Introduction
Patients with symptomatic macromastia or gigantomastia are commonly treated with elective breast reduction surgery. In line with principles of patient autonomy, informed consent is undertaken preoperatively. The consent process is intended to disclose reasonable and material risks to the patient including discussing the possibility of complications.1 Postoperative nipple inversion (PONI) is a material risk to the patient as it changes the appearance of the breast and can affect breastfeeding and sexual function. In the 1970s, PONI was reported as a complication of breast reduction surgery but in recent years, it does not seem to be frequently mentioned. The risk of PONI following breast reduction surgery is currently not known for any described modern operative technique.
Nipple-areola complex (NAC) necrosis and sensation changes are frequently discussed, but nipple inversion and nipple projection are usually omitted from published results and complications. In some published studies, photographic evidence of PONI is evident despite not being mentioned as a complication in the body text of the publication.2
In light of our anecdotal experience of PONI in some patients and the omission of PONI in surgical literature, we performed a systematic literature search of PONI following breast reduction surgery, looking specifically for the rate of PONI for different breast reduction techniques. In addition to reviewing the rate of PONI reported in academic literature, this paper aims to quantify the rate of PONI in a single surgeon’s experience with the use of a superomedial pedicle, Wise pattern breast reduction technique.
Methods: systematic literature search
