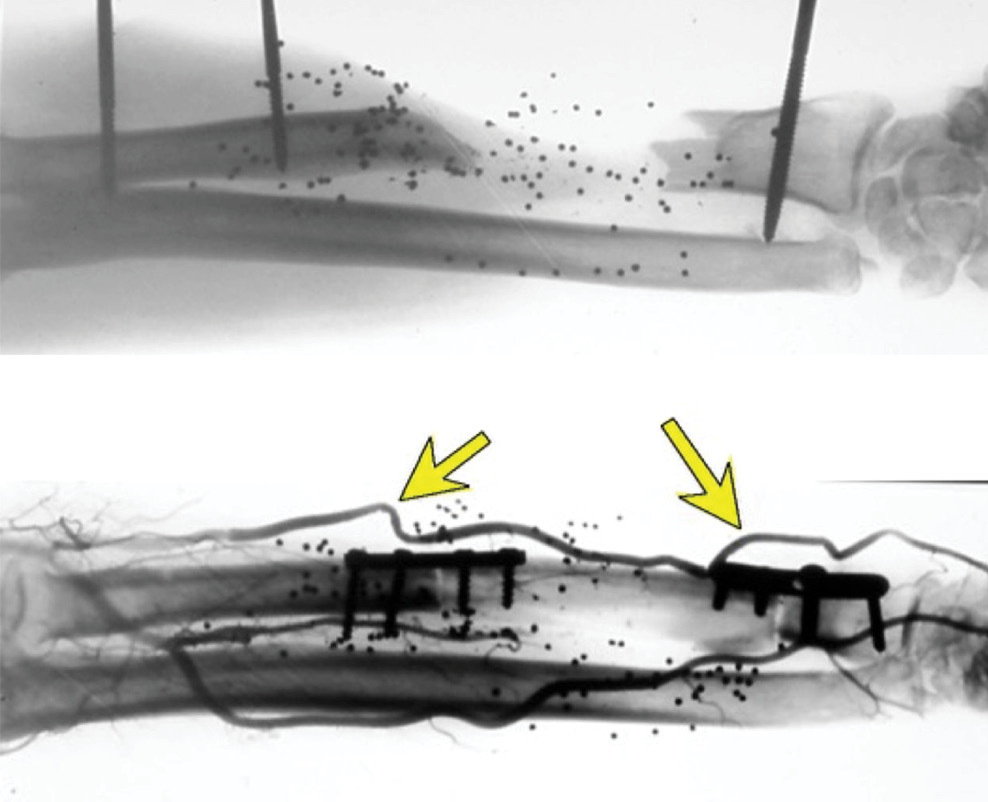
On 20 March 1982, a four-year-old boy sustained a severe compound injury to his left forearm and hand from a motor mower accident. Distal ends of the radius and ulna, and fifth metacarpal and carpal bones on the ulnar side of the hand were missing (Figure 13A). Treated initially by Tim Pitt, the hand was debrided and closed with a filleted fifth finger skin flap and stabilised with an external fixateur. Over the following six months, spontaneous regeneration of the distal radius was observed from residual periosteum that became incorporated with the distal epiphysis (Figure 13B). However, its growth plate had been destroyed, the forearm was short and the patient was referred to us by Tim Pitt for possible free vascularised growth plate transfer.
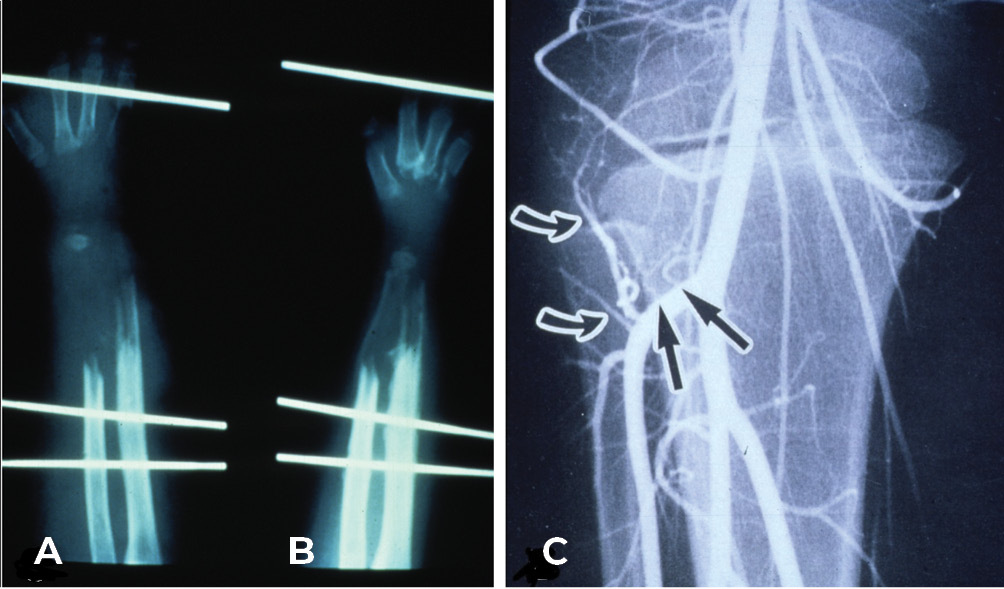
Preoperative angiography revealed the radial artery to be the only major vessel to the hand. A normal three major vessel supply was noted to the right leg. Multiple branches to the epiphysis from the anterior tibial artery were revealed and especially the recurrent genicular artery (Figure 13C). We were about to embark on another first at PANCH and we needed to ensure that disability was minimal in the donor leg. Therefore, it was planned to split the tendon of insertion of biceps femoris to the head of the fibula—half to be left and stapled to the tibia for knee stability; the other half was to anchor the transplant in the hand (Figure 14).
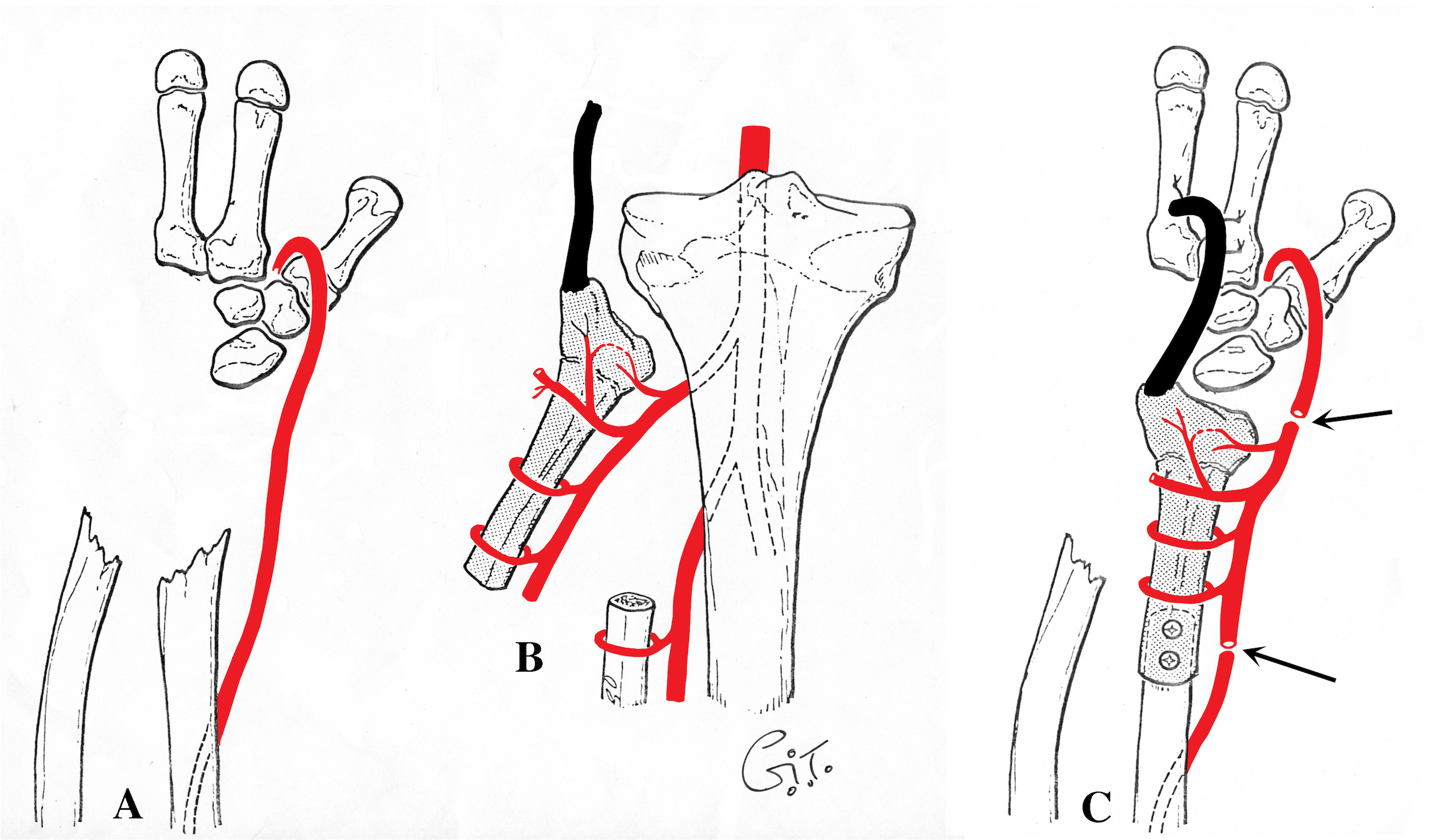
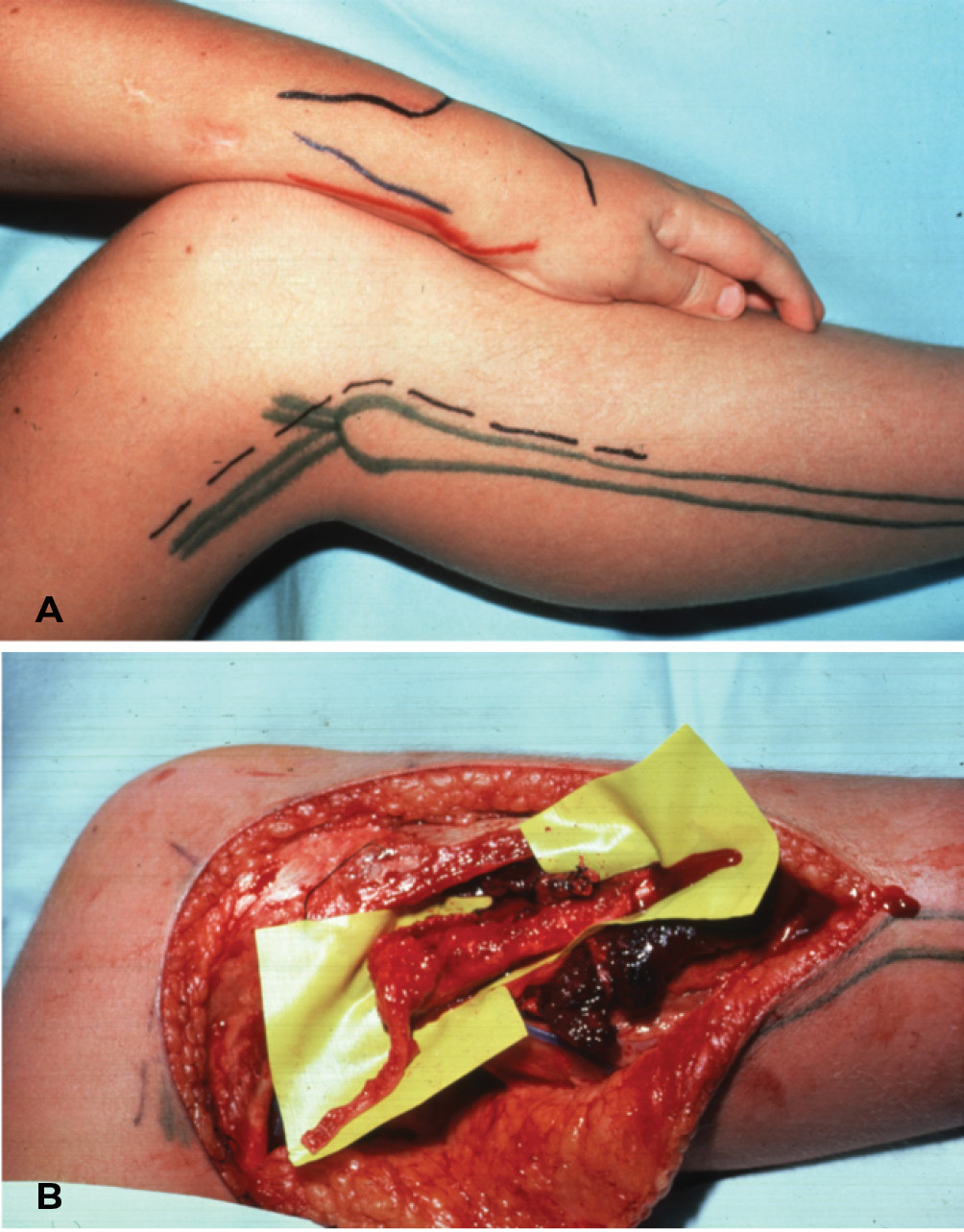
The incisions were marked (Figure 15A) and the operation was performed on 7 May 1984. The head and proximal shaft of the fibula was isolated on the anterior tibial vessels together with a strip of the biceps femoris tendon (Figure 14 and Figure 15B). The flap was detached and transferred to the hand. The shaft of the fibula was fixed to the radius with screws and the head of the bone was snugged against the remaining carpal bones by weaving the biceps femoris tendon beneath and around the insertion of the radial wrist extensors (Figure 14).
