Introduction
Just 18 months ago, we published an excellent overview on the use of robots in plastic surgery by Coehlo and colleagues.1 Since then, however, the pace of change has been staggering. In just over two years artificial intelligence (AI) has exploded and humanoid robots are on the cusp of revolutionary expansion. Elon Musk recently declared medical school ‘pointless’ considering AI’s rapid advancements. Robotic systems and AI, once the stuff of science fiction, are now integral to modern surgery, with Musk predicting that humanoid robots like Tesla’s Optimus could outperform top surgeons within three years, rendering traditional training obsolete.2
Echoing this sentiment, tech investor Jason Calacanis, after witnessing the latest Optimus prototypes, proclaimed that ‘nobody will remember that Tesla ever made a car’,3 suggesting that the robot’s transformative potential could eclipse the company’s automotive origins. Last year Chinese surgeons remotely removed a liver tumour using a robot 2600 km away from Beijing over a cell phone network.4
From da Vinci robotic arms performing minimally invasive procedures to AI algorithms analysing imaging data in real time, these technologies promise precision, reduced complications and faster recovery times for patients. Yet, beneath this veneer of progress lies a stark reality: surgeons’ jobs could be increasingly at risk. As AI and robots handle more tasks autonomously, human surgeons face deskilling, over-reliance on AI and potential obsolescence.
How vulnerable are plastic surgeons compared to our other specialist colleagues and what, if anything, can we do to mitigate the risk and evolve our practices to embrace this rapid change?
Evolving role of AI
The integration of AI and robotics in surgery has accelerated dramatically. A 2025 study highlighted how AI-enabled robotic systems have reduced operative times by 25 per cent and intraoperative complications by 30 per cent in various procedures.5 In July 2025, AI systems even conducted the first autonomous gallbladder removal, trained on mere hours of video data.6 These advancements stem from AI’s ability to process vast datasets, predict outcomes and guide robotic tools with superhuman accuracy. For instance, AI can reconstruct 3D images rapidly and assess surgical performance in real time, outpacing human capabilities in consistency and speed.
However, this efficiency comes at a human cost. Over-reliance on AI risks eroding surgeons’ core skills—a phenomenon known as ‘deskilling’. A 2025 study in The Lancet Gastroenterology and Hepatology found that after just three months of using AI tools for colonoscopies, doctors were significantly worse at spotting precancerous growths without the technology.7 This mirrors broader concerns in healthcare: as AI automates diagnostics and basic tasks, surgeons may lose critical thinking and manual dexterity. Reuters reported in 2026 that AI-integrated surgical devices, like the TruDi Navigation System, have led to over 100 malfunctions and at least 10 patient injuries since 2021, often due to errors when AI misinformed surgeons about instrument locations.8 Such incidents not only highlight technical risks but also underscore how dependence on ‘black-box’ AI—where decision-making processes are opaque—can undermine surgeons’ autonomy and increase errors when systems fail.
Job displacement is another looming threat. A 2024 analysis suggested that while AI’s impact on healthcare jobs is lower than in other sectors, tasks like administering anaesthetics or routine exams could be automated, leading to unemployment in specialised roles.9 An HIMSS discussion on AI in healthcare warns of disruptions to workflows, with roles in medical coding and diagnostics at high risk of obsolescence.10 In a 2024 Pneumon article, experts predict that Super AI could eventually replace entire medical specialties, exacerbating global unemployment in healthcare.11 Surgeons, who invest years in training and accrue substantial debt, may find their expertise commoditised by machines that don’t tire, err less frequently or demand salaries. While AI augments rather than fully replaces in the short term—76% of physicians view it as complementary—the trajectory points toward fewer human surgeons needed for routine operations.9
Ethical and equity issues compound these risks. Biases in AI datasets can perpetuate healthcare disparities, as noted in a 2024 ScienceDirect article, where inadequate training data leads to misdiagnoses in under-represented groups.12 High costs limit AI-robotic systems to affluent hospitals, widening access gaps.13 As AI becomes part of critical decision-making, questions of accountability arise: who is liable for an AI-driven error—the surgeon, the developer or the algorithm?
