
Introduction
Breast augmentation-mastopexy in patients who have undergone substantial weight loss can be complicated by skin laxity and ptotic, deflated breasts due to loss of volume and ligamentous support, often causing unreliable results.1,2 The weight of the implants may result in bottoming-out deformities leading to inferior displacement of the implant.3 Additionally, the presence of excess soft tissue can result in a waterfall deformity, whereby the breast parenchyma slides over the implant and induces a ptotic appearance.4 Presently, there is a paucity of literature regarding the use of synthetic tissue reinforcements in patients undergoing breast augmentation-mastopexy. Recent systematic reviews5,6 suggest the existing body of evidence favours the promising safety profile of titanium-coated polypropylene mesh (Tiloop Bra Pocket, PFM Medical, Germany). There is an even greater scarcity of research regarding breast augmentation-mastopexy in massive weight loss patients.
We present a novel surgical technique which aims to address some of the challenges in this subset of patients, particularly as obesity rates rise and subsequent demand for bariatric surgery and weight loss medications increase.7,8
Operative technique
Sequencing
Surgery of this nature is often characterised by larger procedures with multiple elements. If there is a circumferential abdominal procedure planned at the same time, this is performed first before turning the patient to complete the anterior operations (such as the breast). Deciding which anterior procedure is performed first depends on the position of the breast footprint. If the preoperative breast footprint is high (needing to be lowered), the abdominal procedure is first completed as this