The fibula was revascularised by proximal and distal anastomoses of the anterior tibial artery to the radial artery and proximal vein repairs. The knee joint was stabilised in the donor leg as described above, and distally slivers of fibula were placed between the fibular stump and the adjacent tibia in order to achieve a fibula–tibial synostosis.
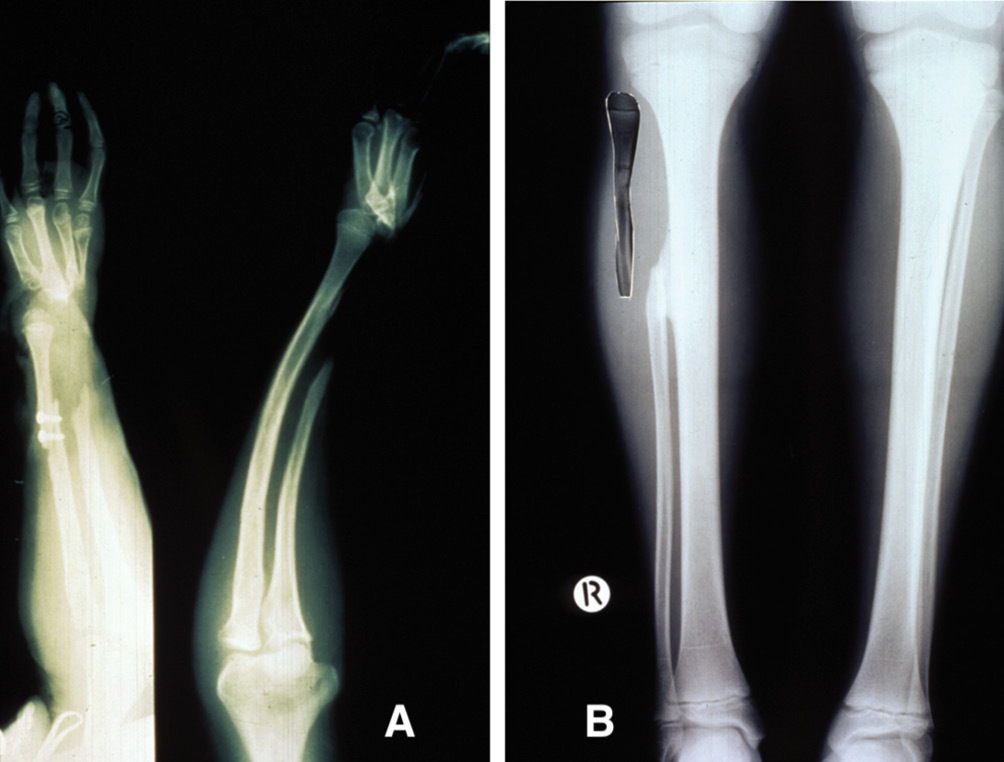
Bony union of the fibula to the radius was evident at six weeks. Serial X-rays of both forearms were made at three-monthly intervals over the next four years and the results confirmed with bone scans. These revealed an average growth rate of 5 mm per year of the fibula growth plate, which compared with that of the distal radial epiphysis in the opposite forearm (Figure 16A) and the proximal growth plate in the fibula of the normal left leg (Figure 16B).
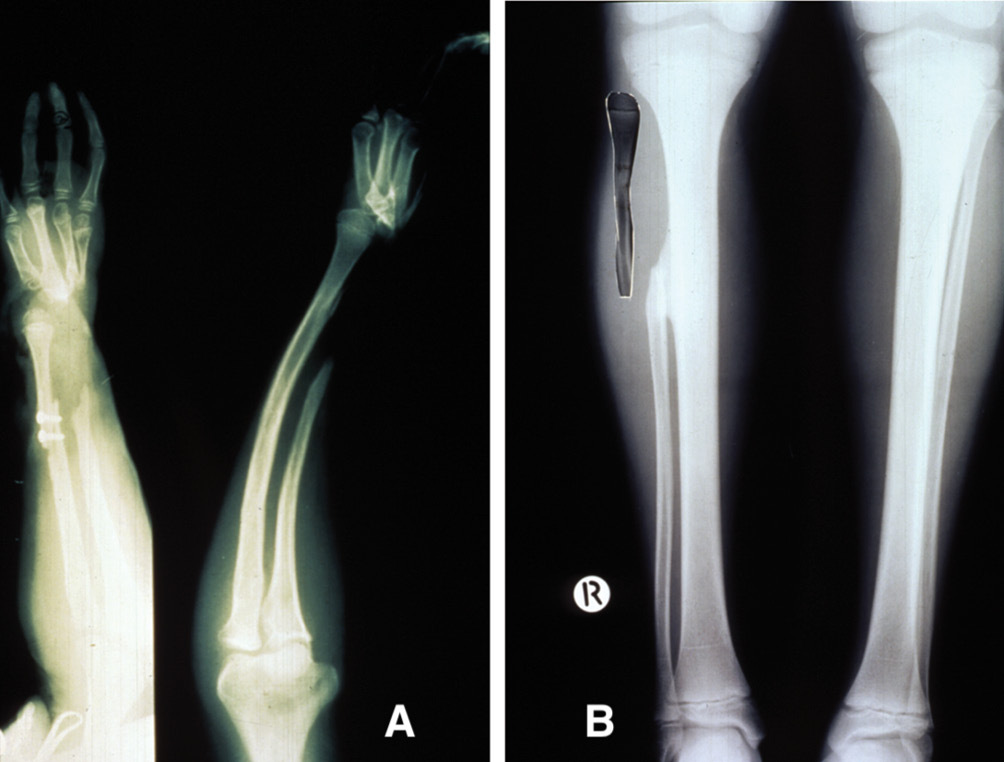
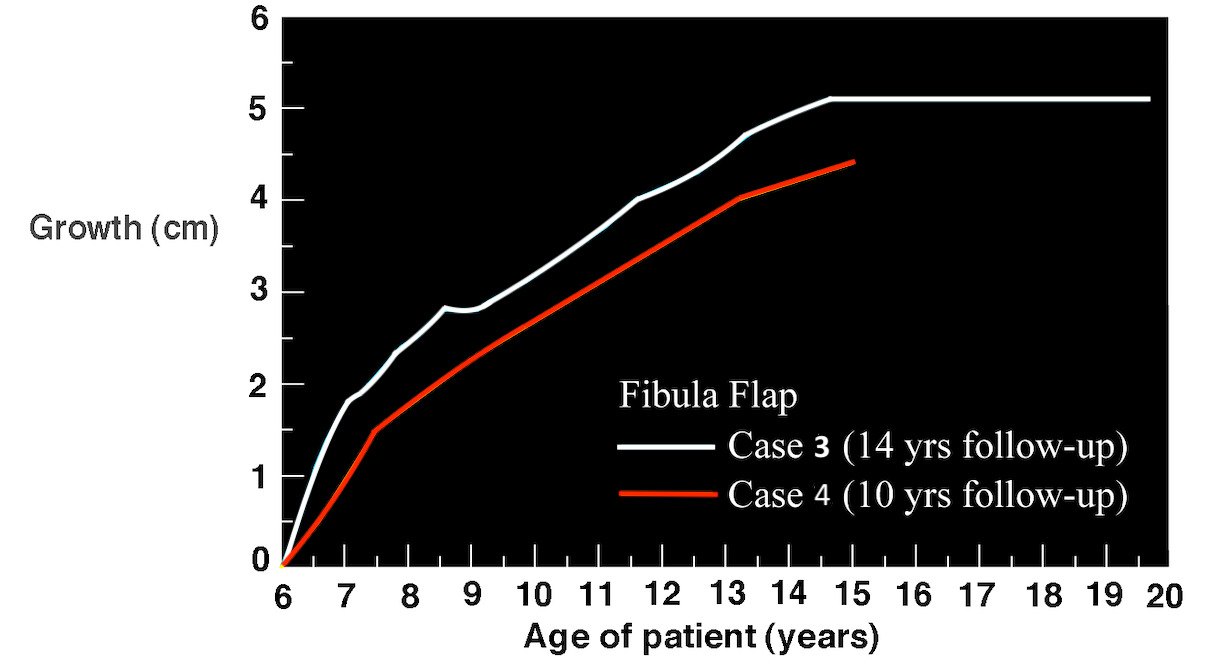
During this four-year period a further operation was required in September 1985 to stabilise the hand on the head of the fibula, for such was the growth rate that the hand was being progressively displaced in an ulnar direction, and the forearms became of similar length (Figure 17). The most recent X-rays reveal that the fibula growth plate had fused at age 15. This is the normal time for fusion of the proximal growth plate of the fibula. When the X-ray was compared with the opposite normal leg it was found that the transplanted epiphysis had grown at the same rate; it had averaged 0.5 cm per year (Figure 18). Functionally the patient has a very useful hand (Figure 19). The donor leg is stable at the knee, it is of normal length and there is no valgus deformity at the ankle joint.
