Introduction
Breast augmentation and/or reconstruction is a major challenge in both aesthetic and reconstructive surgery. Autologous fat grafting (AFG) as an aesthetic and reconstructive tool has become increasingly popular, offering natural tissue restoration with relatively low morbidity. The techniques for AFG have evolved over time with no standard method widely used. In both aesthetic and reconstructive breast surgery, AFG is primarily used to alleviate tissue defects and contour abnormalities to help patients regain physical integrity and for psychological rehabilitation. Autologous fat grafting is generally considered a safe and minor procedure but complication rates can be up to 27 per cent with the most common being fat necrosis.1 Lipomas are one of the most common benign soft tissue tumours with unclear precise pathophysiology. In this report we present the first documented case of iatrogenic lipoma formation following AFG in the breast.
Case
A 69-year-old female patient with a history of multiple sclerosis presented for the third round of AFG to her bilateral breasts. She underwent an oncological bilateral mastectomy for breast cancer in her 20s with immediate implant reconstruction (round textured saline 360 cc). These implants were revised once and remained in situ for 20 years. In 2017 the patient underwent revision and implant replacement (microtextured 440 cc) due to implant rupture and capsular contracture. In 2018 these second implants were removed due to capsular contracture and not replaced. Due to recurrent implant issues, the patient began treatment with AFG to improve contour defects and completed two rounds in July 2022 and October 2022.
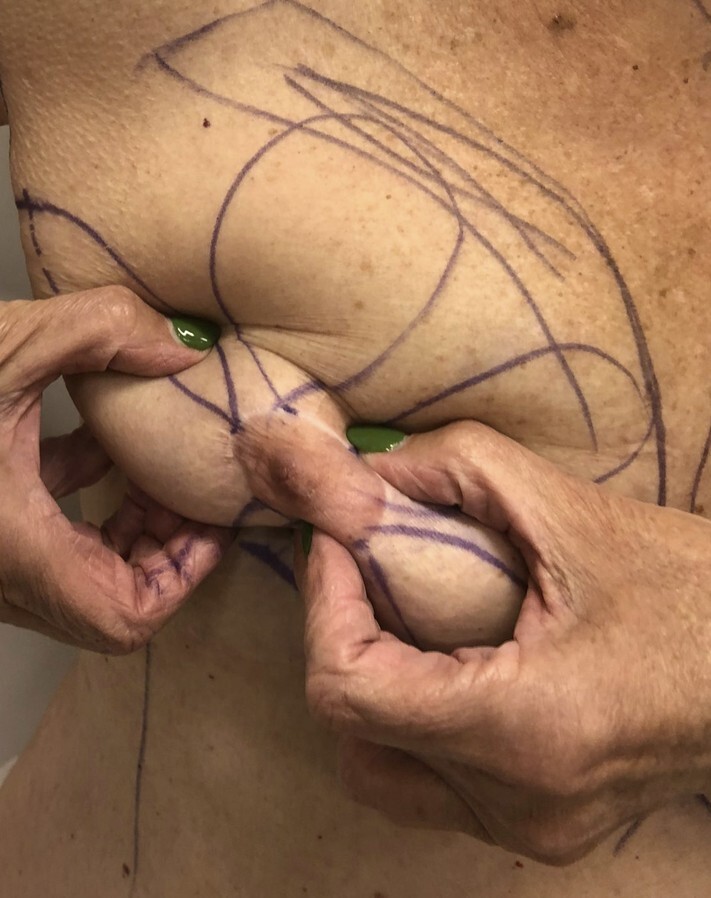
Prior to the third round of AFG, the patient had noticed two right-sided breast lumps present for months. Ultrasound imaging excluded a malignant process and suggested benign changes post fat grafting. On examination there were two distinct, well-defined rubbery lesions in the patient’s right breast that were extremely mobile and able to be moved around the entire breast mound with ease (Figure 1).

