Background
Osteoradionecrosis (ORN) is a severe complication of radiotherapy for the management of head and neck malignancies in which there is exposure of irradiated bone that fails to heal for three months.1 Fundamentally, ORN is a problem of impaired and inadequate cellular turnover and impaired wound healing.2 One key theory proposed by Marx1 for the pathogenesis of ORN describes radiation-induced hypoxia, hypovascularity and hypocellularity as the precursor to tissue necrosis. Radiation-induced dysregulation of fibroblast and osteoblast activity has also been proposed to result in necrosis via the deposition of fibrotic tissue susceptible to breakdown.3 Exposure to radiation also generates reactive oxygen species, and the resulting oxidative stress may contribute to impaired cellular repair mechanisms and exacerbate the fibrogenic response.3 Risk factors for ORN of the head and neck region include tumour site, stage, presence of bone invasion, and radiation dose and duration.4,5
The scalp and calvarium play an important role in the protection of the brain, and therefore it is vital that ORN of the calvarium is managed early and effectively. Patients with ORN of the calvarium may be generally asymptomatic and identified incidentally, or may present clinically with headaches, pain and discharge from the overlying scalp wound.6 Management of ORN depends on the extent of the disease. In the early stages it can be managed conservatively with intravenous antibiotics, wound debridement and hyperbaric oxygen therapy (HBOT).2 Established ORN with bone necrosis and overlying soft tissue defects, however, necessitates radical debridement and reconstruction of the resulting defect with healthy vascularised tissue.2 This reconstruction is often best achieved with a microvascular free flap from a distant site (unaffected by radiation), which has been associated with high success rates (86–100%) in reconstructing defects resulting from maxilla or mandible ORN.7,8