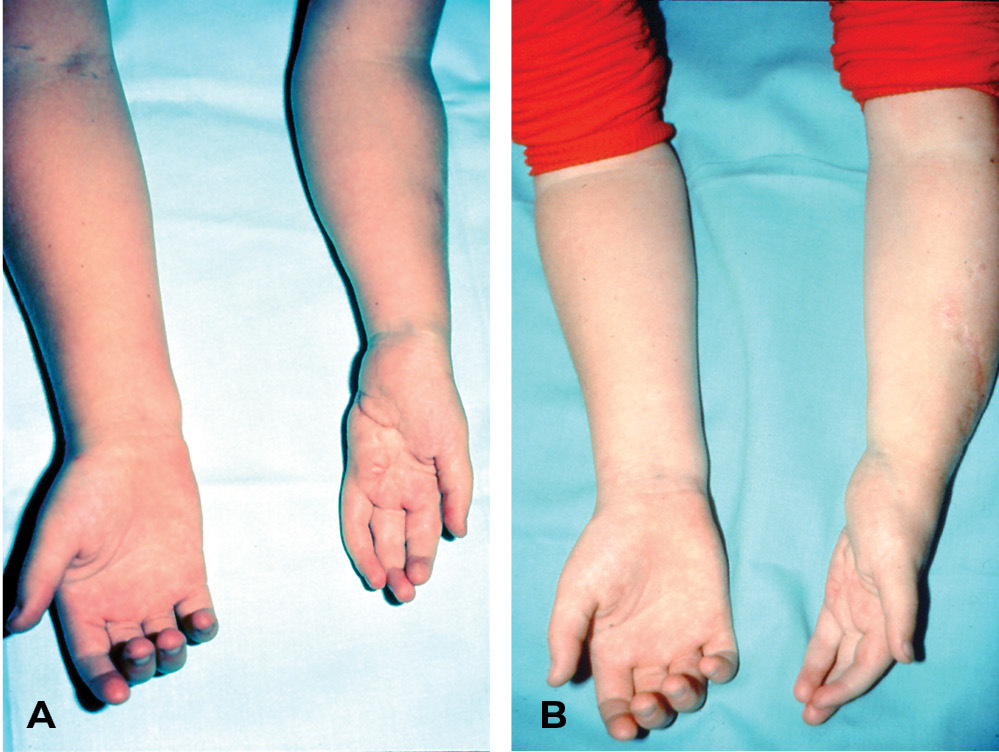
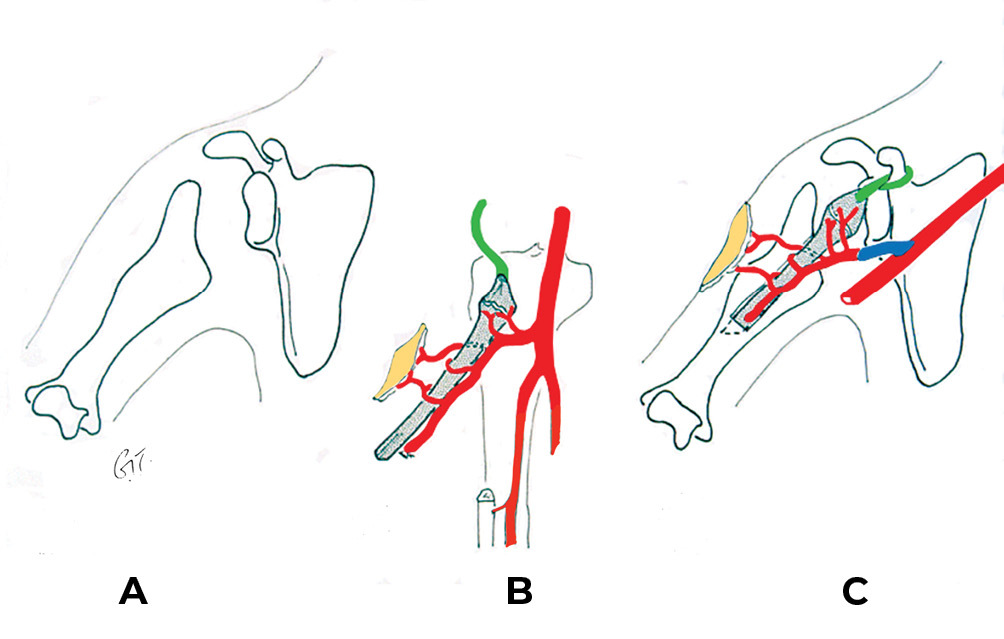
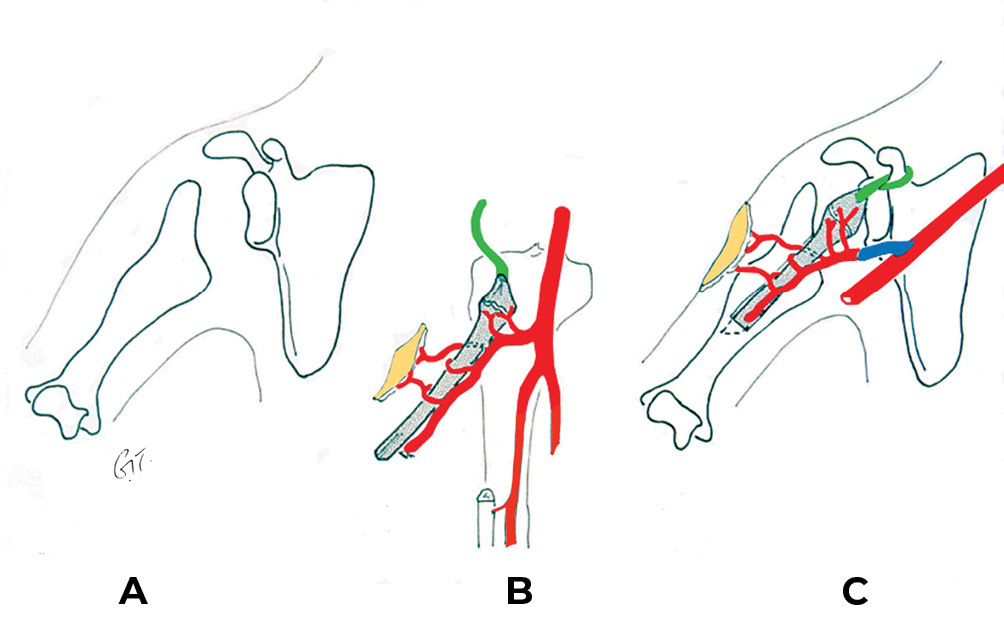
Another transplant was performed in a five-year-old boy (Case 4). He presented with an absent growth plate at the upper end of his right humerus as a result of neonatal septicaemia, which caused him to have a very short arm (Figure 20A). Similar to the previous patient, the upper end of the fibula growth plate was transferred on the anterior tibial vessels. The head of the fibula was secured in the shoulder joint by using the biceps tendon and sutured around the base of the coracoid process of the scapula. A small skin flap design was used to monitor the anastomoses (Figure 20B and C).
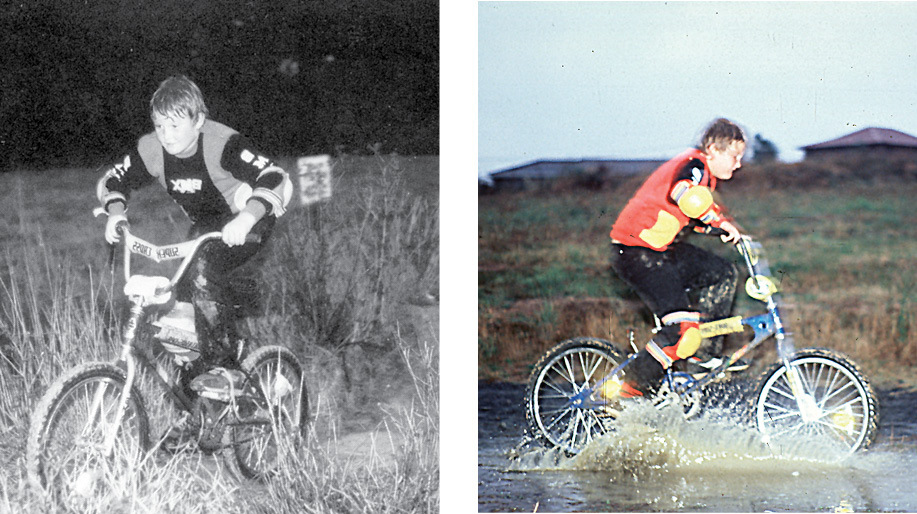
The bone transplant united to the humerus and fibula growth occurred at a rate similar to the epiphyseal transfer in the previous patient (see Figure 18). He was lost to follow up for many years and was seen again at age 15, when it was found that the upper end of the fibula had dislocated anteriorly and superiorly (Figure 21 and Figure 22). Despite this deformity that understated the true growth in the transplant, he had pain-free movement of the shoulder and was a very active surfboarder.