A systematic literature search was undertaken using the following search terms: nipple inversion, nipple retraction, nipple correction, nipple projection, nipple eversion, nipple complications, breast reduction, mammaplasty, mammoplasty, mastopexy and breast surgery. These terms were used to search the following databases: Cochrane, MEDLINE, Embase, PubMed and Google Scholar (see Supplementary material 1). A single reviewer (author BS) reviewed all abstracts for inclusion or exclusion.
The inclusion criteria were English language publications that mentioned nipple inversion as a complication of breast reduction surgery. Papers that examined nipple inversion and its correction unrelated to breast reduction surgery were excluded. Risk of bias assessment was not performed, as none of the included studies were targeted studies investigating PONI.
For included studies, all data was collected and tabulated by author BS. Quantitative data extracted were skin reduction pattern, type of pedicle, number of cases, and number of cases of PONI. Where it was not clear which pedicle was used, the cases were classified as having a ‘mixed’ pedicle. Qualitative data extracted were for explanations and theories regarding the reason for PONI. Fisher exact test was used to assess pooled data for numbers of each pedicle type and for PONI incidence.
Results: systematic literature search
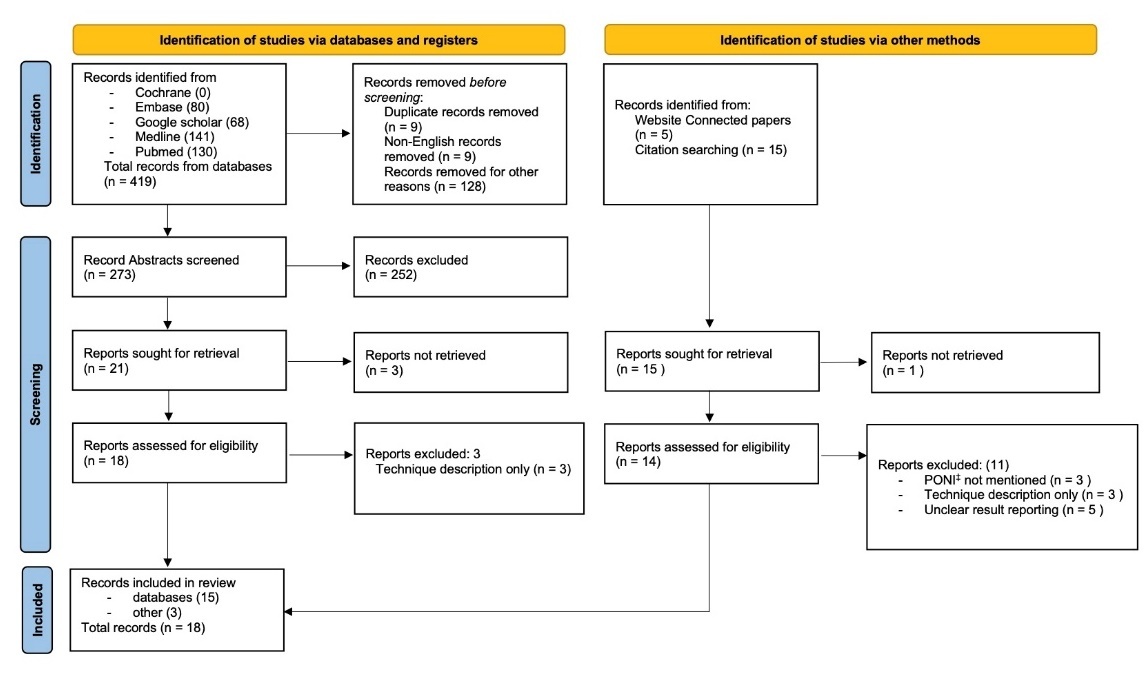
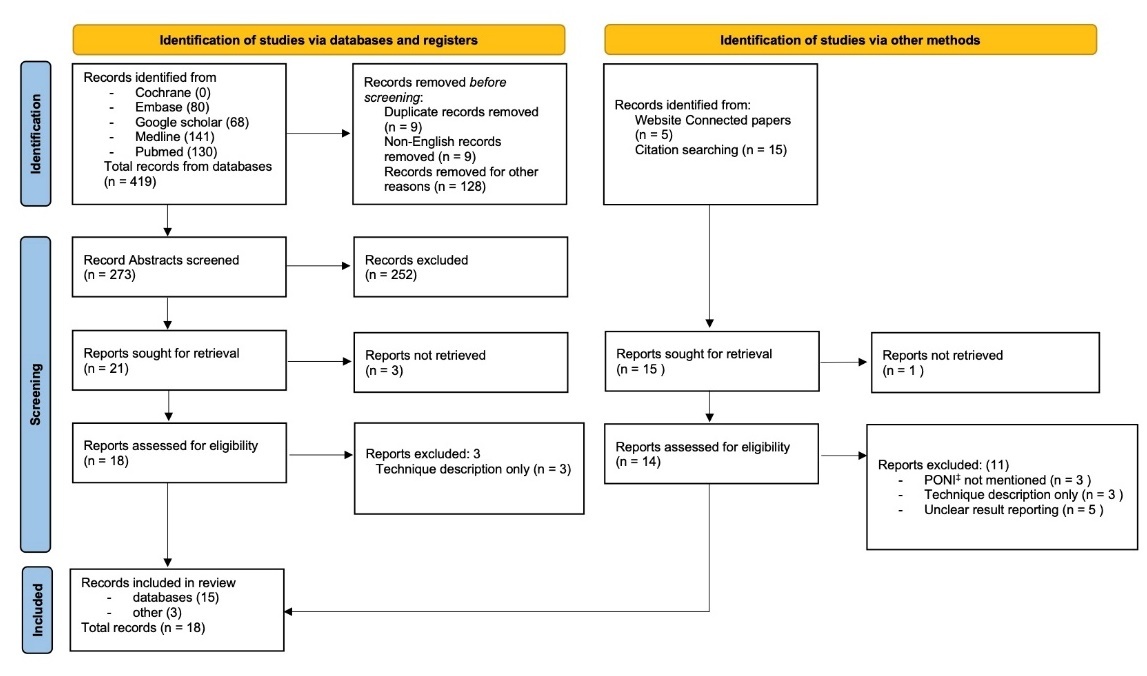
Eighteen studies were included in the final review3–20 (see Figure 1). There were no prospective studies or controlled trials. Sixteen studies3–8,11–14,16–20 were retrospective audits or case series of breast reduction operations. One study was a case series of nipple inversion correction procedures that included two cases of PONI after breast reduction.21 One study was a controlled study of lactating women comparing a cohort of women who had previously received breast reduction and a cohort who had not previously had surgery.10 The operative cohort of this study was included in the analysis.