Most literature on the incidence, evolution and treatment of ORN relates to maxilla, mandibular, temporal bone or skull base ORN as sequelae of radiotherapy for mucosal head and neck cancers. On the other hand, ORN of the calvarium and associated scalp wounds following radiotherapy for cutaneous scalp and intracranial malignancies are frequent occurrences in clinical practice, but are less widely studied. Literature relating to ORN of the frontal, parietal and occipital bones is particularly sparse.6 This systematic review examines the literature to date on the management of ORN of the calvarium in patients who have had radiotherapy for non-mucosal head and neck cancers.
The primary objective of this systematic review is to investigate the risk factors, management and treatment outcomes for patients with ORN of the calvarium.
Methods
Search strategy
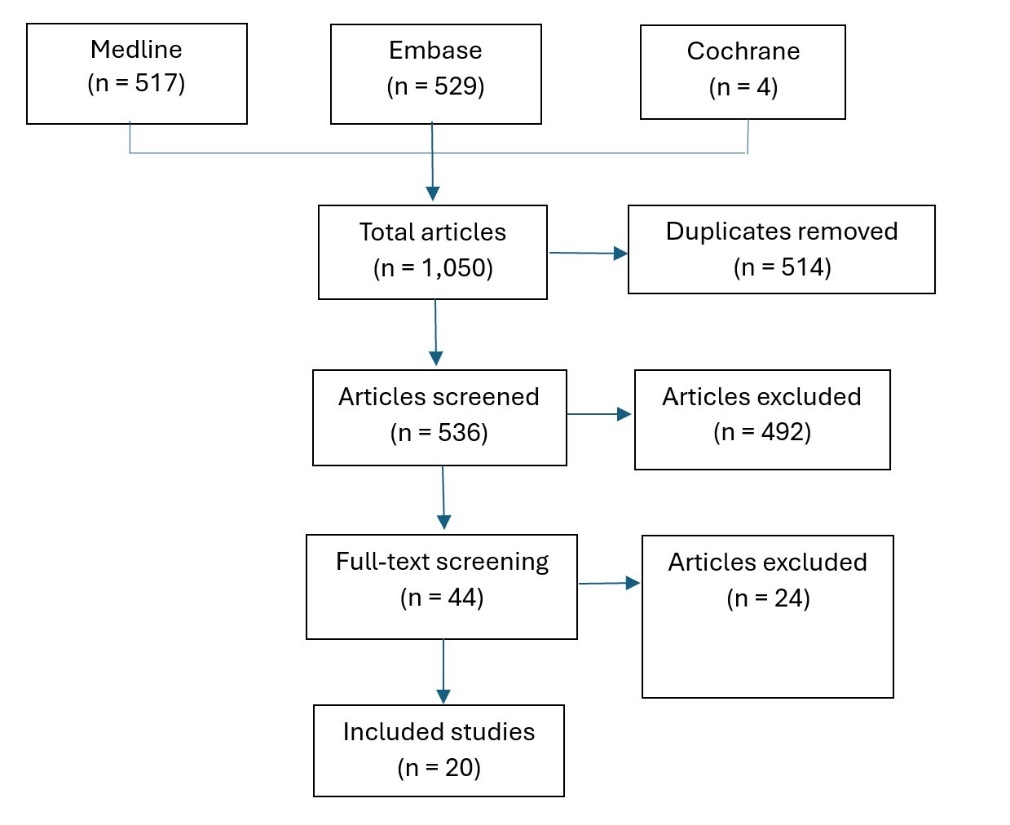
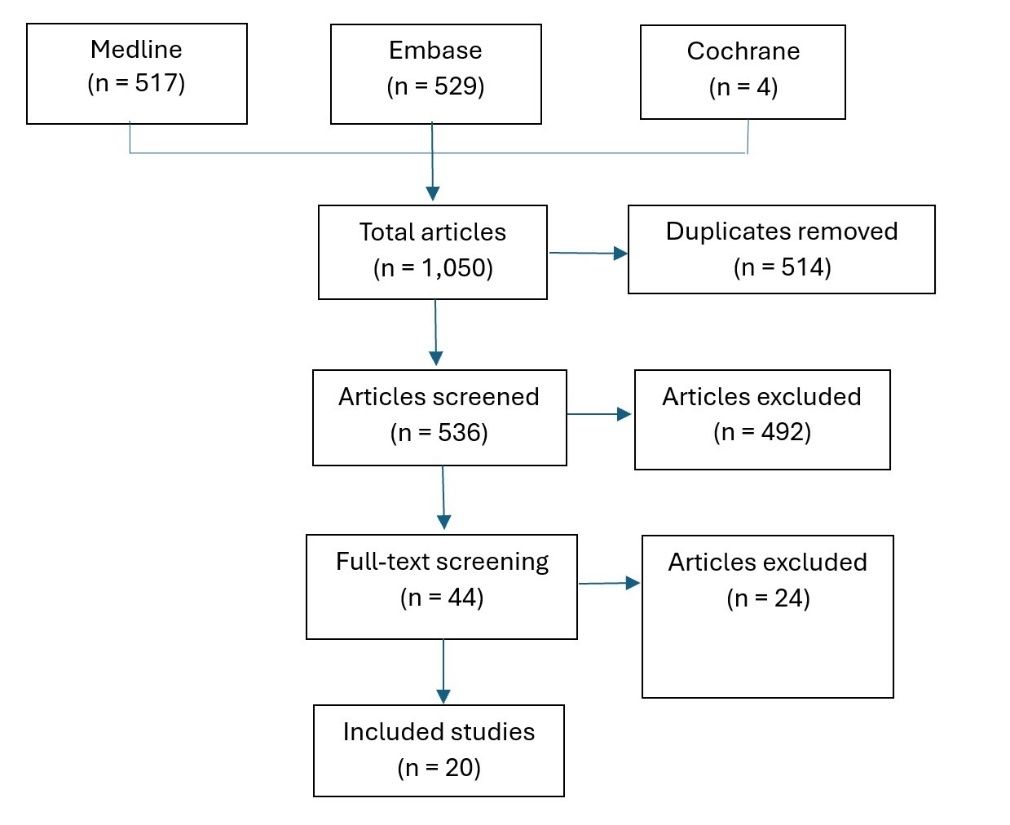
In accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines,9 we conducted a comprehensive search of the literature to identify studies relevant to the risk factors and management of ORN of the calvarium. Two researchers performed a computerised search via Ovid of MEDLINE, Embase and the Cochrane Library for studies on the subject of calvarial ORN with the following key words: ((osteoradionecrosis OR ((radiation OR radiotherapy) AND necrosis))) AND (skull OR cranium OR scalp) AND (malignancy OR carcinoma OR cancer OR sarcoma). Papers on mandibular ORN were excluded with the additional key words: NOT mandible and NOT jaw. Studies that were published up to and including 1 June 2024 were included. Appraisal of titles, abstracts and full text articles was conducted by two independent reviewers. This review was not prospectively registered.