will lower the inframammary fold (IMF) and often mean that there will need to be less of a lift. More commonly, the entirety of soft tissue on the anterior trunk and body has dropped following significant weight loss,9 a phenomenon sometimes described as a ‘melted candle’. It is frequently better to perform the augmentation-mastopexy first so that the IMF and soft tissue are not excessively lowered as a result of the abdominal procedure.
Approach
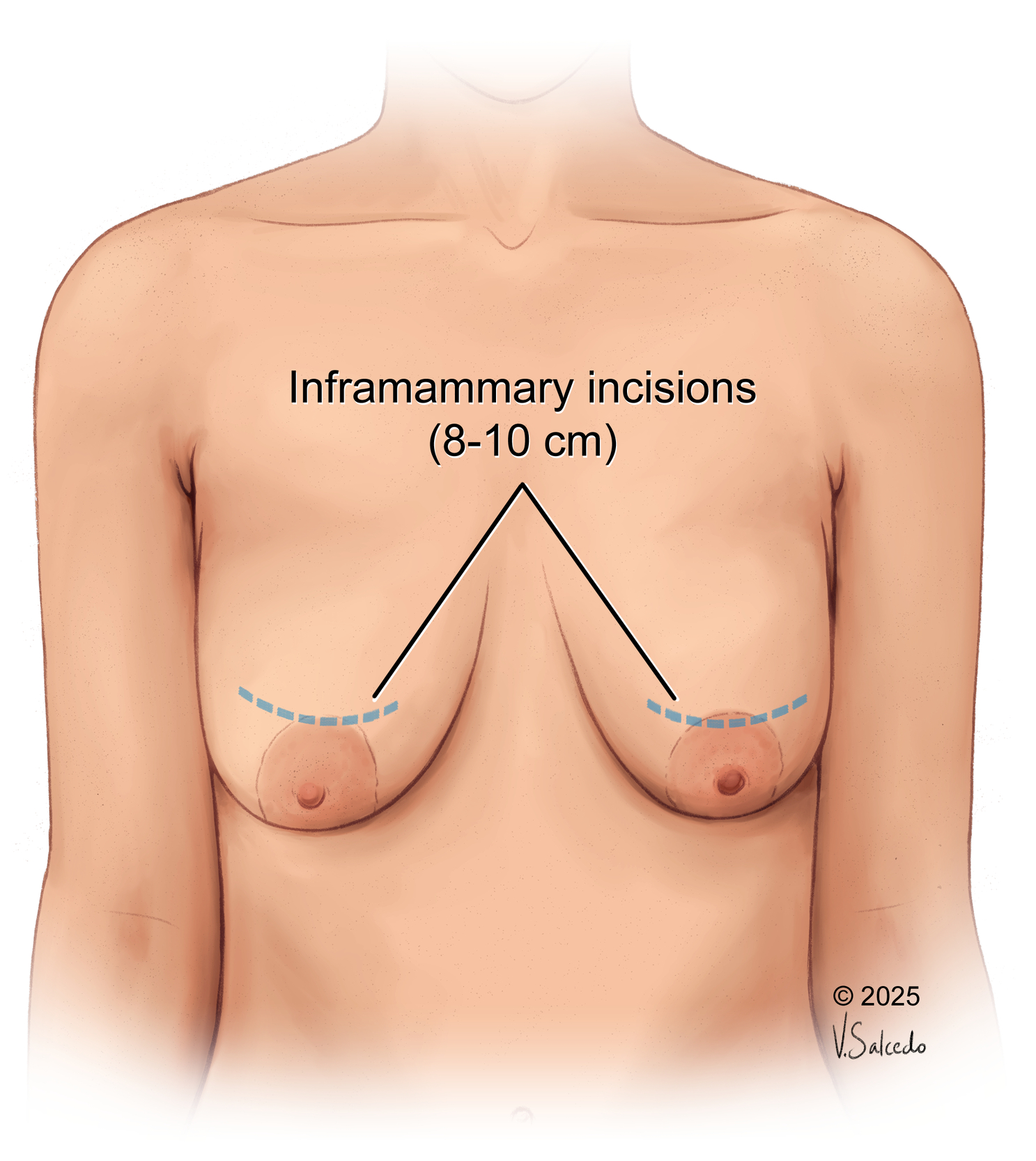
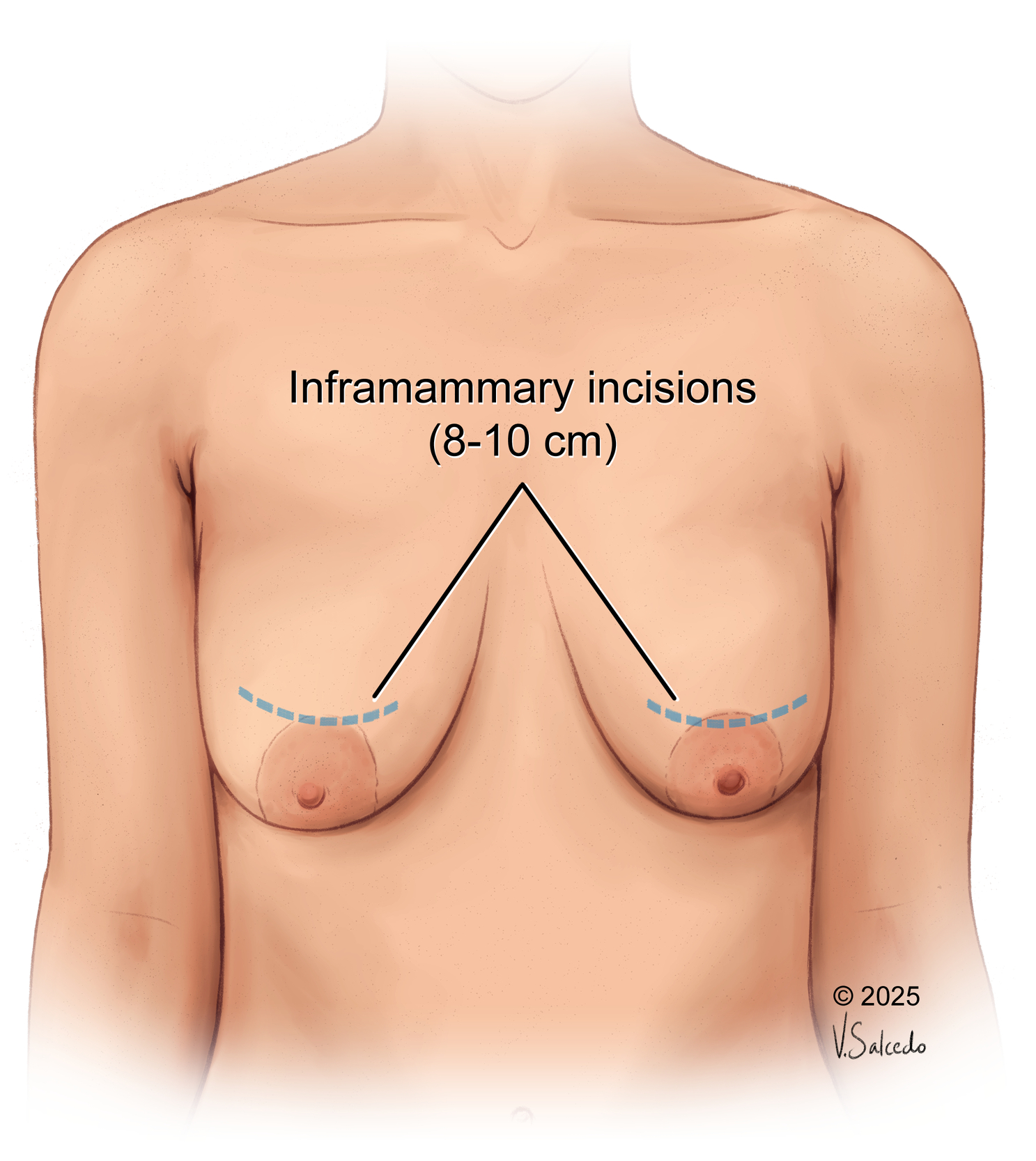
All surgical procedures are performed under general anaesthesia. The augmentation is performed through a standard inframammary incision (8–10 cm) centrally located in the IMF (Figure 1) or a dual plane approach (I or II) when appropriate. This incision is twice as large as a standard breast augmentation incision as it facilitates an easier and more accurate insertion of the implant/mesh pocket construct with less skin contact. An implant sizer is routinely used to assess the adequacy of the pocket before deciding upon the definitive implant. The pocket is prepared with standard antibiotic solutions (cephazolin 2 g and 160 mg gentamicin made to 40 ml and split between both sides), betadine and tranexamic acid, and thoroughly assessed for haemostasis before the implant and mesh pocket are placed. There is a learning curve regarding the insertion technique, and it has evolved over time to ensure that there is minimal handling/exposure and accurate placement of the implant/pocket construct. The learning curve is not overly steep; however, the major pitfall is inaccurate placement of the mesh construct. If this happens it is possible to adjust this pocket as a secondary procedure without much difficulty.