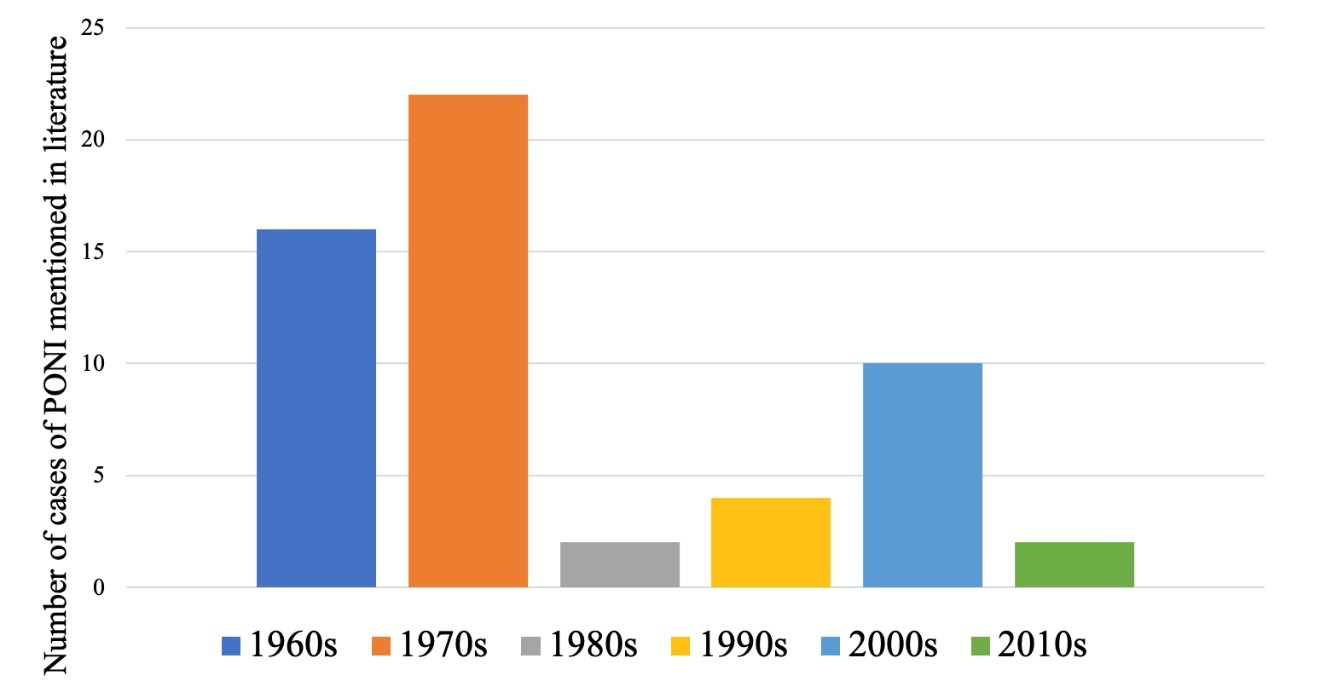
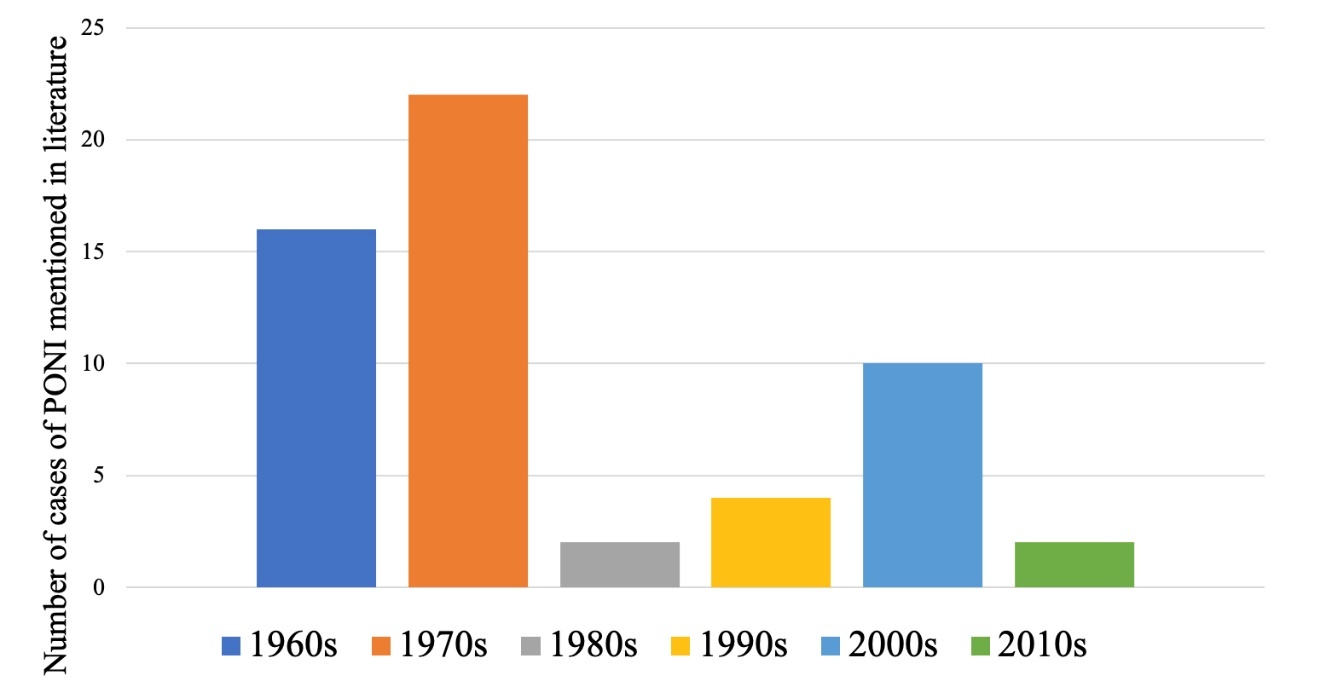
A total of 1453 patients across 18 retrospective studies were reviewed.3–20 There were 56 cases (3.85%) of PONI (see Table 1). The Strömbeck technique had a 17.0 per cent rate of PONI (p = 0.00001). The 1960s and 1970s accounted for 38 of the 56 (67.9%) of all PONI cases reported (see Figure 2).