Discussion
In 2016 we reported our 40-year experience with 384 free vascularised bone transfers between 1 June 1974 and 1 June 2014 with a success rate of 96 per cent.14 The most common donor site was the fibula (198 cases), with the iliac crest (180 cases) designed on either the SCIA or the DCIA running a close second (Table 1).14 The mandible headed the list for recipient sites. Most cases were done at the Royal Melbourne Hospital, PANCH or Royal Children’s Hospital Melbourne, with a significant number done overseas on Interplast trips or by invitation to the USA, Canada, South Africa, Bangladesh and Sri Lanka. Meanwhile, on a visit to Beijing in 2014 no less than 4000 fibula transfers, with a success rate of 99 per cent, were presented. They were done from just two units during the previous decade, for reconstruction of the jaw and the extremities.15–18
When we presented our series in 2016, we considered the fibula to be the ideal bone for reconstructing the long bones of the extremities, the clavicle, the mandible and maxillary jaw from angle to angle, done especially in the edentulous elderly with the atrophic jaw and the growth plate in a child. It had the special advantage of offering a choice between the peroneal or anterior tibial pedicle.
The DCIA iliac bone was considered best for restoring the mandibular ramus, a functional temporomandibular joint without dislocation (even today), with adequate bone height for osseointegration and, especially in the younger patient, sufficient bone spanning from the temporomandibular joint on one side to reach the opposite angle of the jaw with a single osteotomy. It is ideal also for replacement of the curved bones of the pelvis, hand and foot plus a straight segment of 6–8 cm of iliac crest beyond the anterior superior iliac spine (ASIS) for reconstruction in the lower limb.
Today the fibula has moved to centre stage. The authors have footprints on our shoulders. Refinements of planning and techniques at the Royal Melbourne Hospital have made the fibula first choice for mandibular reconstruction. It is timely now to focus on key points regarding case selection, preoperative planning, operative technique, bone fixation, postoperative management and patient care.
Case selection
Guided by our orthopaedic colleagues, who consider that a non-vascularised bone graft of up to 5 cm has a high success rate when placed in a well vascularised bed, we selected our cases for larger gaps between 6 and 33 cm. Skin flaps can be combined with either the fibula or the iliac crest, often with sensation. Other donor bones have been the rib, distal radius and metacarpal. They were used where the fibula or iliac crest were unavailable, or for special recipient site requirements.
Preoperative planning
Done usually the day before surgery or earlier, we believe that this preparation is crucial for success.
-
Angiography: first it offers the surgeon a choice between donor legs. Not only may it reveal the presence of a peronea magna, but for example (i) a longer peroneal pedicle as shown by the early division of the tibioperoneal trunk seen in Figure 9 (Type 2) or (ii) vascular disease. Atheroma with obstruction of the beginning of the peroneal artery is not uncommon. However, it is often a short segment that is involved and the remainder of the artery may still be available.
-
Skin incisions: comment has been made already that highlights the distal siting of the skin flap (Figure 7) and the need to identify the perforator with the patient in the operative attitude. The following is an additional incision that needs to be considered before surgery.
-
Vein grafts: in some cases, and especially in the thigh because of muscle bulk or in the neck following previous surgery or radiotherapy, there may be the need to lengthen the vascular pedicle or the recipient vessels. When so we use the ‘Corlett loop’.6 Distended with heparinised Ringer’s solution and venous valves oriented correctly, it is divided appropriately to match the arterial and venous anastomosis (Figure 23). We select either the cephalic or basilic vein in the forearm; they are thin-walled and often match the size of the recipient vessels. We avoid saphenous veins because they are thick-walled, often go into spasm and are usually too large. Marked out before theatre it warns the anaesthetist that this arm is taboo! Another ‘trick’, especially in the irradiated neck, is to pedicle the cephalic vein from the upper arm to the neck. To be marked out again before surgery.