The steep learning curve may be mitigated by avoiding inaccurate placement of the mesh construct and achieving symmetric mesh placement with the contralateral side, especially in cases where preoperative breast asymmetry in the massive weight loss patient is evident. If asymmetry occurs, it is possible to adjust this pocket as a secondary procedure without much difficulty. Contouring and suturing the mesh atraumatically in the presence of a definitive implant also takes practice, given the limited pliability of TiLoop in contrast to other acellular dermal matrices.
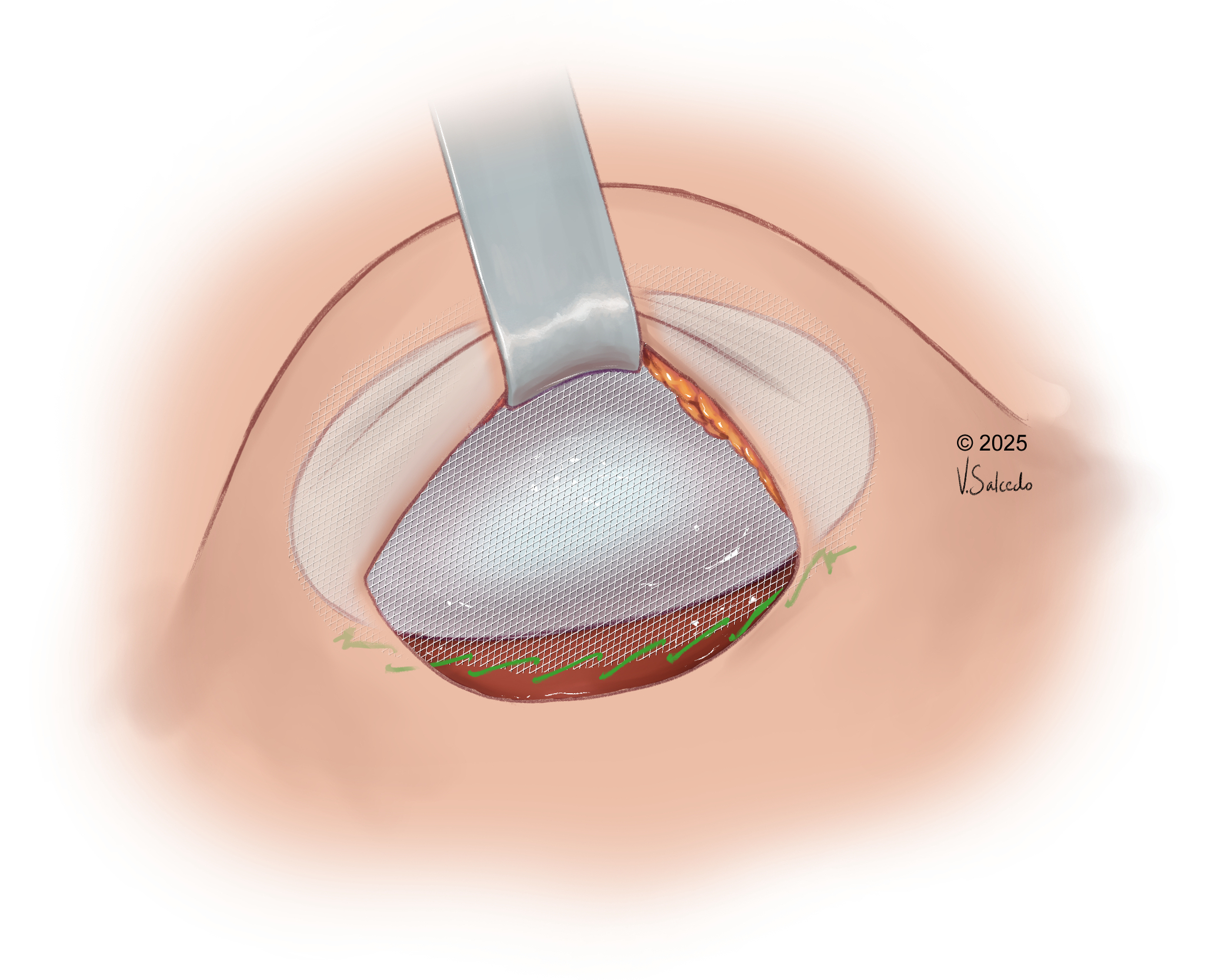
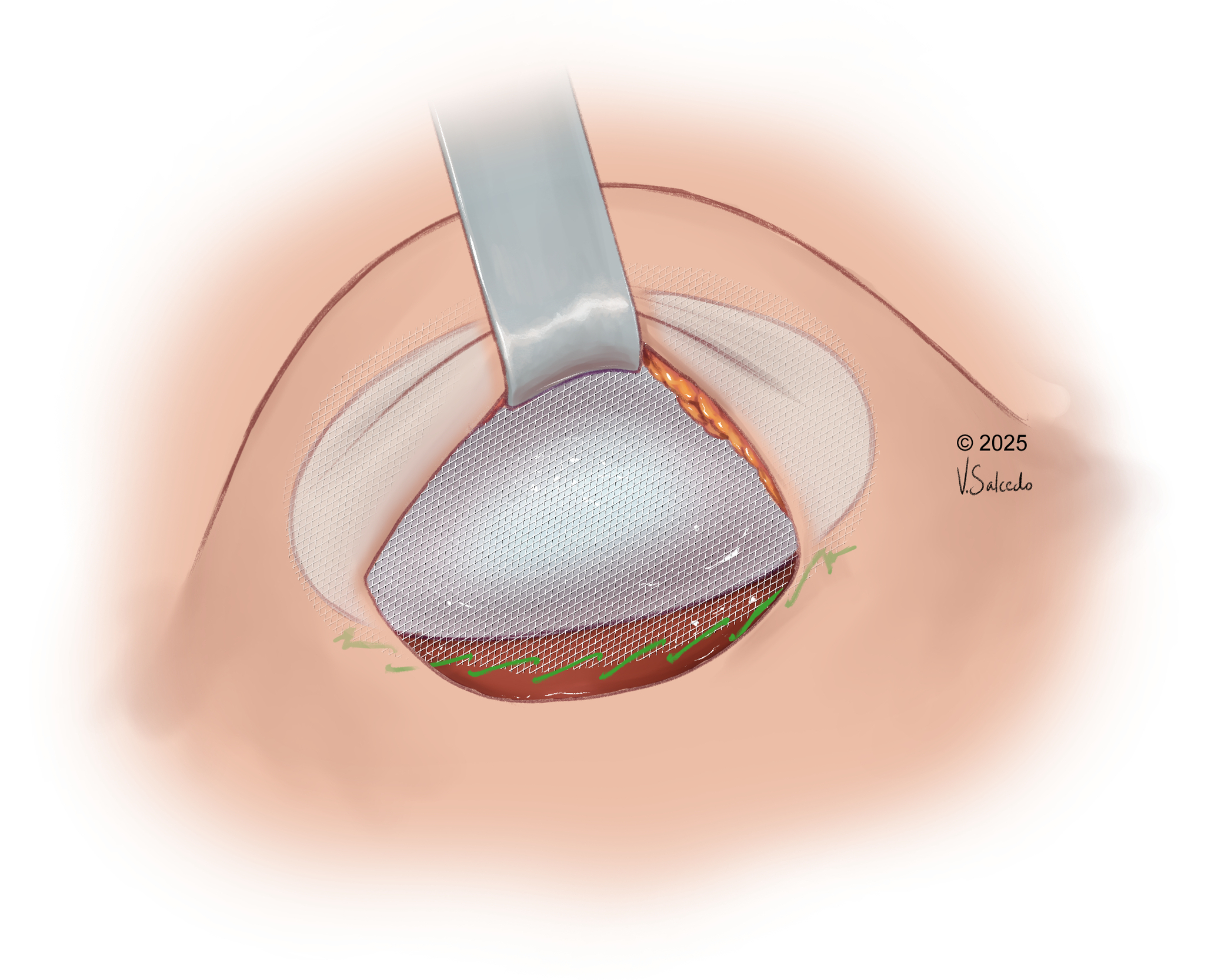
A pocket that is the tightest fit possible around the selected implant is chosen. As the pockets only come in three sizes (S/M/L), additional tailoring of the pocket around the implant is frequently required to ensure there is no movement of the implant within the pocket itself. The most common size used is the medium pocket, which easily supports volumes of up to 550 cc. An interrupted 2.0 PDS suture (Ethicon, Johnson & Johnson) is useful to tailor the mesh so that there is no movement within the pocket prior to insertion. The implant/pocket construct is then inserted at the same time rather than the mesh being inserted, followed by the implant (Figure 2). Subsequently, the mesh is secured in the lower pole using a running barbed suture (2.0 V-Loc 180, Medtronic), with caution to avoid damaging the implant before the pocket is closed in a standard layered approach. Once the implant is inserted, the head of the operating table is elevated so that the mastopexy can be performed. A superior pedicle is designed for the nipple with a 36 mm nipple-areolar complex. The pillars are then closed with 2.0 V-Lok 180 followed by interrupted 3.0 and 4.0 Monocryl (Ethicon, USA) sutures before skin closure is performed with 4.0 V-Lok 90. Any additional fat grafting is performed at this stage, usually in the cleavage area to soften the result as required. Finally, waterproof Prineo dressing (Ethicon, USA) is applied with a post-surgery bra for support.