Eligibility and exclusion criteria
Studies with patients of any demographic who developed ORN of the calvarium (frontal, parietal and occipital bones) following radiotherapy were included. All surgical and conservative approaches to treatment of calvarium ORN were included. All study methodologies were included, and there were no restrictions on study location or publication language. Studies which exclusively examined mandible, skull base or temporal bone ORN were excluded.
Data collection
Two independent researchers analysed all full-text articles that met the inclusion criteria. Key data collected included study type, number of subjects with calvarial ORN, underlying pathology and radiotherapy details, key patient demographic details and method of surgical reconstruction or other management. Any complications resulting from the management of calvarial ORN reported in any study were recorded independently by the two researchers and collated after each researcher had completed their analysis. Studies were assessed independently for methodological quality and risk of bias using a combination of the Methodological Index for Non-Randomised Studies (MINORS) criteria and the Joanna Briggs Institute (JBI) checklists for case reports and case series. Data from all included studies were collated including key demographics, radiotherapy treatment details prior to the development of calvarial ORN, the common surgical and conservative treatments of the condition, and the complications associated with different treatment modalities.
Results
A total of 1050 studies were initially screened by title and abstract; after removal of duplicates and full-text screening, 20 studies10–29 were included in the review (Figure 1). These studies involved a total of 79 patients with a mean age of 52.9 years, of whom 42 were male. The included studies comprised one cohort study, 11 case series and eight case reports, with an overall quality assessed as low to moderate based on MINORS criteria; however, case series and reports scored favourably when assessed using the JBI checklists specific to these study designs (see Table 1 for a summary of study characteristics).
Osteoradionecrosis primarily affected two patient populations: those with skin malignancies (n = 33), mainly squamous cell carcinoma (SCC, n = 24), and patients with brain tumours (n = 34) who underwent craniotomy and adjuvant radiotherapy. The pathologies reported included SCC, melanoma, basal cell carcinoma, astrocytoma, medulloblastoma, glioblastoma and rarer conditions such as atypical fibroxanthoma and haemangioma, though some studies did not specify the pathology.
The mean radiotherapy dose was 44.88 Gy, with a range of 14–160 Gy, administered over an average of 26.81 fractions. Fourteen patients received multiple courses of radiotherapy. The latency between radiotherapy and the onset of ORN averaged 4.2 years (excluding an outlier with likely delayed diagnosis of ORN at least 70 years after radiotherapy), ranging from six months to 70 years.
Management strategies varied widely (Table 2). Approximately one-third of patients were treated conservatively with debridement and dressings, while 24 per cent received HBOT as part of their management. Surgical interventions were performed in about half of cases, including cranioplasty (most commonly with titanium mesh) and soft tissue reconstruction. Twenty-eight patients underwent free flap reconstruction (two requiring more than one free flap), with the anterolateral thigh and latissimus dorsi flaps being the most commonly used. Among patients who underwent surgical management, 10 patients required multiple revisions due to wound dehiscence, infection or failed reconstructions. Four patients ultimately required removal of their cranioplasty and secondary free flap reconstruction.
Conservative management appeared to yield low rates of intracranial infection; however, healing times were inconsistently documented across the studies. Table 3 provides an overview of the management strategies of calvarial ORN documented in the 20 studies reviewed and summarises the treatment complications.