-
Computer generated bone replicas: they are used especially for jaw reconstruction. See below under ‘Bone fixation’.
-
Rehearsal in cadavers: this is priceless, not only for the beginner but especially for unfamiliar recipient sites or donor sites such as the DCIA iliac crest transplant. Such procedures can be done in the hospital mortuary with permission and especially if there are no extra external incisions. Currently the University of Melbourne is establishing a forum for this to take place in the Melbourne Academy of Surgical Anatomy.
Operative technique
The most important factor in our experience is to keep the patient warm and well hydrated, including any blood transfusion. Initially our greatest enemy was arterial spasm. Our success rate was about 65 per cent and the phone call after midnight of a failing flap was dreaded! It invariably meant a return to theatre with a tired surgeon and anaesthetist and few flaps were rescued.
When the patient was warmed, our success rate jumped to the high 90 per cents. We even had 100 successful cases in succession at one stage. Then we lost two flaps in a row, both due to delayed and undetected recipient vein thrombosis when a muscle flap was used to repair a traumatic leg wound and surfaced with a split skin graft. Following this we delayed the application of the skin graft for several days until we were sure that the muscle was viable.
The anastomotic technique will vary between surgeons. The peroneal vessels, except in a child, are more than 2 mm so the success rate is usually high. Briefly our method, whether end-to-end or end-to-side, usually involves the following sequence:
-
yellow plastic background behind artery
-
arterial anastomosis first with interrupted sutures
-
back wall then front, leaving three sutures untied
-
irrigate then tie sutures
-
release artery clamp first and view venous return before releasing this clip
-
if anastomosis leaking, wrap plastic background around artery, clipping it parallel to the vessel
-
wait five minutes and most leaks will have closed.
Bone fixation
This is best discussed separately for each recipient site, with the most important feature being protected stress on the fibula. If not, it will not hypertrophy (see Case 14 below). This applies especially to the lower limb.
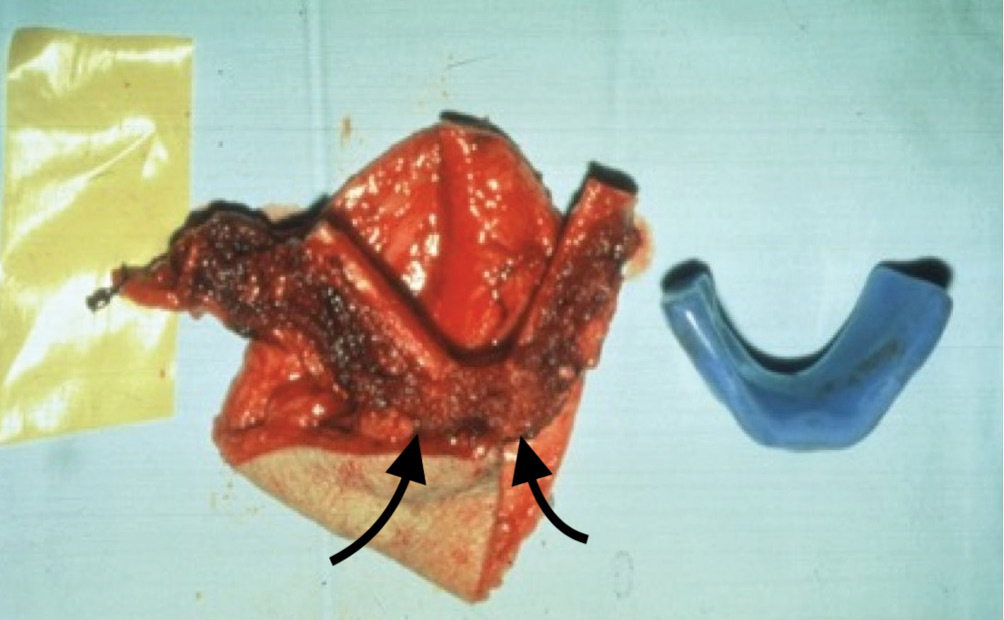
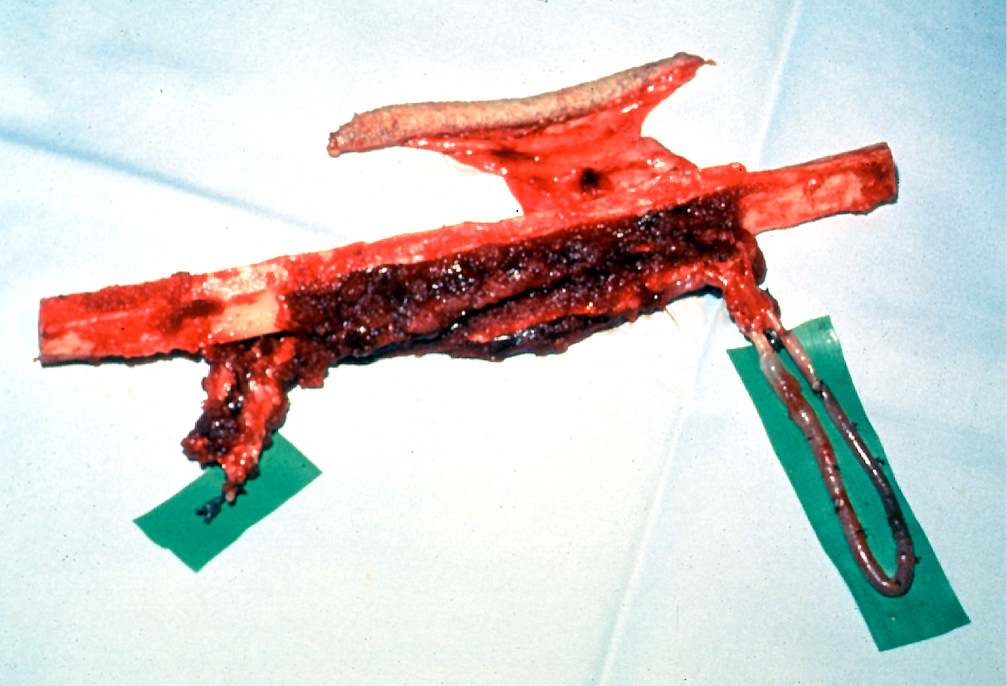
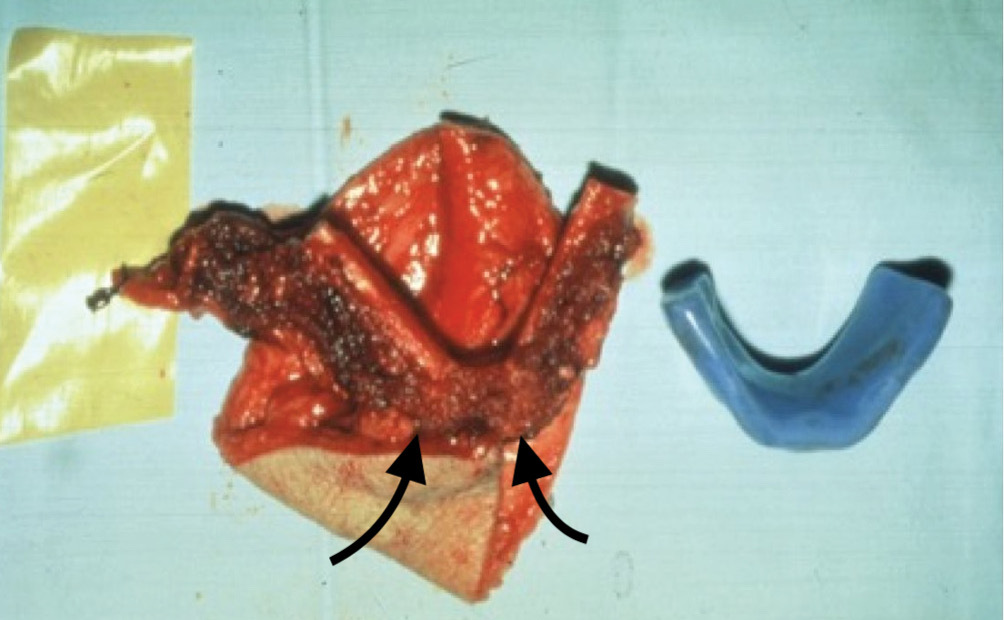
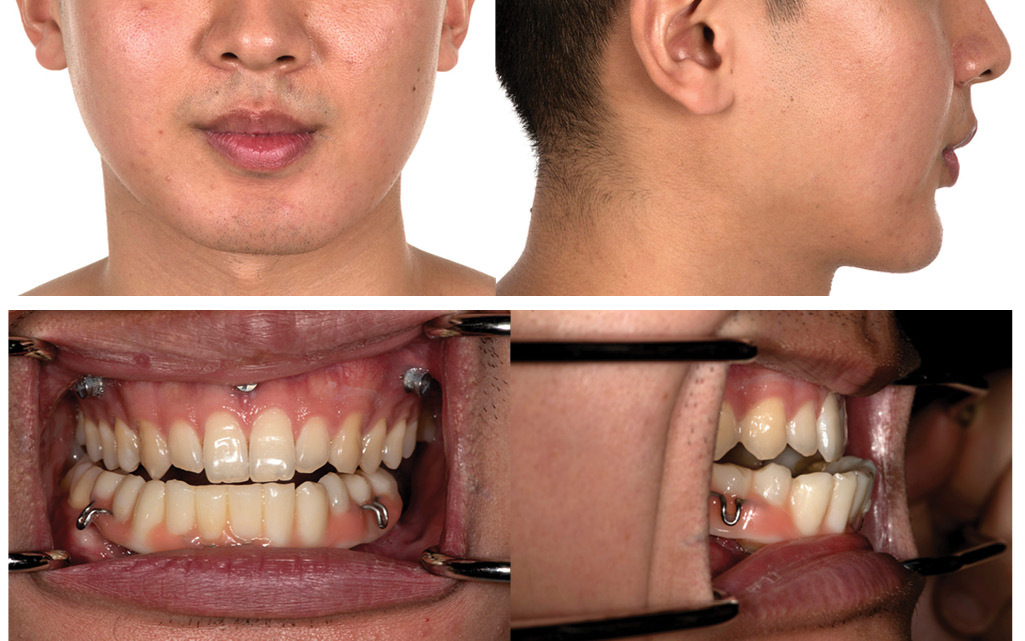
- The jaws: initially we confined the fibula to reconstruction of the bony arch of the mandible or maxilla. A range of acrylic models were used to match the shape of the removed or missing jaw segment shown in Case 5. Two bone wedges were removed from the inner surface of the fibula with an intermediate segment to recreate the chin and fixed with a single mini plate (Figure 24 and Figure 25).
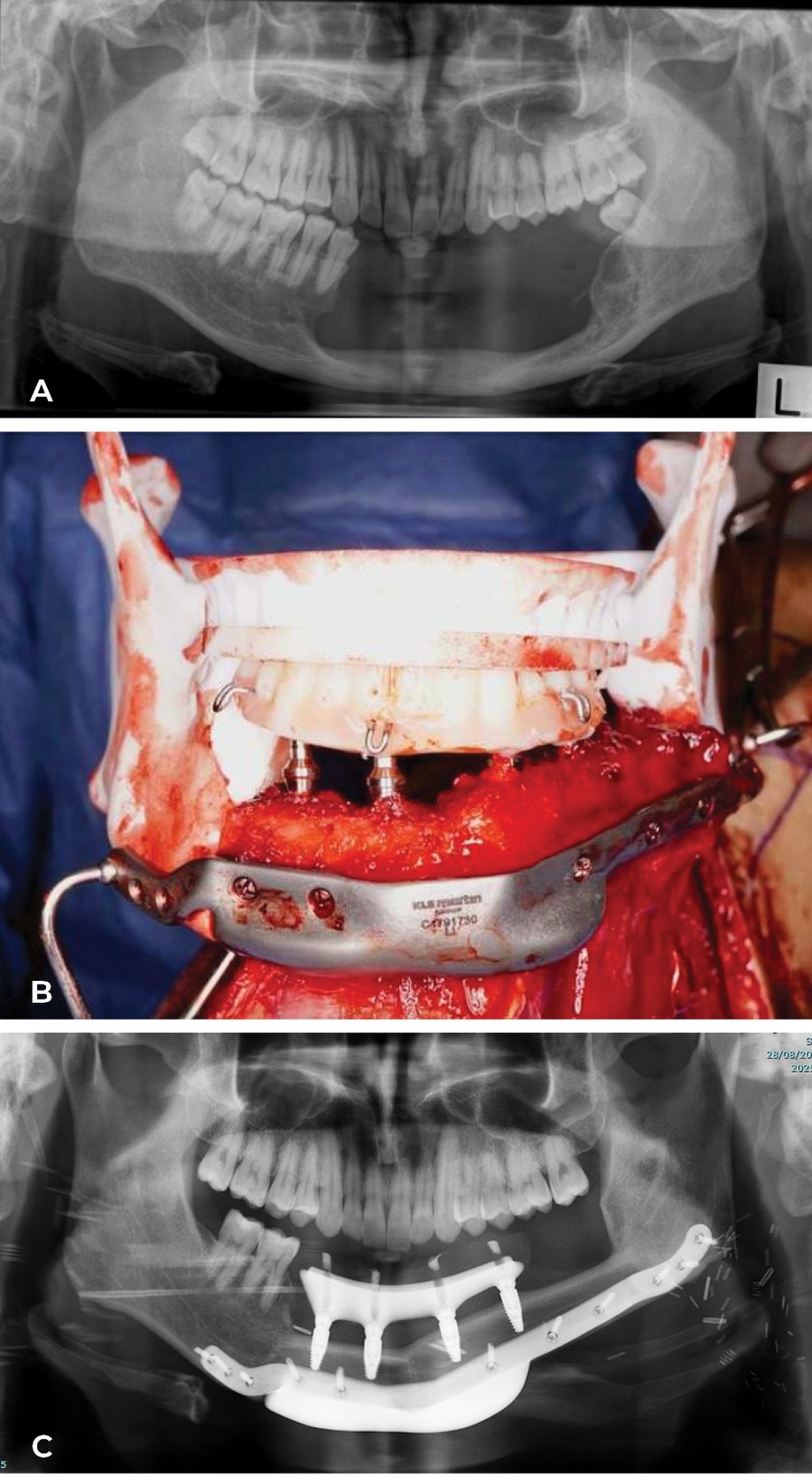
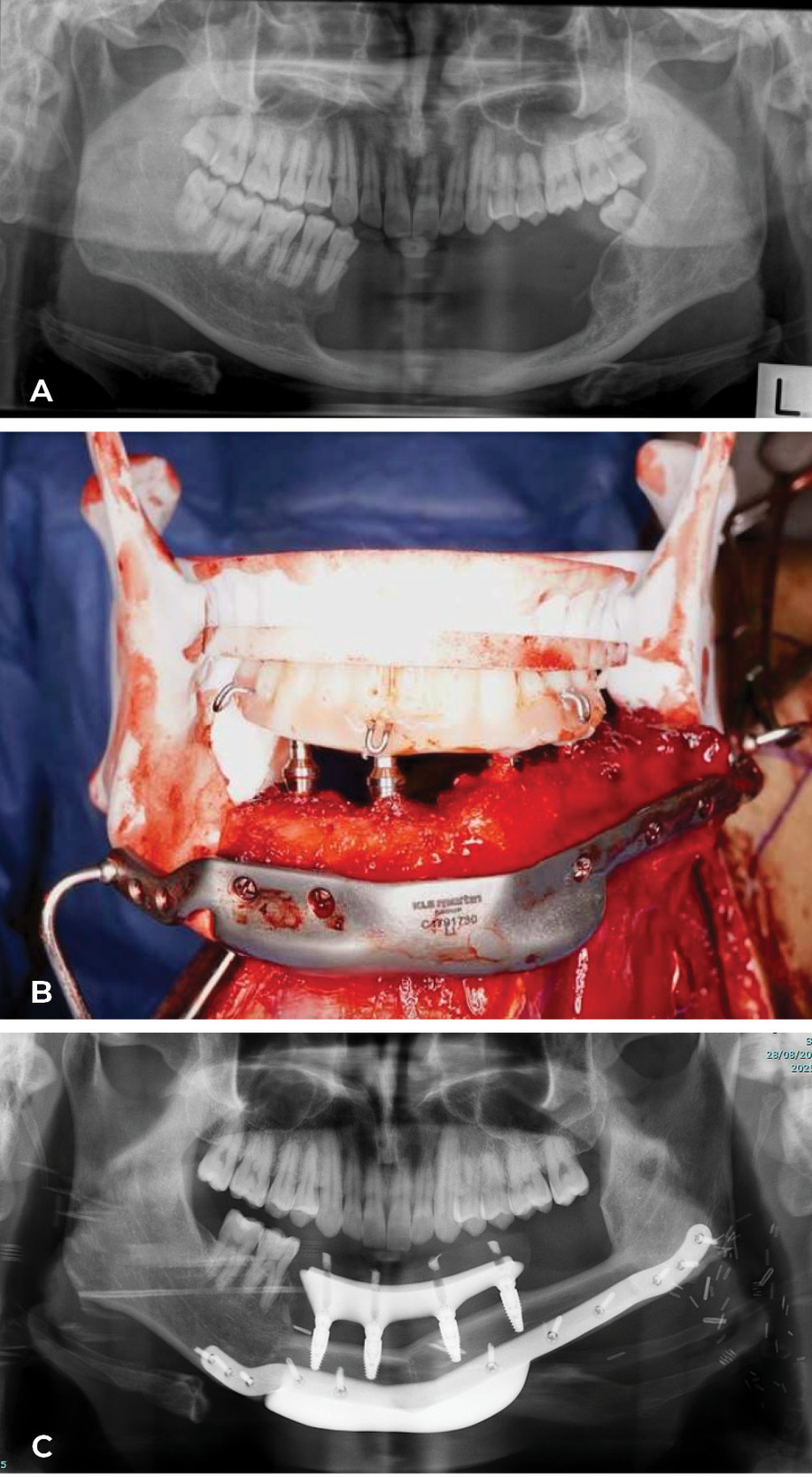
Today the ‘Model T Ford’ has changed shape at the Royal Melbourne Hospital. The computer (3D printing) is used to generate a replica of the fibula, selected after angiography, plus the patient’s jaw segment to be removed. Key osteotomies, with their site and angle, are designed on the fibula replica to reconstruct the shape of the jaw. In a case Ian watched in theatre, the fibula reshaping was done and fixed with plates while still attached in the leg. The fibula was detached, fixed in the mandible and dentures inserted at predetermined sites to match the occlusion of the upper jaw. The patient went to theatre with a tumour in the jaw and woke with a new set of teeth! A case done by Anand Ramakrishnan, Head of Plastic and Reconstructive Surgery and the team at the Royal Melbourne Hospital, is shown in Case 6 (Figure 26 and Figure 27). Combined with maxillofacial and oncological surgeons they now provide four separate teams a week at the Royal Melbourne Hospital to treat facial malignancy. In the last 10 years their total of fibula jaw reconstructions is 198.