Discussion
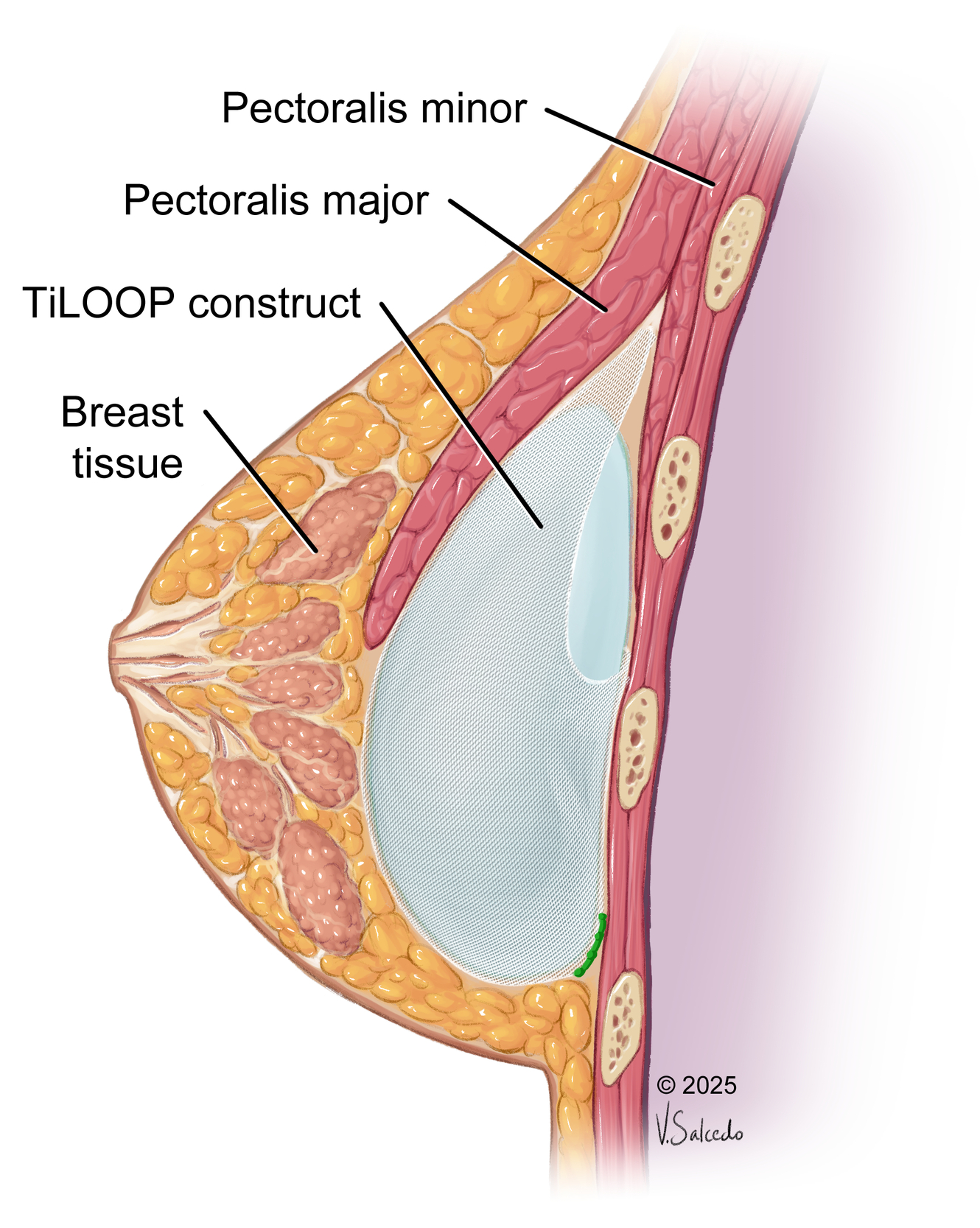
Breast augmentation-mastopexy in massive weight loss patients remains both surgically difficult and consistently understudied in the era of bariatric surgery and injectable weight loss treatment options.8 Regarding breast reshaping specifically, deflated and ptotic breasts are a common issue following substantial weight loss, often resulting in aesthetic impairments.10 Hence, particular considerations must be taken into account within the massive weight loss population. When dealing with significant amounts of excess soft tissue, removal of too much glandular tissue may result in necrosis and removal of inadequate tissue may result in persistent ptosis. We present an approach to breast augmentation-mastopexy in massive weight loss patients using a titanium-coated polypropylene mesh pocket to reshape ptotic and deflated breasts. This shares some similarities with the ‘empanada’ technique, in which an acellular dermal matrix or synthetic mesh covers the entirety of the implant.10,11 The construct is then used in a prepectoral approach in breast reconstruction. Our technique does not require suturing the circumference of the implant, only the lower pole, as the cranial aspect of the pocket sits tight between the pectoralis major and minor (Figure 3). There are no concerns regarding the barbed sutures being in contact with the implant because the sutures sit low in the sulcus between the anterior and posterior walls and are never in contact with the implant. The empanada technique also makes no reference to use of the GalaFLEX mesh (BD, USA) in the massive weight loss cohort, rendering its application to our patient cohort an area of future study.