Discussion
Osteoradionecrosis of the calvarium is a late complication of radiotherapy that is rare but it can have a significant impact on patients. It is defined as exposed irradiated bone that fails to heal over a three-month period (or two-month period in Weerakkody and colleagues29) without the recurrence of local neoplastic tissue.1 Most commonly ORN affects bones with a low intrinsic blood supply, most notably the mandible. It can also involve the calvarium; however, reports of calvarial ORN in the literature remain limited.19,29
Advancements in irradiation techniques and protocols for managing head and neck cancers have led to a decline in the incidence of craniofacial ORN. Nevertheless, it remains a substantial source of morbidity for patients undergoing high-dose radiotherapy, often presenting significant challenges for surgical reconstruction.15 Management of calvarial ORN is particularly complex due to the advanced age and high comorbidity burden of affected patients, which increase perioperative risks. A better understanding of the incidence and associated risk factors for calvarial ORN is essential to identify high-risk patients and develop effective prevention strategies.19,29
The incidence of calvarial ORN reported by Weerakkody and colleagues is approximately 8 per cent.29 While no other cohort studies have specifically examined the incidence of calvarial ORN, this figure is comparable to the reported rates of mandibular ORN, which range from 5–15 per cent.30 Two distinct patient populations appear to be at higher risk of developing calvarial ORN. The first includes patients with scalp skin malignancies, particularly SCC. The second group comprises patients who have undergone craniotomies for brain tumours. Unlike the mandible, which has inherently poor blood supply, the scalp is highly vascularised and would theoretically exhibit resistance to devascularisation; however, the incidence of ORN in the calvarium is comparable to other subsites. In craniotomy patients specifically, the elevation of a bone flap disrupts the vascular supply to the affected segment. Subsequent radiotherapy further compromises the bone’s integrity, placing these patients at particularly high risk for developing ORN.16
Weerakkody and colleagues29 identified several risk factors for the development of calvarial ORN. These include a strong association between cumulative radiotherapy dose, higher fraction counts, and the likelihood of developing ORN. Interestingly, tumour size and stage were not associated with the development of calvarium ORN, in contrast to studies of mandible ORN.4,5 Additionally, the method of reconstruction following initial treatment influences risk. Patients who underwent skin grafting were found to have a higher likelihood of ORN compared to those who received more robust reconstructive approaches, such as local or free flap coverage.
Another significant risk factor for cranial ORN is a history of craniotomy. While ORN typically does not occur at radiation doses below 50–60 Gy, a study by Kim and colleagues16 demonstrated that ORN can develop at doses as low as 30 Gy in patients who have undergone craniotomy. This increased vulnerability may stem from the compromised healing capacity of the bone flap, as the process of creating the flap detaches it from the dura, periosteum and surrounding cranial bone, disrupting its vascular supply. This highlights the compounded risk for patients receiving radiotherapy following craniotomy, emphasising the need for tailored preventive measures and close monitoring in this population. This review also demonstrated that calvarial ORN can develop at varying intervals following radiotherapy.16 The median time to ORN onset is reported as 4.9 years, with a range from 0.5 to 70 years. This latency period is consistent with that observed for mandibular ORN, underscoring the need for long-term follow-up and proactive screening in high-risk patients.15
The literature supports radical surgery for treating osteoradionecrosis (ORN), with conservative treatment failing in 70–83 per cent of cases.15 Hyperbaric oxygen therapy is often considered a logical treatment option for ORN due to its ability to enhance tissue oxygenation and promote healing; however, its clinical efficacy remains contentious, particularly in advanced stages of the disease.15 The evidence supporting HBOT is limited; a randomised controlled trial by Annane and colleagues31 in 2004 demonstrated no benefit for HBOT in the treatment of patients with mandibular ORN, although anecdotal reports suggest it may aid wound healing when used as an adjunctive treatment.
Hyperbaric oxygen therapy has shown potential in improving soft tissue healing in irradiated wounds, potentially by enhancing vascular remodelling and reducing thrombosis within the radiation zone.11 Despite these theoretical advantages, the treatment is associated with significant practical challenges. The logistical demands of repeated sessions can be burdensome for patients, and the therapy also carries risks of complications, including middle ear dysfunction, tension pneumothorax, seizures, pulmonary alveolar collapse, arterial gas embolism and exacerbation of acute viral infections.11,15 While HBOT may have a role in select cases, particularly in early or less severe ORN, its utility in advanced disease remains uncertain, warranting further investigation to establish its efficacy and cost-effectiveness.