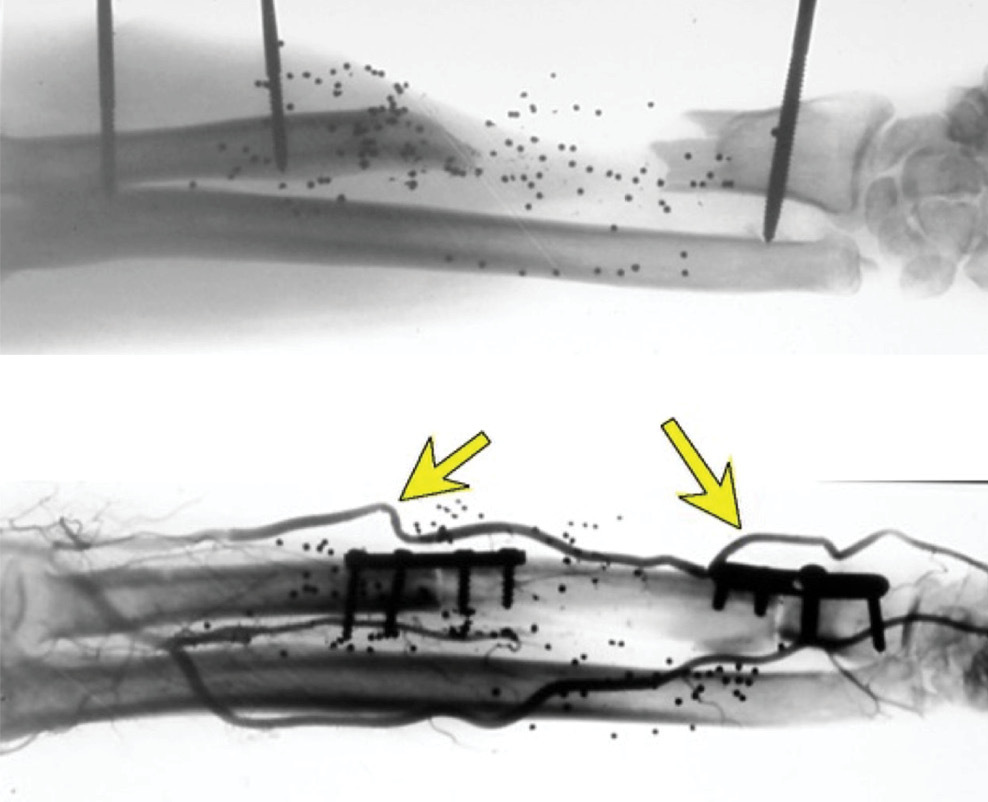
- The upper limb: the fibula matches the radius and ulna almost exactly with plates used at each end to fix the fibula in position. The stage is set then for a flow-through anastomosis at each end between the peroneal and recipient vessels shown in Case 7 (Figure 28). Vessel diameters match and if one fails the anastomosis at the other end may still prevail.
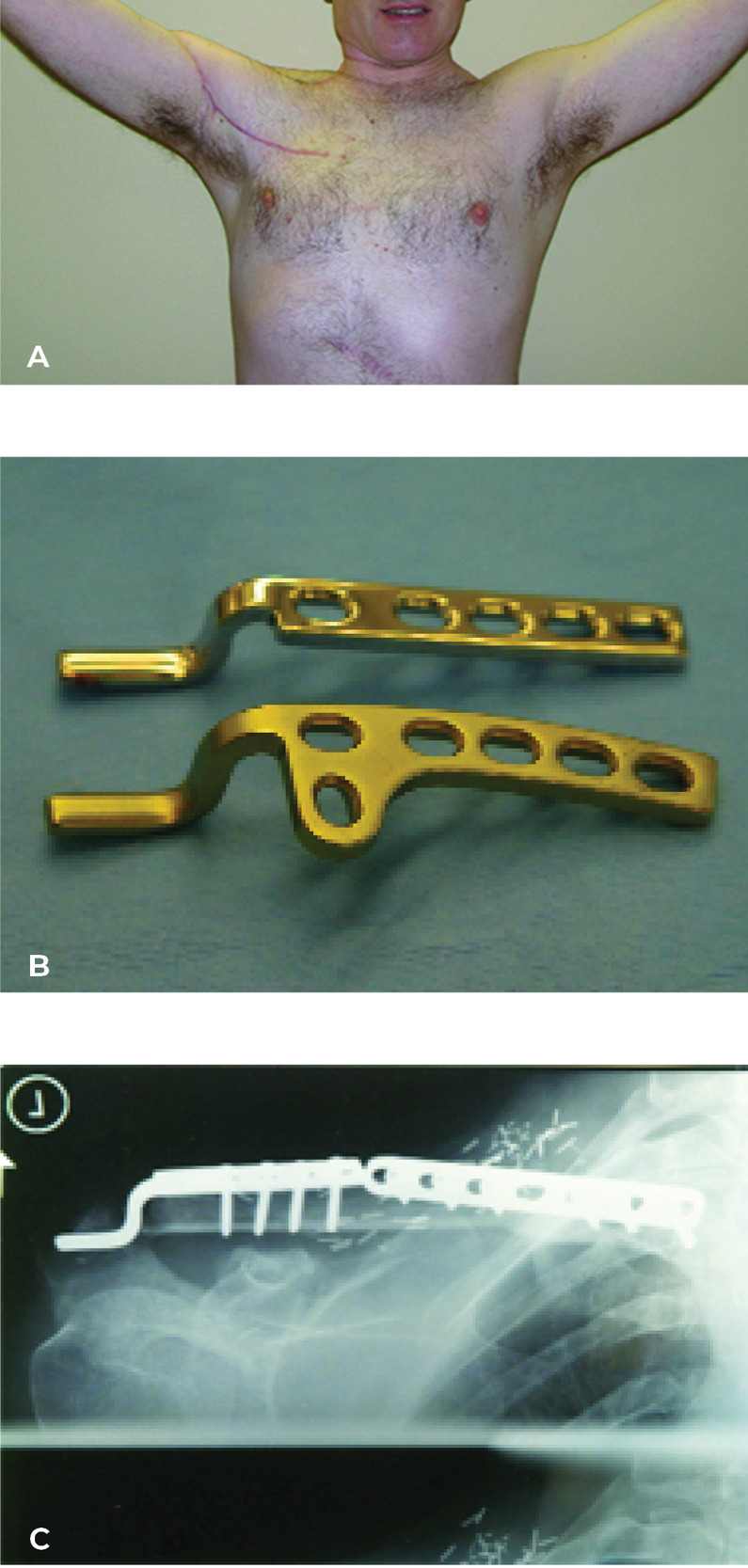
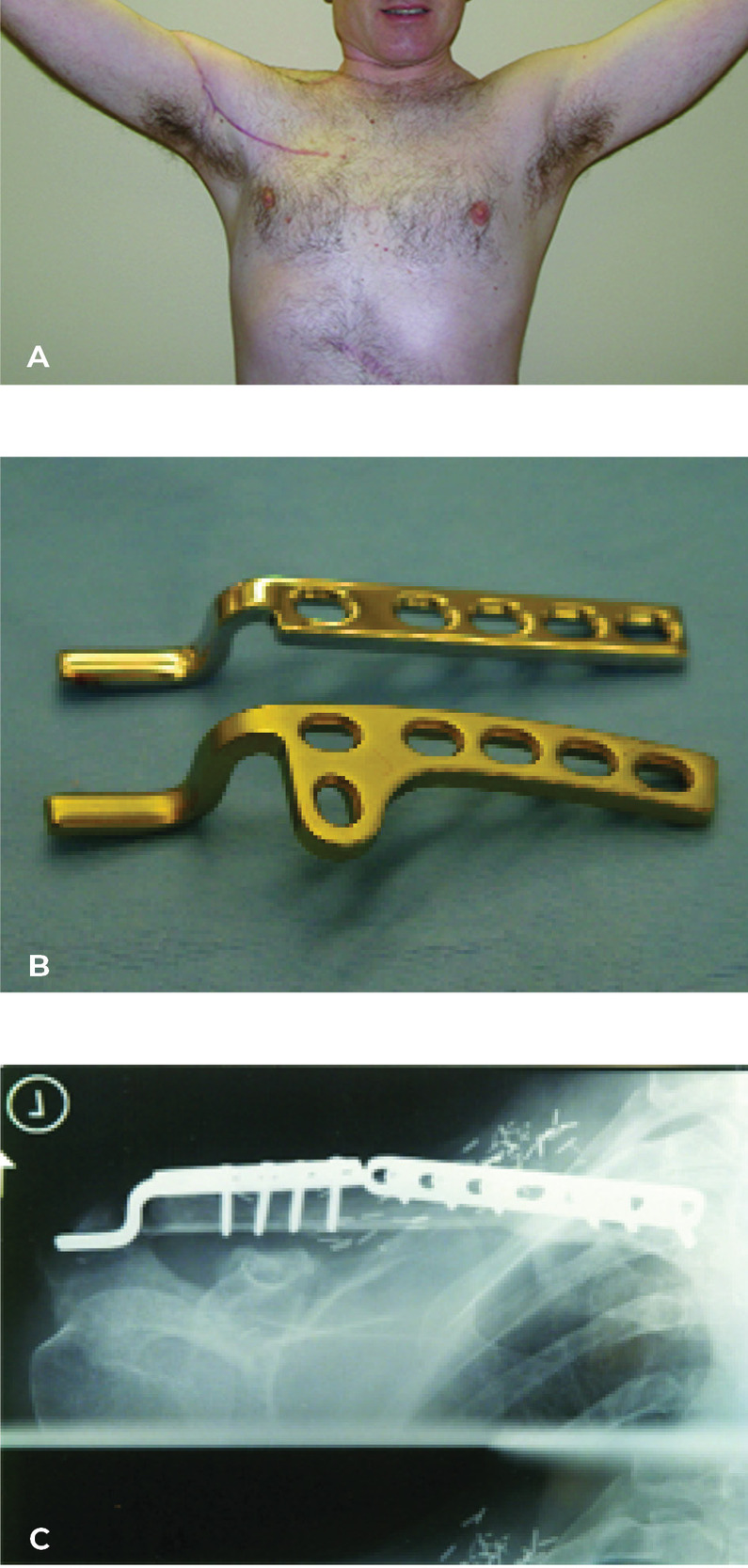
- The clavicle: just one case so far. But thanks to a close friend and engineer Fevzi Alakus, the curved Martin Richardson plate was reshaped to match the straight shape of the fibula and prevent subluxation of the acromioclavicular joint.19 A dermatofibrosarcoma attached to the clavicle was removed with an excellent result shown 10 years later in Case 8 (Figure 29).