Reasons discussed as the potential cause for PONI (see Table 2) were a short Strömbeck pedicle in small reductions,4,22 inadequate tissue bulk beneath the NAC,6,8,12,20,23,24 inferior pole ptosis applying inferior traction on the pedicle,5,23 and differential height of NAC skin and breast skin.17,20
Methods: retrospective audit
This retrospective audit was conducted with approval from the Ramsay Health Human Research Ethics Committee (approval number 2023/ETH/0039). The target population of this study was female patients who underwent surgery performed by the senior author from January 2021 until June 2022. Inclusion criteria were bilateral breast reduction for symptomatic macromastia with pedicled repositioning of the NAC. Exclusion criteria were patients who underwent symmetrising reduction in the context of breast cancer or breast reduction with free nipple graft. Of the 90 patients identified, 32 had incomplete documentation of preoperative or postoperative nipple inversion status and were excluded from the analysis.
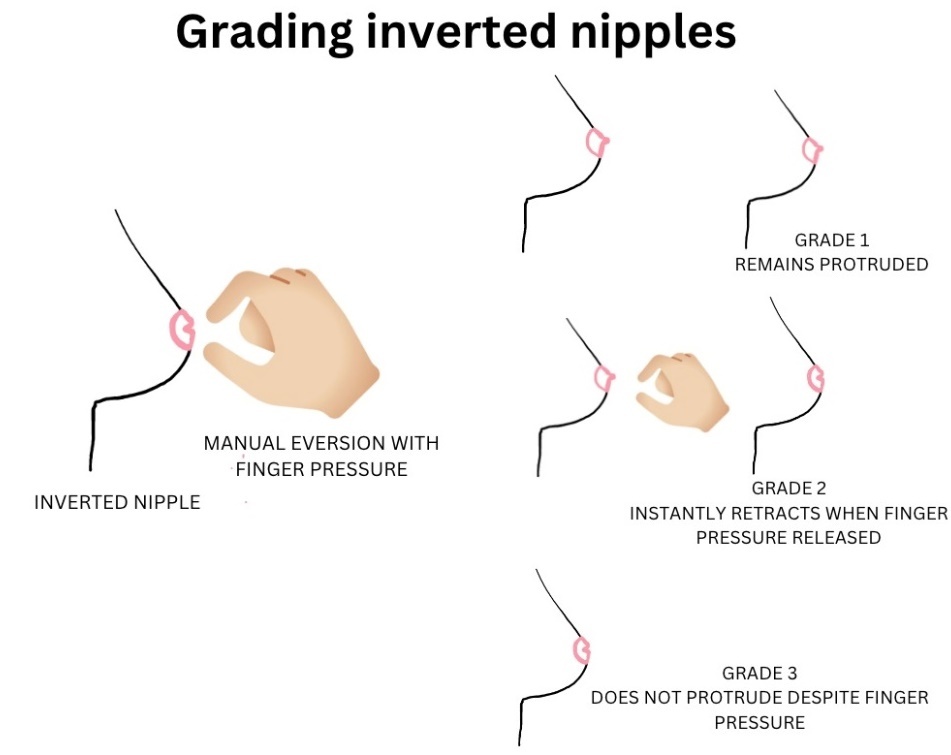
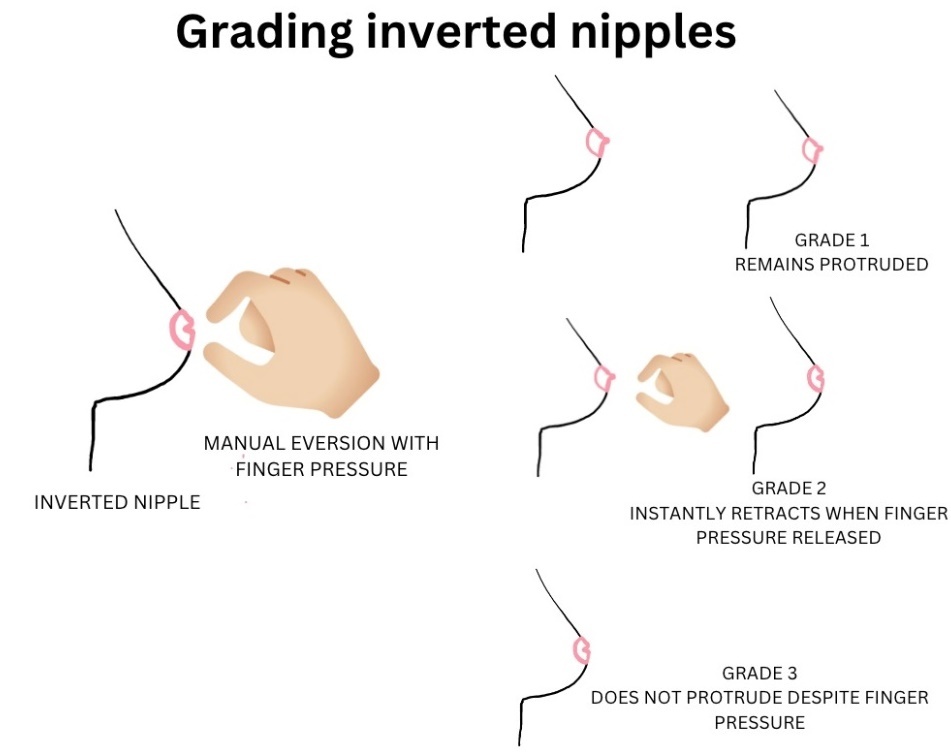
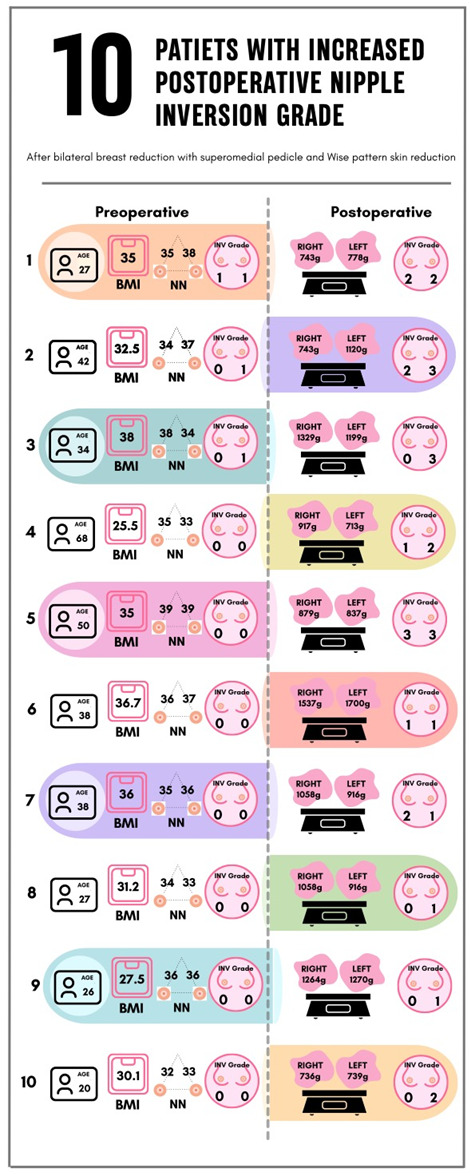
The primary outcome was the increased severity of postoperative nipple inversion compared to preoperative severity using the nipple inversion grading scale (see Figure 3) as defined by Han and Hong.25
Demographic and biometric data including age, body mass index (BMI), nipple to notch length (cm), tissue reduction weight (g) and preoperative nipple inversion grade was collected retrospectively from the patient record. Data regarding PONI was collected at 6–24 months postoperatively.
Data analysis was performed using RStudio (Posit Software, PBC 2025). Pearson correlation coefficient was used for continuous normally distributed variables. Fisher exact test was used for categorical variables. P-values less than 0.05 were considered to be statistically significant.