Conservative treatment regimens are demanding and resource-intensive. For instance, one study19 outlined a protocol involving daily wound cleaning with soap and water, application of petroleum ointment, quarterly follow-ups, bedside debridement of necrotic bone during each visit, wound cultures, and treatment with oral antibiotics and topical gentamicin 0.3 per cent solution when indicated. Despite the risks of severe infections such as osteomyelitis, cranial abscess and meningitis, the reported infection rates in conservative treatment cohorts were surprisingly low. However, no studies documented the exact time required for complete wound healing, which can span months to years.
While local debridement and dressings may be effective in some cases, failure to achieve resolution should prompt consideration of radical surgical approaches. Radical debridement followed by free tissue transfer is particularly effective in advanced ORN and has been shown to provide superior outcomes in terms of efficacy and cost-effectiveness compared to prolonged conservative management.15
Kelishadi and colleagues15 reported that most patients with craniofacial ORN who initially underwent conservative therapy ultimately required radical resection and free flap reconstruction. The total cost per patient averaged US$55,040, with nearly half of this cost attributable to failed conservative management. Earlier implementation of definitive surgical intervention may reduce costs and shorten treatment duration. Developing clear guidelines to classify ORN severity and guide the choice between conservative and surgical management could optimise outcomes and resource utilisation, ensuring that patients with advanced disease receive timely, cost-effective treatment.
We acknowledge several limitations of this review. Most of the data reviewed are derived from case series and case reports, with only one cohort study available. Additionally, no randomised controlled trials comparing outcomes of conservative versus surgical treatment for calvarial ORN exist in the current literature. As a result, the findings are potentially influenced by confounding factors and biases. A review is limited by the evidence presented in its included studies and these do not address a number of important considerations in the evaluation and treatment of calvarial ORN. For instance, these studies did not provide evidence relating to patient demographics, comorbidities or the specific anatomical location of ORN (eg, watershed areas of the scalp) as potential independent risk factors for ORN, and there was insufficient data available to allow these factors to be assessed in this review. Future studies are needed to provide clear diagnostic and management algorithms for calvarial ORN, including assessment of the extent of bony involvement. Clear evidence-based guidelines are needed for staging ORN of the calvarium and to elucidate indications for cranioplasty, the precise extent of bony resection and the modality of soft tissue reconstruction associated with the best patient outcomes in specific patient populations.
In addition to the paucity of high-quality evidence available to inform the management of calvarial ORN, the significant variability and heterogeneity in methodologies of the studies presented here complicated data synthesis and interpretation. Study methodologies, patient demographics, types of reconstruction or conservative management, and follow-up periods varied widely between studies and precluded valid comparisons between studies or meta-analysis of the effectiveness of different treatments for calvarial ORN. To overcome these limitations, future research should focus on larger, prospective, multicentre studies with standardised data collection and reporting protocols, and work towards a nuanced and clinically useful treatment algorithm for the management of patients with calvarial ORN.
In summary, we advocate for the early identification of patients at risk of developing ORN, ensuring they receive long-term follow-up due to the latency of the condition. Robust reconstruction methods, such as locoregional or free flap coverage, should be considered in patients undergoing adjuvant radiotherapy to mitigate the risk of ORN. There is a clear need to develop evidence-based guidelines for staging the severity of ORN, which would aid in determining the appropriateness of conservative versus surgical management. This approach would help ensure that patients with advanced disease receive timely surgical intervention, avoiding unnecessary costs and delays associated with prolonged conservative treatment.
Conclusion
Calvarial ORN is an under-reported but serious late complication of radiotherapy to the scalp. Based on the findings of this review, we advocate for early identification of patients at risk of developing ORN to ensure effective long-term follow-up and early intervention. Early robust locoregional or free flap reconstruction in appropriate patient populations should be considered in patients undergoing adjuvant radiotherapy to mitigate the risk of ORN; however, there is currently insufficient evidence to elucidate the best management for established ORN. Further prospective, randomised trials are required to provide vital information on the key risk factors and most effective management of ORN of the calvarium to inform best practice in the prevention and treatment of these patients.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship and/or publication of this article.
Revised: August 31, 2025 AEST