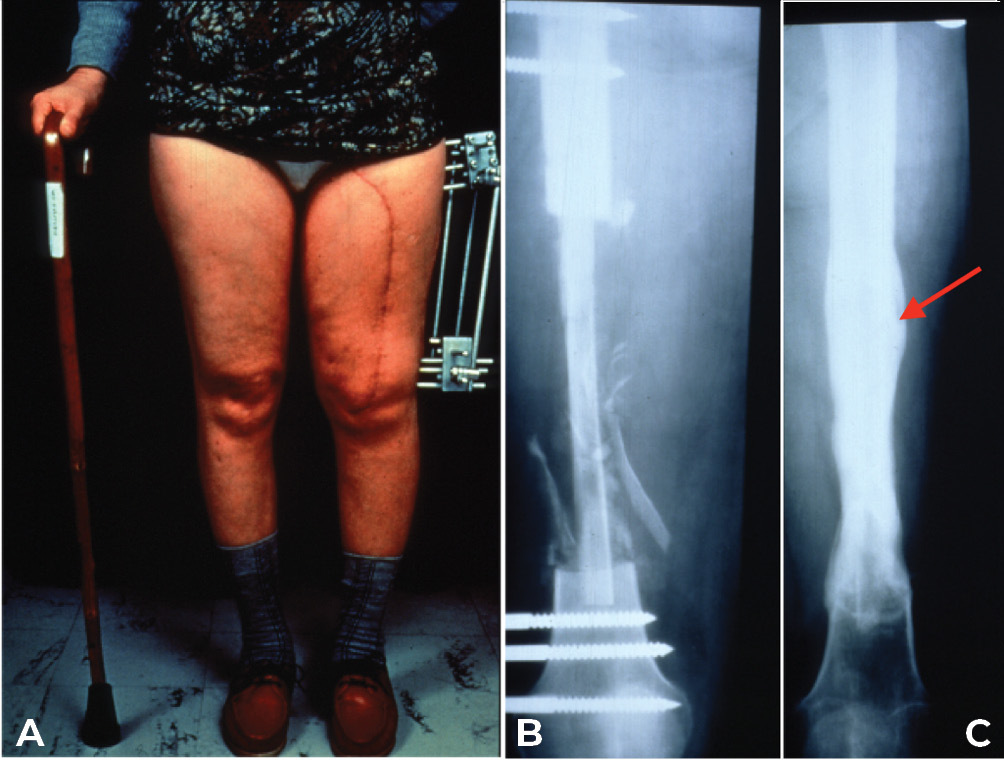
- The lower limb: This is where protected stress on the fibula in the line of weight bearing, is so important, otherwise it will not hypertrophy (see Case 14 below). This is why we always place the fibula within the medullary cavity of the recipient long bone. For the femoral shaft we choose an external fixateur. David Young, an eminent orthopaedic surgeon and a neighbour at the time, designed his fixateur for our first case. Pins are placed above and below the fibula after inserting it into the femur and sited to prevent it ‘telescoping’ within the recipient bone. Three parallel rods are attached to the pins, shown in Case 9, that can be released one at a time to allow stress on the transplant (Figure 30).
The same applies in the tibia, where the fibula is placed always within the medullary cavity of the bone. There it has been maintained again with the external fixateur or simply an above-knee plaster cast. Notably hypertrophy is frequently initiated by an undisplaced, often unidentified stress fracture as shown in Cases 1, 9, 10 and 11 (Figures 5, 30 and 31). If a specific fixateur is unavailable, in an emergency several transverse pins, a bit of bone cement and any nearby long metal rod or stick will do!
Another form of fixation is an intramedullary nail or rod used in two of our nine cases of resection of a pseudarthrosis of the tibia in a child shown in Cases 12 and 13 (Figures 32 and 33). In these two cases, the distal tibial fragment could not be fixed to the fibula with a screw. Instead a Rush nail was passed from below through the heel, calcaneum, talus and distal tibia and into the medullary cavity of the transplanted fibula. The result was exactly the same as the other seven cases. Even in plaster you can’t keep a child still! By six weeks all, including the two with nails, showed union and early bone hypertrophy (Figures 32 and 33).
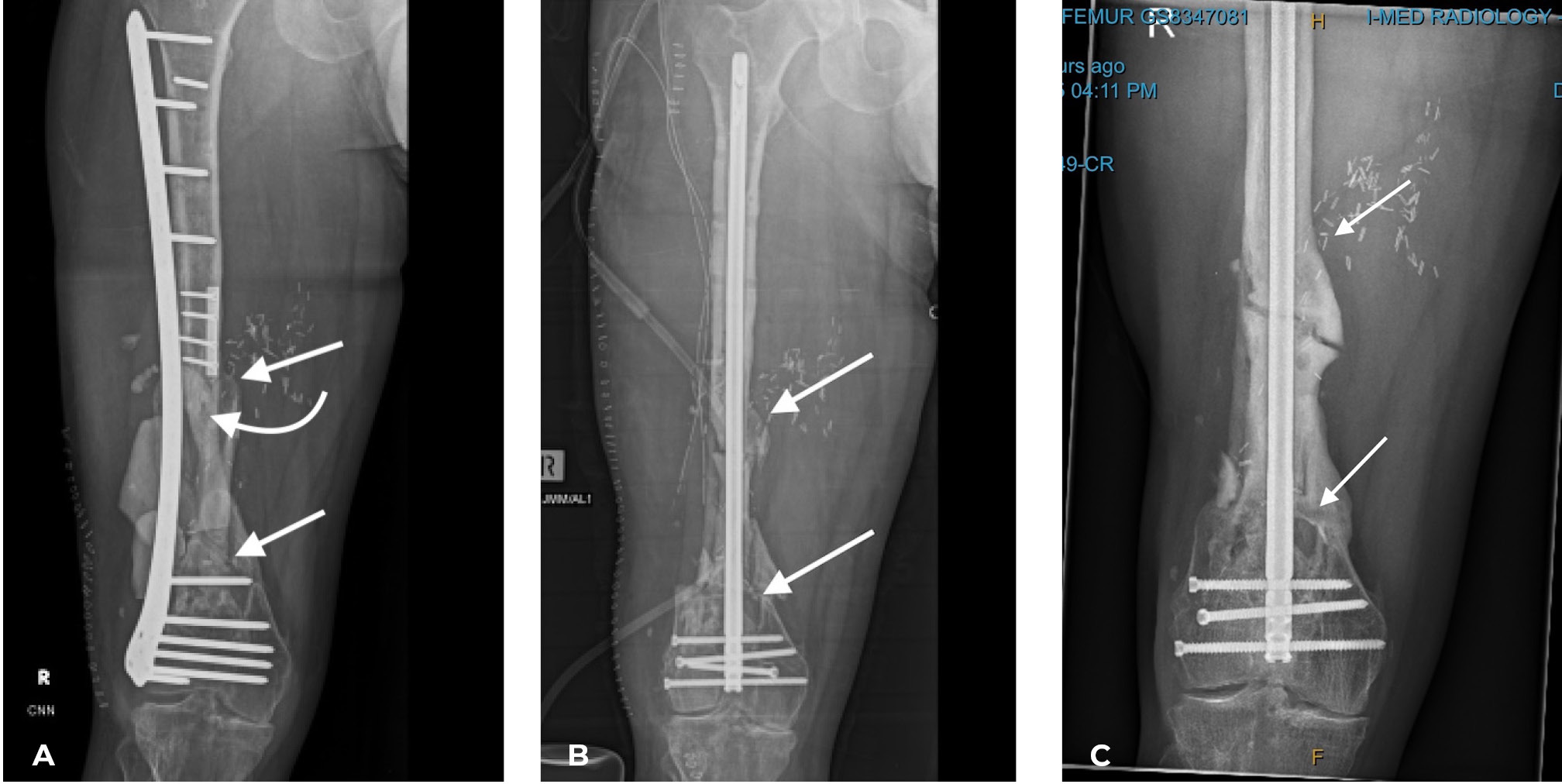
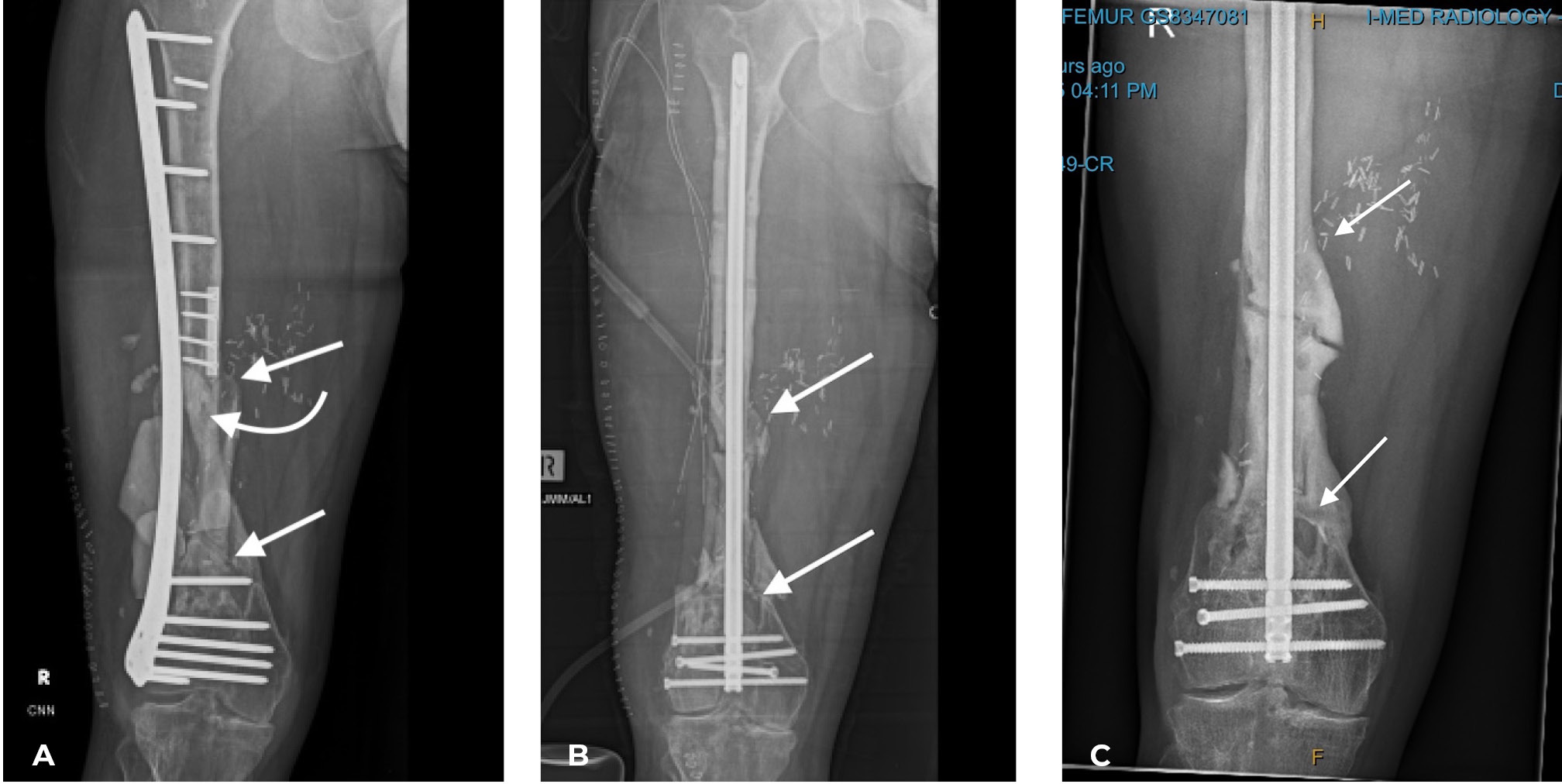
The importance of centralising the fibula within the medullary cavity of the femur or tibia is again reinforced by another case done at the Royal Melbourne Hospital. The fibula was used to reconstruct the femur but fixed rigidly with a plate and screws in Case 14 (Figure 34A). Twelve months later there was union but no sign of hypertrophy of the transplant. Then the plate broke. A Kuntscher nail was inserted from above and down through the medullary cavity of the fibula. It shattered forming a row of ‘bangles’ around the nail (Figure 34B). Two years later, having walked on his ‘box of bones skewered by the K-nail,’ he was located and the leg radiographed. Except for one level, there was union and hypertrophy of all bone bangles (Figure 34C).

If one stops to think, it is the periosteal supply to the fibula that is so important and the nutrient artery to the medulla is just a large one of these. Every time the mandible is reconstructed with a fibula the nutrient artery has been divided at each osteotomy site and relies totally on the periosteal supply. There is the need now for someone to review the range of Kuntscher and Rush nails or to reconstruct a new narrower Royal Melbourne Hospital nail, similar to the Kuntscher nail, to match the diameter of the medullary cavity of the fibula, maybe a TC (Taylor-Corlett) nail, thereby providing an alternative option to an external fixateur.
Another feature, revealed in this series in Case 3, is the behaviour of the transplanted fibular growth plate. It has grown at the same rate as if still in the leg. This genetic programming is a feature that we have noticed before with other free vascularised tissue transplants. For example, if lower abdominal tissue is transplanted to reconstruct the breast and the patient gains weight in the abdomen, that breast reconstruction will gain weight also! One of the most dramatic cases we saw that exhibited a similar genetic programming was a young woman in whom we transferred a groin flap to replace a burn scarred neck. We thinned this flap on two occasions giving a nice neck contour, then she became pregnant. She gained weight in her abdomen and so did our thinned neck flap. Then she delivered the baby, lost the weight in her abdomen and the neck flap returned to its thinned shape! More research is waiting.