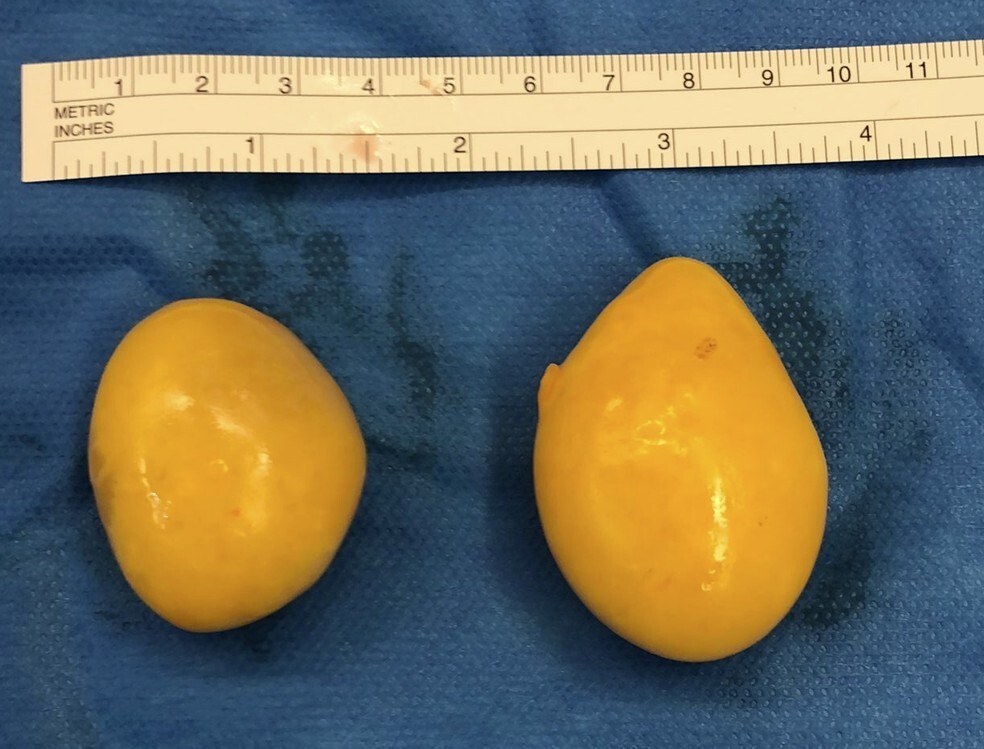
The patient underwent surgery to remove the lesions. Intraoperatively a vertical incision was made beneath the nipple areolar complex through the subcutaneous plane. Both lesions were expressed out of the incision without requiring dissection (see Figure 2 and Supplementary video). There was minimal seroma fluid and no distinct capsule or pocket containing the lesions. The lesions were distinct, yellow, rubbery masses measuring approximately 46 × 35 × 24 mm and 38 × 29 × 23 mm. The rest of the breast cavity and tissue was otherwise unremarkable.

Histopathology confirmed a diagnosis of benign lipoma with the lesions composed of lobules of mature adipose tissue, without atypical features, surrounded by a thin fibrous capsule. One specimen contained small areas of clear fluid suggestive of a previous seroma component. The patient recovered well postoperatively and no lipomatous lesions were present elsewhere on the body. At one-year postoperatively the patient had not developed any recurrent lesions and declined further AFG, opting to trial implant reconstruction once again.
Discussion
Autologous fat grafting is an increasingly popular procedure performed for both aesthetic and reconstructive purposes. It is usually described as a minor or minimal procedure with low risk. This study presents a case of iatrogenic lipoma formation secondary to AFG in the breast.
The exact pathophysiology of lipoma formation is unclear, though literature suggests roles for trauma, chronic irritation and adipocyte dysregulation.2 Iatrogenic lipoma formation has been reported in association with blunt trauma, with a hypothesis that trauma causes fat necrosis along with secondary inflammation stimulating lipoma formation.3 In this case, multiple fat grafting sessions combined with numerous implant-related complications may have promoted the formation of a lipoma. The presence of clear fluid in one lesion alludes to a possible relationship with chronic seroma formation potentially creating an environment to allow the adipocyte aggregation. These potential circumstances do align with literature hypotheses of trauma or surgery-induced lipogenesis.2
Conclusion
This case represents the first reported instance of iatrogenic lipoma formation following AFG for breast reconstruction. Although the precise mechanism remains unclear, multiple fat grafting and prior breast implant complications play a role in abnormal lipoma formation. Postoperative nodularity in the breast after AFG is typically attributed to fat necrosis and oil cysts. Recognition of lipomas as a rare outcome after AFG, as well as a differential for assessing new masses, may influence diagnostic workup, patient reassurance and management.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary online material
A video accompanying this case report can be found on the AJOPS YouTube channel: https://youtu.be/1WyewBAghmg. Please note that due to YouTube content restrictions, you may be required to sign in or create a login to access the video.