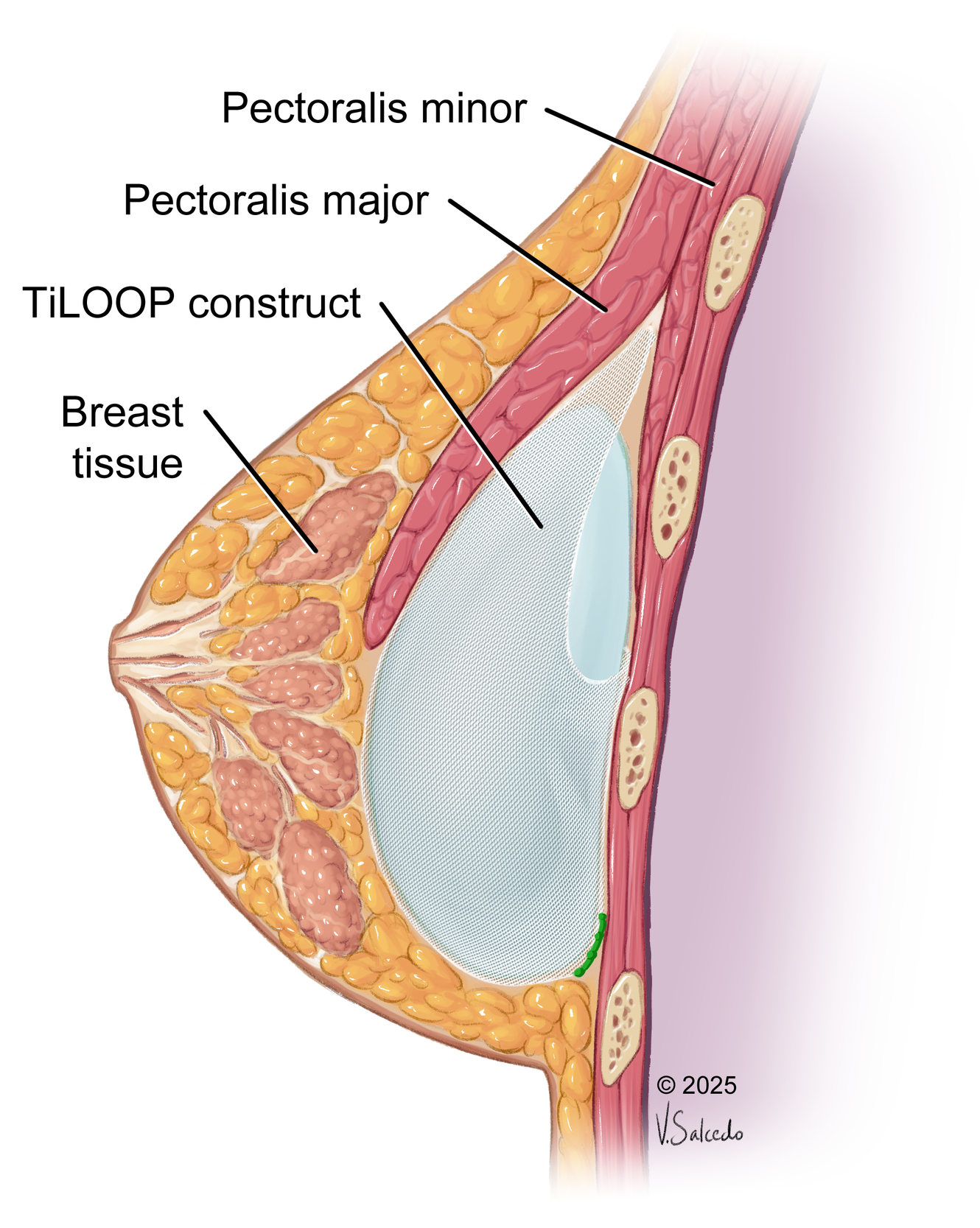
In the massive weight loss patient, the skin envelope at the upper breast pole can often be striated and thin. Placing sutures in the upper pole of this area could therefore become palpable and cause rippling of the mesh, which would appear unsightly. Suturing in the upper portion of the implant/mesh construct also carries a high risk of inadvertent implant rupture by attempting to suture in this tight space. Our illustrations demonstrate a tight upper pole that is achieved by virtue of securing the mesh posteriorly and inferiorly, which serves to mitigate the risk of implant migration.