Finally, we wish to mention a complication that occurred with our early fibula donor sites. Initially we repaired all muscle layers meticulously, being careful also to avoid encircling the posterior tibial nerve that occurred and had to be released in one case. The problem was a fixed flexion deformity of the great toe due to resuture of FHL. This was avoided by repairing the superficial tissues only, draining the deep spaces with suction, and applying a full plaster or a back slab to the foot with the great toe in extension. This was left for several weeks until the swelling subsided and prevented this complication thereafter.
Conclusion
Fourteen cases of patients with free vascularised fibula transplants are presented, selected from a series of 397. They embrace diaphyseal shaft transfer for the first time on the peroneal and then the anterior tibial arterovenous pedicle, followed by the first epiphyseal growth plate transfer on the latter vessels and especially its recurrent genicular branch. They demonstrate the use of the fibula to reconstruct the jaw, clavicle and long bones in the extremities.
Emphasis is placed on:
-
Preoperative planning including: angiography to detect damage, anomaly and the better donor limb; computer-generated models of the donor and recipient bones, especially for jaw reconstruction; incision markings for skin flaps after Doppler perforator studies; and vein grafts if the anticipated pedicle length would be too short and trial operations in cadavers.
-
Operative technique, especially patient warmth and operative positioning for an anterolateral dissection.
-
Bone fixation, especially in the lower limb where the fibula should be placed within the medullary cavity of the femur or tibia to allow protected stress on the fibula in the line of weight bearing with either a plaster cast, external fixateur or now it seems an intramedullary nail or rod as illustrated in the last two cases. If not the fibula will not hypertrophy.
With worldwide series now in the thousands and success rates in the high 90 per cents the fibula has emerged as the gold standard for major long bone defects and especially for mandibular reconstruction.
Acknowledgements
We wish to thank the ever reliable and indefatigable Prue Dodwell for help with this article, the Department of Anatomy and Neuroscience, University of Melbourne, the surgeons at the Royal Melbourne and Royal Children’s Hospitals Reconstructive Plastic Surgery, Maxillofacial Surgery and Orthopaedic Surgery Units. Graeme Miller and Frank Ham for their involvement with Case 1, Anand Ramakrishnan, co-surgeon Richard Barton, maxillofacial surgeon Felix Sim and prosthodontist Gordon Burt for Case 6, Rory Maher and Andrew Oppy for Case 14 (Figure 34) and Registrar Tetyana Kelly for help with Figures 26, 27 and 34, Cases 6 and 14. Thanks also to Levent Efe for Figure 6.
Figures 1, 2, and 3 are reproduced from Taylor GI, Miller G, Ham FJ. The free vascularized bone graft. A clinical extension of microvascular techniques. Plast Reconstr Surg. 1975:55(5);533–544. Figure 4 is from Taylor GI, Corlett RJ, Ashton MW. The evolution of free vascularised bone transfer: a 40-year experience. Plast Reconstr Surg. 2016:137(4);1292–1305. Figures 8, 9, 10, 11, 13, 14, 15 and 16 are from Taylor GI, Wilson KR, Rees MD, Corlett RJ, Cole WG. The anterior tibial vessels and their role in epiphyseal and diaphyseal transfer of the fibula: experimental study and clinical applications. Brit J Plast Surg. 1998:41(5);451–469. Figures 17, 21 and 22 are from Taylor GI, Pan WR. The angiosome concept and tissue transfer. Dodwell P, associate ed, CRC Press, Thieme Publishers, 2013. Included in this volume is a CD that shows four cases of lower limb reconstruction, including Case 1 in this article using the fibula and iliac crest as well as Jaws IV, a film showing DCIA reconstruction of the mandible.
The first fibula transplant, performed on 1 June 1974 was published in The American Journal of Plastic Surgery the following year in May 1975. In that issue the editor, Frank McDowell printed an editorial entitled20 ‘The free living bone graft’ stating that Taylor, Miller and Ham report the first successful, clinical free transference of assuredly living bone (in this instance, from one fibula to bridge a gap in the opposite tibia) by microvascular anastomoses. The following year it received The James Barrett Brown Award by the American Association of Plastic Surgeons presented at their Meeting in Atlanta, for the best paper published in Plastic and Reconstructive Surgery for the preceding year, 1975.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.
Revised: December 11, 2025 AEST