Results: retrospective audit
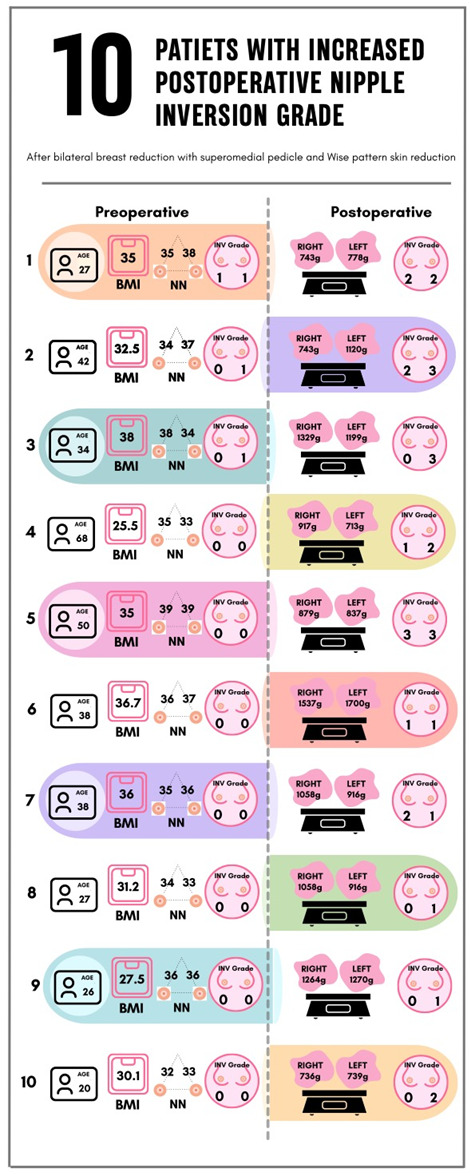
Fifty-eight female patients (116 breasts) with a median age of 39.2 underwent bilateral breast reductions with a median reduction weight of 602 g. A superomedial pedicle was used in 56 cases with a Wise pattern skin reduction. Two cases with reductions less than 500 g had vertical skin pattern reductions with a medial pedicle (see Table 3). Eight patients (13.8%) had preoperative nipple inversion. Ten patients (17.2%), including 16 breasts (13.8%), had an increase in the severity of their preoperative nipple inversion grade (see Figure 4). Per breast analysis revealed that preoperative nipple to notch measurement (p = 0.0001) and preoperative presence of grade 1 nipple inversion (p = 0.05) were associated with an increased risk of a postoperative increase in nipple inversion grade. Three of the eight patients (four breasts) with preoperative nipple inversion experienced an increase in postoperative inversion grade severity (see Figure 4).
Discussion
This study reports on the rate of PONI following breast reduction surgery in surgical literature (3.9%) and presents an audit of 58 of the senior author’s breast reduction cases. Cases of PONI were published and discussed widely in the late 1960s3,5,22 and 1970s,4–6,23 largely caused by the Strömbeck22 technique. Rates of PONI reached 30 per cent in some studies of that technique.3
After 1979, the presentation in publications of PONI as a complication of breast reduction effectively ceased until its tangential mention in 199110 by Terrill and colleagues in a paper discussing incising the mammary ducts in the treatment of inverted nipple. Scattered cases appear in the 2000s13–20 with no clear pedicle or technique emerging as the culprit. It would seem, based on the dearth of literature regarding PONI since the 1970s, that it is no longer a common clinical entity. However, our systematic search of the literature reveals ‘chatter’ about PONI as it is incidentally mentioned in some papers over the subsequent decades. In 1987, Hoffman reported that 4 per cent of medical legal lawsuits following breast reduction were brought due to PONI.9 In 2008, Abdel-Khalek and colleagues reported a 2 per cent PONI rate following 34 cases of superomedial pedicle vertical pattern reduction.17 In 2016, Henderson and colleagues presented a modification of the superomedial pedicle, Wise pattern reduction technique, which is specifically designed to prevent PONI.20 It is strongly suspected by the authors that the incidence of PONI following breast reduction surgery is under-reported and/or PONI is under-recognised.