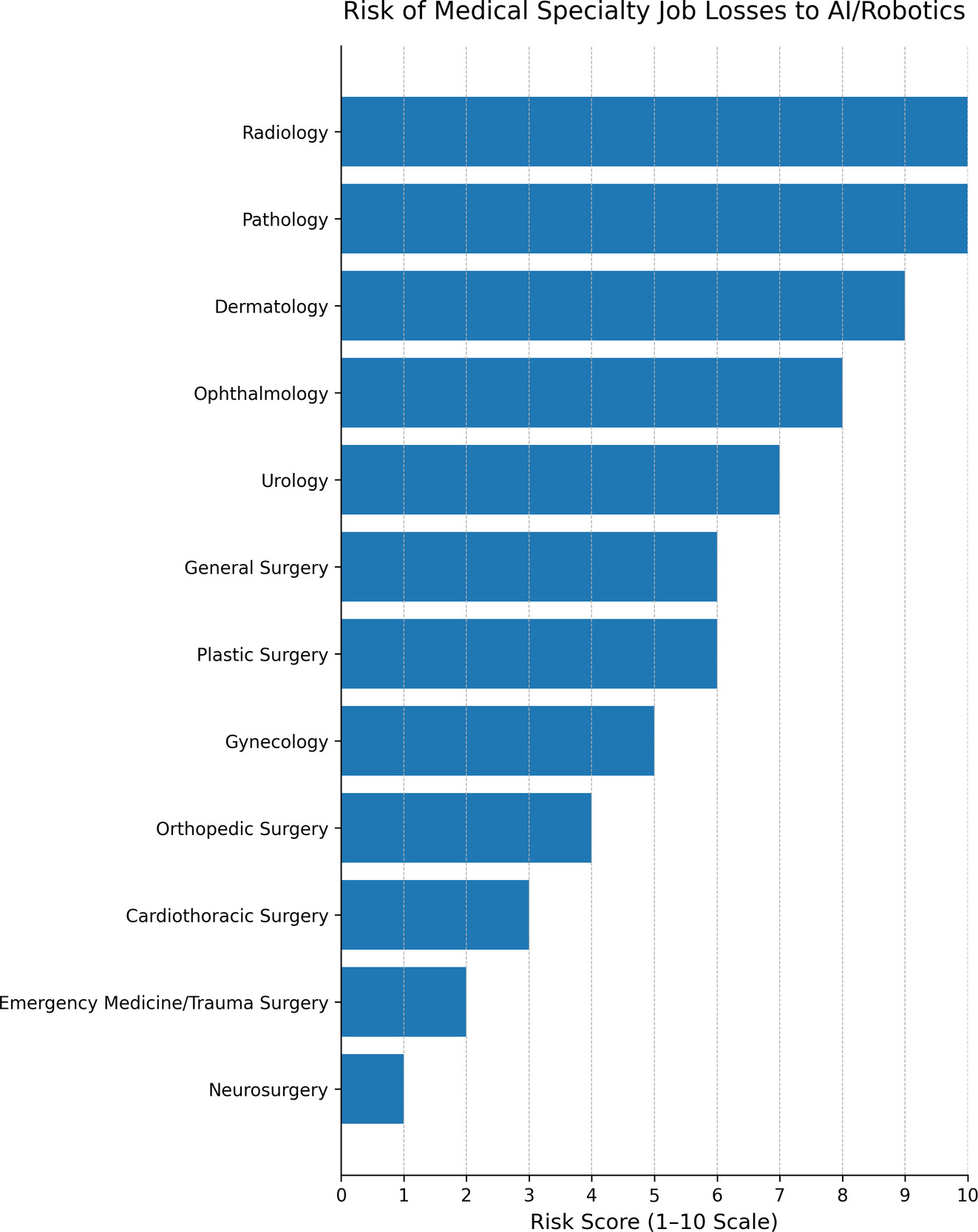
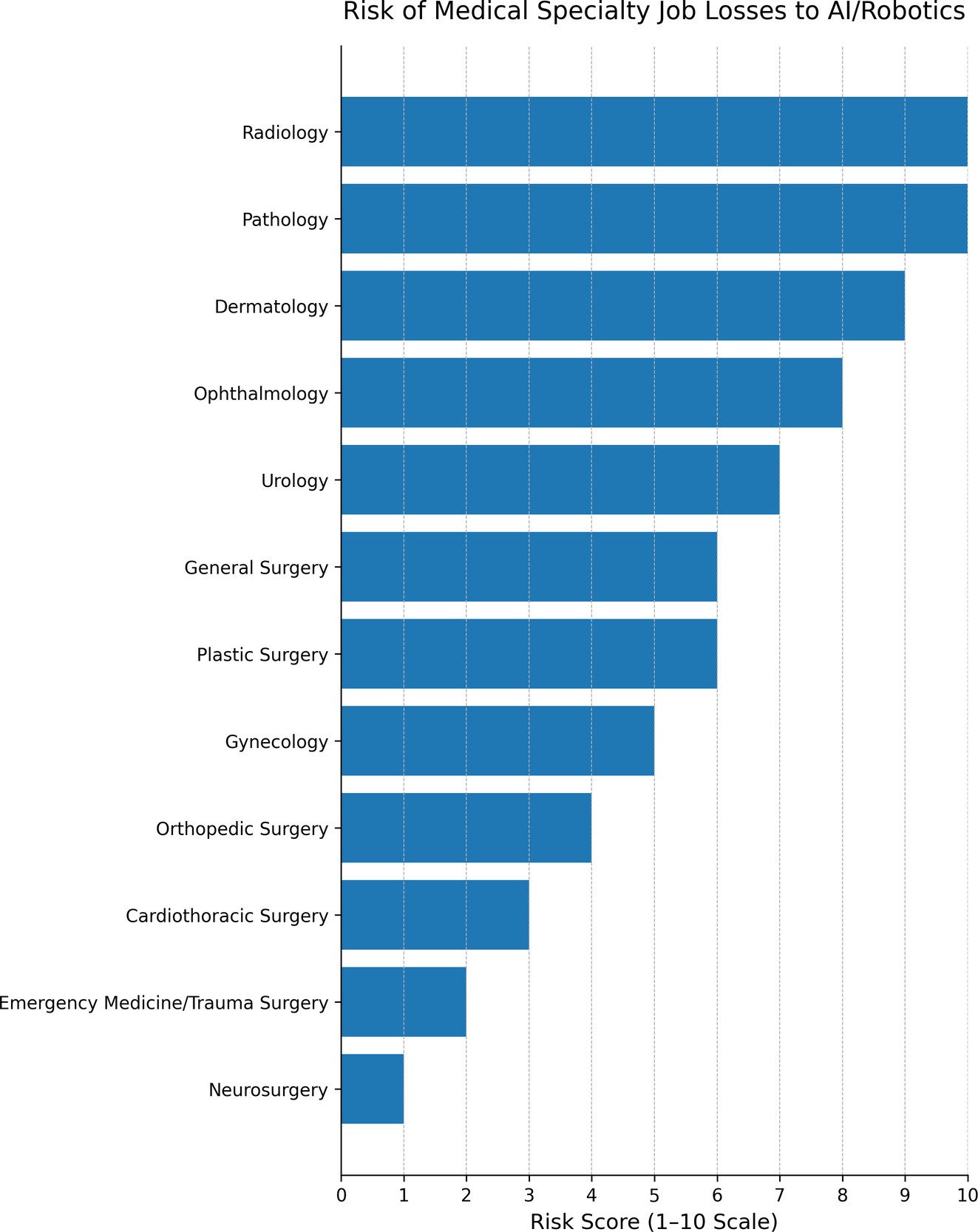
Below is an AI-generated table of at-risk specialties in medicine. It is interesting to see how AI rates the at-risk specialties (see Table 1 and Figure 1).
Zooming in: plastic surgeons on the cutting edge of disruption
While all surgeons grapple with these threats, plastic surgeons face amplified vulnerabilities due to their field’s aesthetic, reconstructive and elective nature. From preoperative planning to postoperative monitoring, AI and robotics are transforming plastic surgery, potentially sidelining human expertise in ways that could decimate job prospects.
