Introduction
Rhinoplasty has become increasingly popular in many countries, particularly in Iran.1 Rhinoplasty is a complex procedure with the ultimate goal of improving both the function and appearance of the nose while enhancing quality of life.
It is crucial to evaluate the outcomes of surgeries based on patient satisfaction and quality of life, particularly in the field of plastic surgery. There is an increasing interest in self-reported outcome evaluation in plastic surgery, with facial plastic surgery being one of the most significant areas of research.
Rami Alsarraf developed the Rhinoplasty Outcomes Evaluation (ROE) questionnaire based on the concept that patient satisfaction after facial aesthetic surgery is influenced by physical, emotional and social factors.2
Evaluating the satisfaction of patients who undergo rhinoplasty can be time-consuming, especially when multiple consultants are involved. To simplify this process, a standardised questionnaire called the Rhinoplasty Outcome Evaluation (ROE) was used.3 This questionnaire is a reliable and efficient tool for evaluating the quality of life after rhinoplasty and measures various aspects such as social, emotional and psychological factors.4
In this study, we aim to compare the satisfaction of patients assessed by ROE, based on when they saw the rhinoplasty results.
Method
The ROE questionnaire has been translated and adapted based on criteria established by Guillemin and colleagues.5 We used the previously validated version of the questionnaire.6,7 The questionnaire consists of six questions, each with five answer options graded from zero to four. Therefore, the total satisfaction score of the questionnaire can range between zero and 24.
During pre-surgical consultations, patients were informed in detail about the expected postoperative course, including transient swelling, nasal tip stiffness, bruising and asymmetry. They were specifically advised not to take off the nasal tape and splint, nor to look at a mirror before their assigned viewing time. Close family members were encouraged to participate in the discussion and cooperate with these instructions.
To mask the rhinoplasty results, post-surgery all patients were covered with standard nasal splints and excessive amounts of adhesive tape, which remained in place until the physician performed the first dressing change. Patients visited the hospital for each tape change, which was done in an environment designed to prevent them from seeing their results. A single physician was responsible for performing the tape changes during hospital visits. To maintain the integrity of the study, strict protocols were enforced, which included the prohibition of mirrors and photography in settings where only the physician and the patient were present. This ensured that no external influences or feedback could affect the patients’ perceptions of their condition.
After rhinoplasty, we randomly selected patients and divided them into two equal groups. The data analyst was blinded to the group assignments, ensuring impartiality in the evaluation. One group viewed their results one week after the operation, while the other saw their results two weeks after the procedure. This staggered approach aimed to assess the effects of time on patient perception and reaction. The ROE was administered three months postoperatively to assess whether long-term satisfaction was influenced by the timing of the initial viewing.
This study was approved by the ethics committee of Shahid Beheshti University of Medical Sciences (No: IR.SBMU.RETECH.REC.1402.189). The study protocol was in accordance with the Declaration of Helsinki. All patients who participated in the study were informed about the process and the purpose of the study, and their written consent was obtained.
RStudio (v 2025.09.1+513, Posit Software, PBC, Boston, MA, USA) was used for statistical analysis. Descriptive variables were reported by frequency and percentage. The quantitative variables were demonstrated by means and standard deviation.
The Shapiro–Wilk test was used to assess the distribution of data. If the data was normally distributed, an independent t-test was conducted; otherwise, the Mann–Whitney U test was performed. A p-value less than 0.05 was considered significant.
Results
Sixty consecutive patients were included in this study. Patients were randomly divided into two groups of 30 people each. Each group consisted of 23 females (76.6%) and 7 males (23.4%). The mean age of included patients was 24.57 ± 2.64 (ranging from 20–30 years). The age of the patients was normally distributed and did not differ significantly between the two groups.
The mean of each question in the ROE is listed in Table 1. The difference between the two groups was assessed by Mann–Whitney U test.
As demonstrated in Table 1, patients who viewed the result of the rhinoplasty after two weeks had higher satisfaction in their appearance, breathing and nose looking as good as it could.
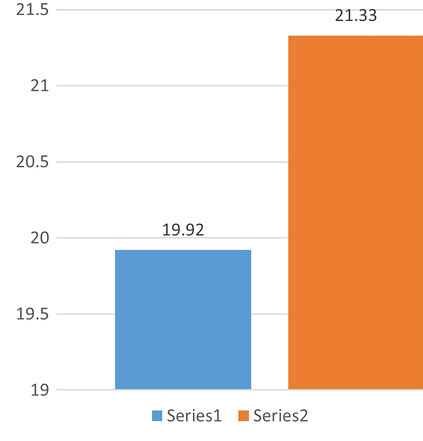
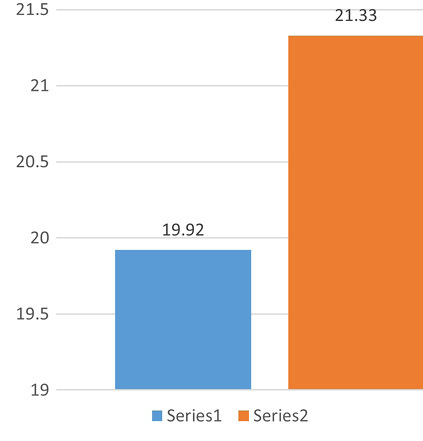
The total scores of the two groups were compared by the Mann–Whitney U test. The results revealed that the patients who viewed their appearance after two weeks had a higher level of satisfaction (p-value = 0.02407). The mean ROE scores are illustrated in Figure 1.