Speculations for the cause of PONI were discussed in nine out of the 18 papers included in the systematic literature search.4–6,8,12,20,22–24 Strömbeck mentioned that breast reduction in small breasts yielded downward pull on the areola,22 and Melmed speculated that, when using the Strömbeck technique, short pedicles cause inversion.4 This is presumably due to the fact that the nipple is tethered on short medial and lateral pedicles as it is advanced superiorly under tension. Müller, who used the Strömbeck technique, claimed that PONI occurred months after surgery for his patients and he suspected the culprit to be ptosis of the gland within the skin enveloped over time.5
Regarding superior and superomedial pedicles, six publications discuss insufficient tissue bulk below the NAC as the cause for PONI.6,8,12,20,23,24
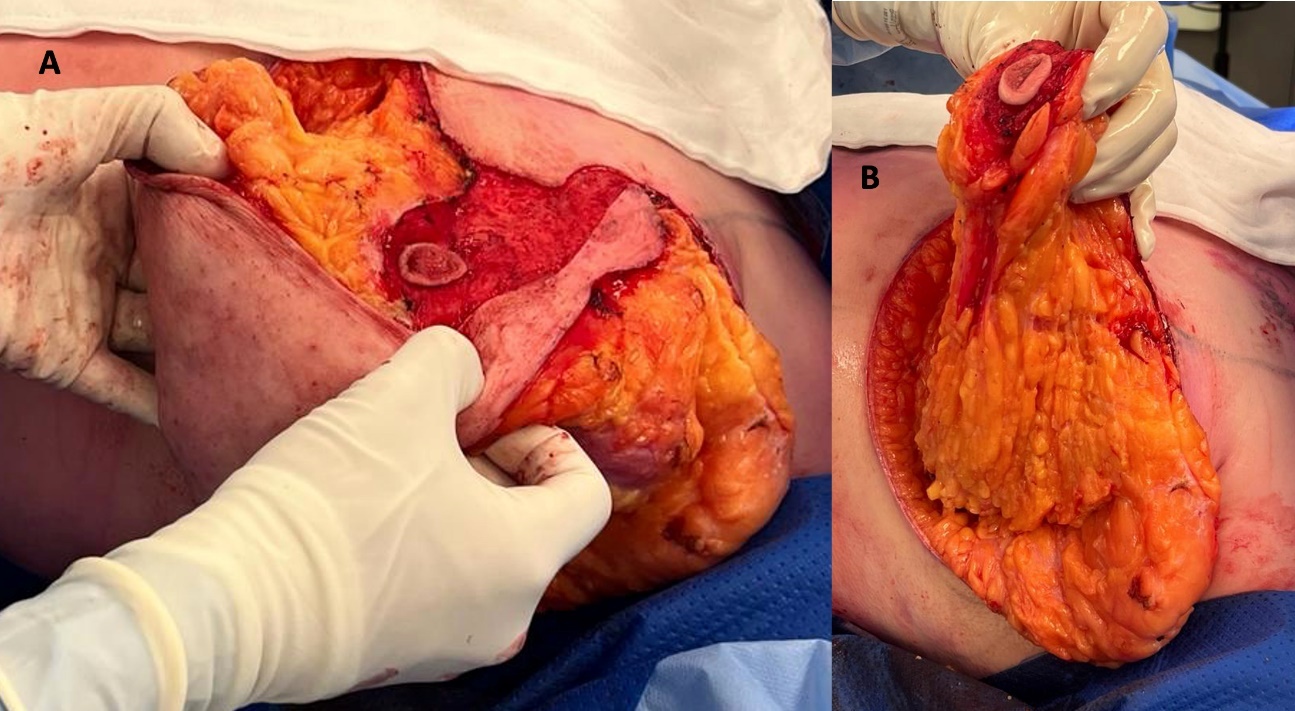
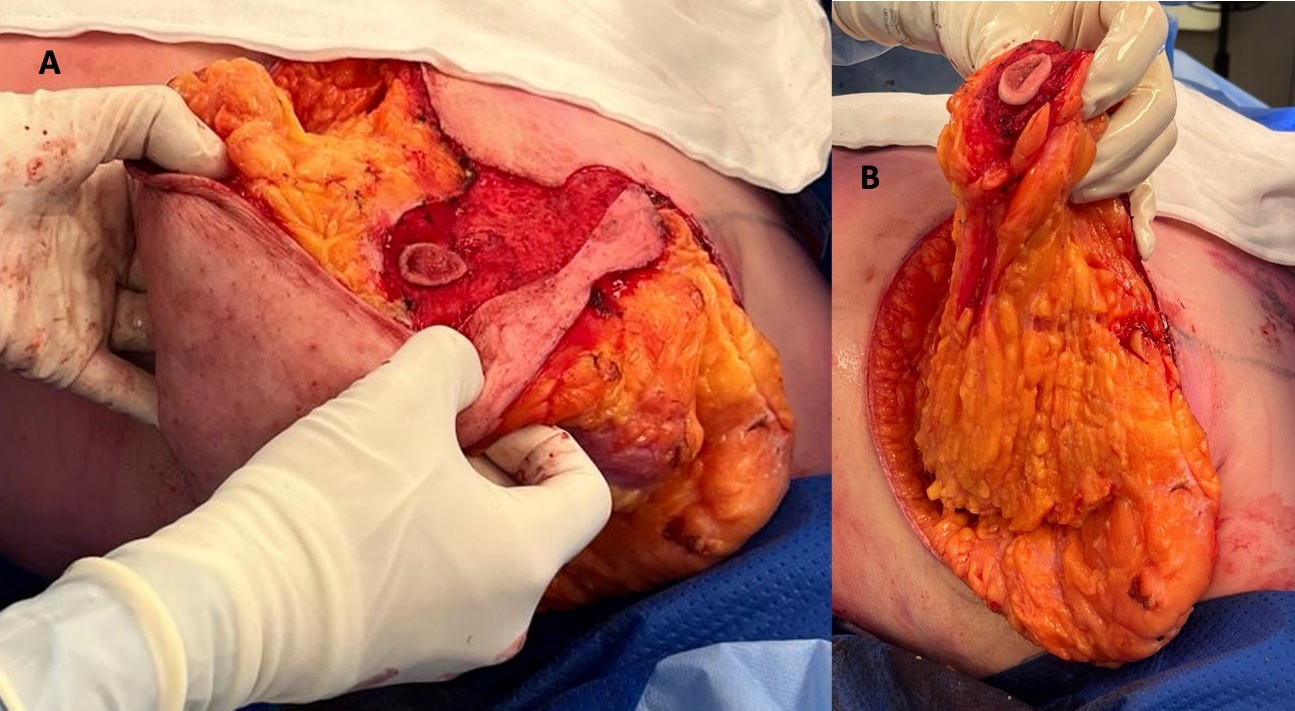
The authors of this paper, in addition to the above, speculate that during rotation of the superomedial pedicle to reposition the NAC, some of the inferior lactiferous ducts, which are connected to lobules within the pedicle, are stretched as the nipple is elevated in a superior direction. These ducts reach the limit of their stretch and pull the nipple inward. It is clear that this is not the only factor as it appears that some nipples invert intraoperatively at the time when the dermis of the pedicle is incised, before the repositioning of the nipple (see Figure 5). This phenomenon suggests that NAC smooth muscle and/or autonomic function may play a part. Clearly, there is a mechanical-anatomical reason for the change. The authors acknowledge that three patients (four breasts) who had preoperative nipple inversion experienced a decrease in their nipple inversion grade. This may be due to particularly short lactiferous ducts within a ptotic gland causing inversion that is corrected following reduction of the gland and repositioning of the nipple superiorly.
Strengths and weaknesses of this study