Artificial intelligence excels in predicting surgical outcomes and simulating procedures, areas central to plastic surgery. A 2023 review noted AI’s potential to forecast results, optimise procedures and track recovery, reducing risks like infections or poor healing.14 Tools like AI-driven photo analysis simulate post-rhinoplasty appearances or map vessels for flap surgeries, often with greater precision than manual methods.15 Robotics, meanwhile, enhances microsurgery—key for reconstructions—by filtering tremors and enabling intricate tasks in confined spaces.16 A 2025 Genoa article described AI in plastic surgery for risk calculators and wound monitoring via wearables, potentially automating much of the decision chain.15
Yet these innovations heighten job risks. Plastic surgeons rely on artistic judgment and patient interaction, but AI could commoditise this. Ethical reviews in 2024 highlight biases in AI models, which may misjudge outcomes for diverse skin tones, leading to inequities and eroding trust.17 Overdependence on AI simulations risks deskilling, as surgeons defer to algorithms for planning, potentially losing intuitive skills.18 Cybersecurity threats are acute; a 2022 npj Digital Medicine study warned of vulnerabilities in robotic systems, where hacks could disrupt procedures.19 In elective fields like cosmetics, where patient satisfaction drives revenue, AI ‘hallucinations’—fabricated outputs—could lead to malpractice suits.20 A 2024 Australasian Journal of Plastic Surgery review noted that while robotics expands possibilities in head, neck, and breast reconstructions, high costs and retraining needs may displace less tech-savvy surgeons.1
Moreover, the field’s elective focus makes it susceptible to market shifts. As AI lowers barriers—enabling non-surgeons to use robotic tools for aesthetic treatments—traditional plastic surgeons could see demand drop.16 A 2025 Cureus systematic review found AI-robotics reducing errors in minimally invasive procedures, but at the expense of human roles.21 In a competitive specialty with limited residencies, AI could exacerbate unemployment, as fewer surgeons are needed for augmented operations.
Navigating the robotic horizon
The encroachment of AI and robots on surgery is inevitable, but it need not spell doom for surgeons. Rather than resistance, the path forward lies in adaptation. Surgeons must advocate for hybrid models where AI augments human judgment, not supplants it—ensuring transparency in algorithms to combat black-box issues.12 Continuous education is essential: the surgical curricula should integrate AI literacy, emphasising ethical use and bias mitigation.17 Policymakers must enforce regulations on data privacy, cybersecurity and equitable access to prevent disparities.19
Reconstructive surgery, a cornerstone of plastic surgery, demonstrates remarkable resilience against the disruptive potential of AI and robotics, primarily due to its inherent complexity, patient-specific variability and the indispensable role of human expertise. Unlike routine aesthetic procedures that can be standardised and partially automated through AI-driven simulations and predictive modelling, reconstructive efforts—such as those addressing trauma, congenital defects or post-cancer tissue restoration—demand adaptive decision-making in unpredictable scenarios, where anatomical irregularities and real-time complications defy algorithmic predictability.22 Robotics and AI excel in augmenting precision, such as in microsurgery where robotic systems filter tremors and enhance visualisation, potentially reducing operative times and improving outcomes in flap reconstructions or lymphatic procedures.22 However, these technologies primarily serve as assistive tools rather than replacements, as evidenced by studies showing that while AI can simulate outcomes and monitor recovery, it struggles with the ‘sim-to-real’ gap—the transition from controlled simulations to the chaotic realities of human biology, ethical dilemmas and interdisciplinary collaboration. Experts emphasise that AI’s black-box nature, biases in training data and inability to replicate surgeons’ intuitive judgment in high-stakes, bespoke cases, ensure human oversight remains central to mitigating risks like algorithmic errors or cybersecurity vulnerabilities.21,23 Furthermore, regulatory hurdles, liability concerns and the need for surgeon-led integration slow full automation and position reconstructive surgery as a field where innovation enhances rather than erodes professional resilience.24 As AI evolves, reconstructive surgeons who embrace hybrid models—combining robotic assistance with their tactile skills and empathy—will not only adapt but thrive, preserving the specialty’s human-centric essence in an increasingly tech-driven landscape.6,25
More broadly, surgeons should lead this transformation, shaping AI and robotics as a tool for better care rather than a replacement. By embracing innovation with caution, the profession can preserve its human essence while harnessing technology’s power. The scalpel may evolve, but the surgeon’s humanity and insight is irreplaceable.
Suggestions to navigate the great disruption
-
Stay broad, narrow practice interests increase vulnerability.
-
Keep emergencies and trauma in your practice. More unpredictable cases are less likely to be replaced by robotics.
-
Innovate, plastic surgery has a long history of finding solutions and changing direction. (Who knows what ‘super microsurgery’ may be possible with incredible magnification and dexterity.)
-
Avoid ‘cookbook’ operations, robotics is most likely to replace areas that are the most routine and reproducible.
-
Keep reconstructive surgery in your practice. Complex reconstructive surgery requires human planning and innovation.
-
Consider regional and remote areas as part of your practice. Expensive robotics are most likely to commence in larger tertiary centres due to cost.
-
Stay united and support your society so that they can advocate as a collective.
-
Embrace your humanity and personal interaction with patients. This cannot be replaced.