Discussion
Rhinoplasty is one of the most common and technically demanding procedures in plastic surgery. This is because the surgery can impact three distinct aspects of the patient: appearance, functionality and psychological wellbeing.8 Beyond its aesthetic and functional goals, rhinoplasty profoundly affects a patient’s psychological wellbeing and social confidence. Evaluating postoperative satisfaction therefore requires not only anatomical assessment but also psychological insight into how patients perceive their evolving appearance.
In this context, our study examined whether the timing of first exposure to postoperative results influences patient satisfaction. Patients who first viewed their results two weeks postoperatively reported higher satisfaction after three months compared to patients who first viewed their results after one week. This finding highlights the importance of timing and expectation management in shaping patient satisfaction. Early visualisation—when swelling, bruising and asymmetry are still present—may create premature negative impressions, while delayed exposure allows early inflammation and oedema to subside, giving patients a more realistic sense of the surgical outcome.
From a psychological perspective, the observed effect of the timing of first exposure to postoperative rhinoplasty can be linked to cognitive biases such as the negativity bias, where individuals tend to give more weight to negative experiences (eg, initial swelling) than positive ones, influencing early self-perception. Additionally, the confirmation bias may lead patients to interpret early imperfections as confirmation of unmet expectations, lowering initial satisfaction. Delayed viewing at two weeks, when most swelling has resolved, aligns with a more balanced self-assessment, reducing these biases and enhancing long-term ROE scores.
The observed variance in outcomes between groups likely reflects differences in postoperative oedema, individual healing rates and patient expectations. Early exposure may amplify minor imperfections perceived as major flaws due to psychological sensitivity in the immediate postoperative period. Additionally, individual variations in tissue reaction, skin thickness and bruising intensity contribute to short-term dissatisfaction, but have little correlation with the long-term outcome. Seeing the result at one week—when oedema and ecchymosis peak—can negatively influence perception and self-esteem, even if the final aesthetic result is excellent. The transient swelling, residual bruising and minor asymmetries at that stage may bias patient opinion, leading to lower ROE scores later. By contrast, viewing the result after two weeks allows most swelling to resolve, leading to a more favourable and realistic self-assessment.
The ROE is composed of six questions that cover three domains related to quality of life: physical, emotional and social. This questionnaire has been widely used throughout the years. Despite the heterogeneity associated with different rhinoplasty approaches, the ROE can be considered a useful evaluation tool for rhinoplasty.9 Various studies have evaluated patient satisfaction using the ROE.
Gökçe Kütük and colleagues assessed 90 patients in the first, third and sixth months after rhinoplasty. They found that ROE scores significantly rose with the passage of time from the first to third and sixth months.10
Sena Esteves and colleagues evaluated 107 patients and followed them for three and six months. They showed that the ROE score did not significantly differ between three and six month follow-ups.4
Balikci and colleagues evaluated 62 patients using the ROE and divided them into two equal groups; one was followed up for less than six months and the other for more than six months. The results revealed that the satisfaction scores were nearly the same in both groups.11
In a study conducted by Bilgin and colleagues, 60 patients who underwent rhinoplasty were evaluated by ROE. It was revealed that males and older individuals (aged over 30) had a higher level of satisfaction.12 Arima and colleagues also showed that older patients have overall higher satisfaction.13 However, the effect of gender on satisfaction is still controversial. Some studies have indicated that women experience higher satisfaction after rhinoplasty,14,15 while others have shown that there is no significant difference between genders.16
Although none of these articles evaluated the effect of the timing of initially viewing the rhinoplasty results, they demonstrated that age and gender may also play a role in subsequent satisfaction. These can all provide guidance for surgeons to better satisfy patients who undergo rhinoplasty.
The senior author has adjusted his clinical practice based on these findings. He now routinely recommends that patients avoid visual self-assessment during the first 14 days postoperatively. Instead of early mirror viewing, patients are reassured that postoperative swelling and bruising will distort results temporarily. This approach has reduced early dissatisfaction and unnecessary anxiety among patients.
Based on these observations, we propose the following patient recommendation protocol:
-
Avoid patient mirror viewing and photography for at least 10–14 days after surgery.
-
Provide structured preoperative counselling explaining the normal recovery process.
-
Encourage patients to involve supportive family or friends in preoperative counselling to reinforce realistic expectations.
-
At two weeks, allow supervised first viewing with a clinician who can explain transient irregularities.
-
Schedule structured satisfaction assessments (eg, ROE questionnaire) at three and six months postoperatively.
This study has several limitations that should be considered when interpreting the results. First, the sample size was relatively small (n = 60), with 30 patients per group, which may limit the statistical power to detect subtler differences of subgroup effects, such as variations by gender or age, despite the observed significance in overall ROE scores. Additionally, the study population was homogenous, consisting primarily of young adults aged 20–39 years and predominantly females, all recruited from a single centre in Iran; this restricts generalisability to broader demographics, older patients or diverse cultural contexts where perceptions of rhinoplasty outcomes might differ. The follow-up period was limited to three months post-surgery, which may not capture long-term changes in satisfaction, as prior research using the ROE questionnaire has shown that scores can continue to improve or stabilise beyond the three-month time frame.
Conclusion
Ultimately, this study emphasises that patient satisfaction after rhinoplasty depends not only on surgical skill but also on timing, communication and psychological management. By delaying early visualisation, improving preoperative counselling and involving family support, surgeons can enhance postoperative satisfaction and reduce negative self-perception during recovery.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.
Revised: December 7, 2024 AEST; March 24, 2025 AEST