In our retrospective cohort of 58 patients, the rate of PONI was 17.2 per cent, which is a rate that warrants discussion in the preoperative setting. The results of this study are limited by small sample size and selection bias, as only a subset of eligible participants who underwent bilateral breast reduction had clear documentation of preoperative and postoperative nipple inversion status in their medical record. This study was devised following anecdotal experience by the senior author of an increased rate of PONI in patients with preoperative nipple inversion. As a result, retrospective review of eligible patients yielded a significant minority in whom preoperative nipple inversion status was not clearly documented. These patients most likely did not have preoperative nipple inversion and did not experience symptomatic PONI or they would have had closer follow up. Therefore, this study’s selection of patients likely represents a selection bias with a skew towards PONI. In future studies, this bias could be overcome by prospectively and contemporaneously collecting data on preoperative and postoperative nipple health from all patients as part of the clinical workflow.
A strength of this study is its homogeneity. All patients underwent operations by the senior author and 55 (95.8%) underwent superomedial pedicle, Wise pattern breast reductions. In this sense, the operative technique and method was consistent.
This under-researched complication leaves many unanswered questions, which could be addressed in further studies. The biomechanical and physiological causes of PONI have not been discussed in detail in past publications. This may in part be due to the relatively scarce literature describing the comprehensive anatomy of the nipple and areola. Many contemporary publications and resources focus on the vascular and cutaneous sensory supply of the NAC but few reference the NAC’s intradermal smooth muscle structure, its autonomic nerve supply or the relationship of this functional smooth muscle unit to the lactiferous ductal system.
Conclusion
Postoperative nipple inversion following breast reduction surgery may be an under-reported complication and may occur commonly enough to warrant specific discussion in a preoperative consultation. This paper is a call to surgeons to record and publish their outcomes regarding PONI to more accurately quantify its incidence.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.
Revised: August 19, 2025 AEST