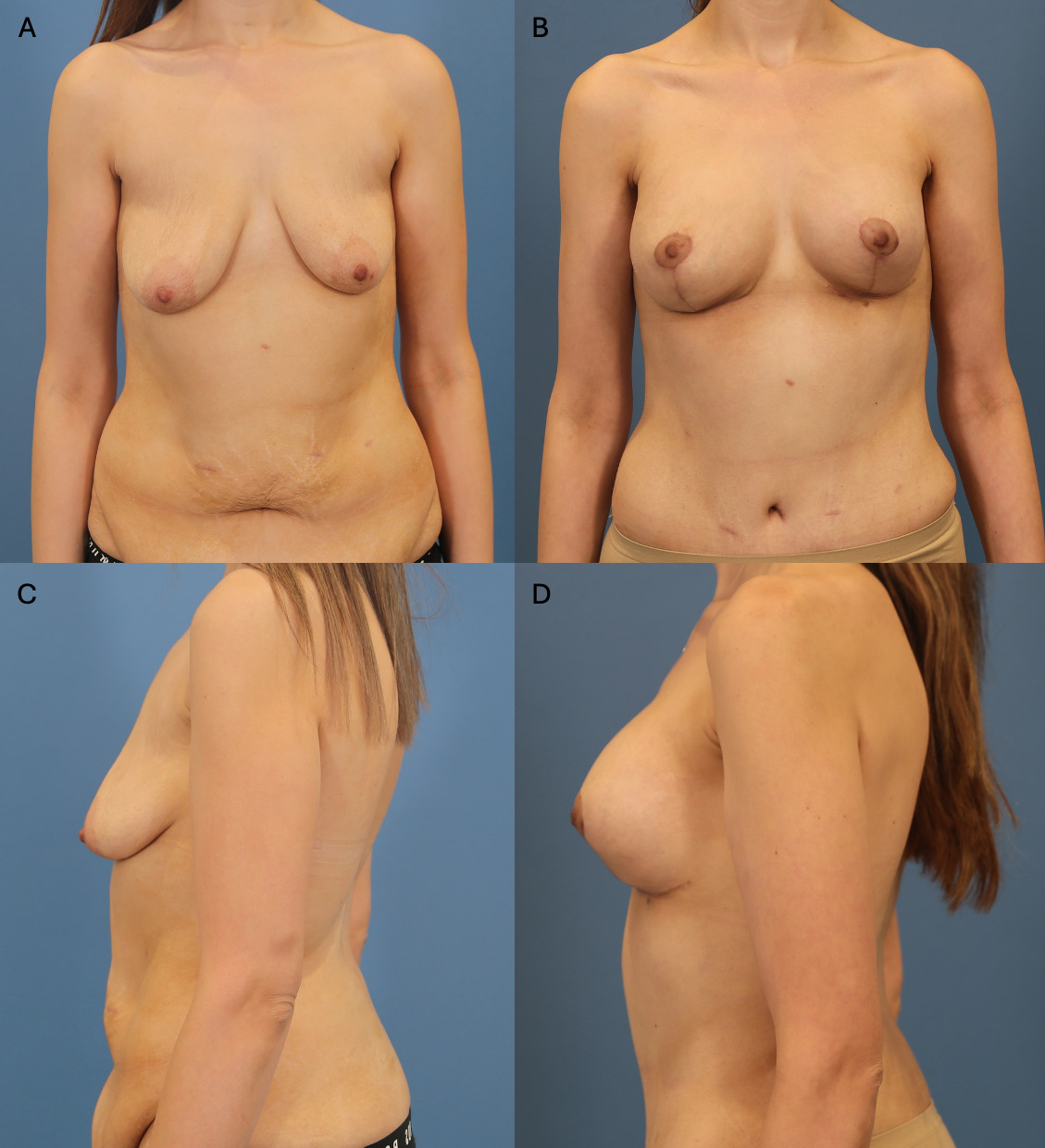
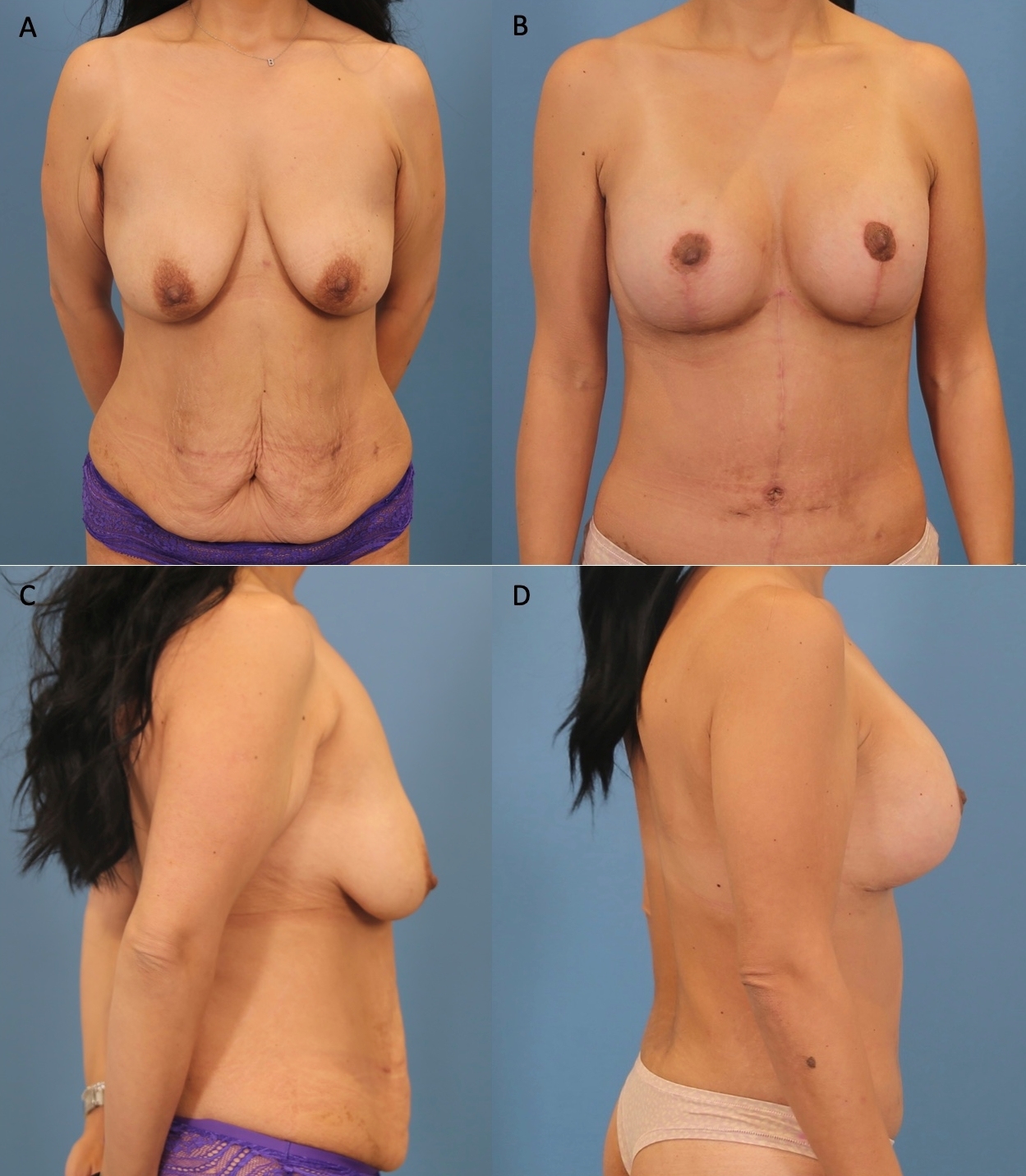
Thus far, this technique has produced favourable aesthetic outcomes, with significant improvements in breast volume and projection (Figures 4, 5 and 6). Though ptosis and pseudoptosis remained a challenge, the bra pocket mesh integrated well with the breast tissue and the implant position was highly stable. This technique has been used for 23 patients so far, of whom only one (4.4%) underwent pocket correction due to malposition (an earlier case before the pocket was customised around the implant). Otherwise, there were no instances of implant loss/malposition. In cases where revision surgery was required, patients subsequently achieved very satisfactory aesthetic results. Unfortunately, we have not assessed case cohorts without mesh use, hence a direct comparison cannot be made, however we can report a highly stable implant position in a challenging population subset with typically high rates of aesthetic complications. A single supply of mesh per patient can range between AU$1000 to AU$3000, well below the cost of revisional breast surgery, which would include anaesthetist fees, operating theatre costs and a potential overnight stay in a private hospital. Revisional surgery also incurs additional costs of ongoing dressings, wound care, review appointments and time off work for patients. Hence we can easily justify the additional cost of the mesh when presenting this as an option to patients. All patients presented with this option were willing to pay the additional fee with the intention of prolonging the longevity of their aesthetic result.



Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.
Revised: November 6, 2025 AEST