Introduction
Craniosynostosis is a congenital condition affecting approximately one in 2500 live births, characterised by the premature fusion of one or more cranial sutures.1 This abnormal suture fusion restricts cranial growth at the affected site while leading to compensatory expansion at the remaining open sutures. The resultant skull deformity can contribute to increased intracranial pressure (ICP), neurocognitive delays and aesthetic concerns, necessitating surgical intervention to optimise functional and psychosocial outcomes.1–3
Effective surgical management of craniosynostosis is influenced by patient age, severity of deformity and institutional preferences. Craniosynostosis can be treated using either minimally invasive suturectomy techniques or traditional open cranial vault remodelling.4 One of the minimally invasive approaches involves an endoscopic strip craniectomy (ESC) combined with postoperative helmet therapy, first popularised by Barone and Jimenez in 1999; another involves intraoperative spring-assisted expansion.5,6
The choice of surgical approaches remains a subject of ongoing debate, with proponents of suturectomy emphasising its advantages in younger infants due to their skull pliability and capacity for guided postsurgical remodelling.7 Critics highlight concerns about treatment failure rates associated with earlier, less technologically advanced techniques. However, modern advancements in helmet therapy and other adjuncts have substantially improved the efficacy of minimally invasive approaches, making them a viable alternative to traditional open procedures.8
Historically, our institution’s treatment algorithm for single-suture craniosynostosis was primarily age-independent: patients with unicoronal or metopic craniosynostosis were managed with fronto-orbital advancement and remodelling regardless of the age at diagnosis. Sagittal craniosynostosis was treated with spring-assisted cranioplasty if diagnosed before six months of age and with total cranial vault remodelling if diagnosed later. Lambdoid craniosynostosis was uniformly treated with posterior vault remodelling, again irrespective of age.
In November 2022, the Sydney Children’s Hospitals Network was the first in Australia to introduce ESCs with postoperative moulding helmet therapy. For patients diagnosed before four months of age, ESC is now offered for all types of single-suture craniosynostosis—metopic, sagittal, lambdoid and unicoronal—as well as for some cases of multi-suture craniosynostosis. For patients diagnosed after four months of age, our protocol remained unchanged. The aim of this study was to evaluate our initial experience with craniosynostosis patients treated with ESC and helmet therapy.
Methods
Following institutional review and ethics approval from the Sydney Children’s Hospitals Network Human Research Committee (HREC 2021/ETH11396), a retrospective review of consecutive patients with craniosynostosis managed with ESC and helmet therapy at the Sydney Children’s Hospitals Network (Children’s Hospital at Westmead and Sydney Children’s Hospital, Randwick) between November 2022 and January 2025 was performed. All medical records available on PowerChart (Cerner, Sydney, Australia), including electronic records and scanned paper records, were reviewed and relevant data extracted using REDCap electronic data capture tools (REDCap, Seattle, Washington, USA). No concurrent control group or morphometric comparisons were performed in this chart review.
All patients referred to our centre with craniosynostosis were assessed in a multidisciplinary clinic consisting of plastic surgery, neurosurgery and ophthalmology.
Surgical technique
Under general anaesthesia with endotracheal intubation, patients were positioned based on the affected suture and head shape: prone for sagittal and lambdoid craniosynostosis, and supine for metopic and unicoronal craniosynostosis. Incisions were infiltrated with xylocaine 1% with epinephrine. An arterial line and two intravenous catheters were routinely placed. Prophylactic antibiotics and tranexamic acid were administered.
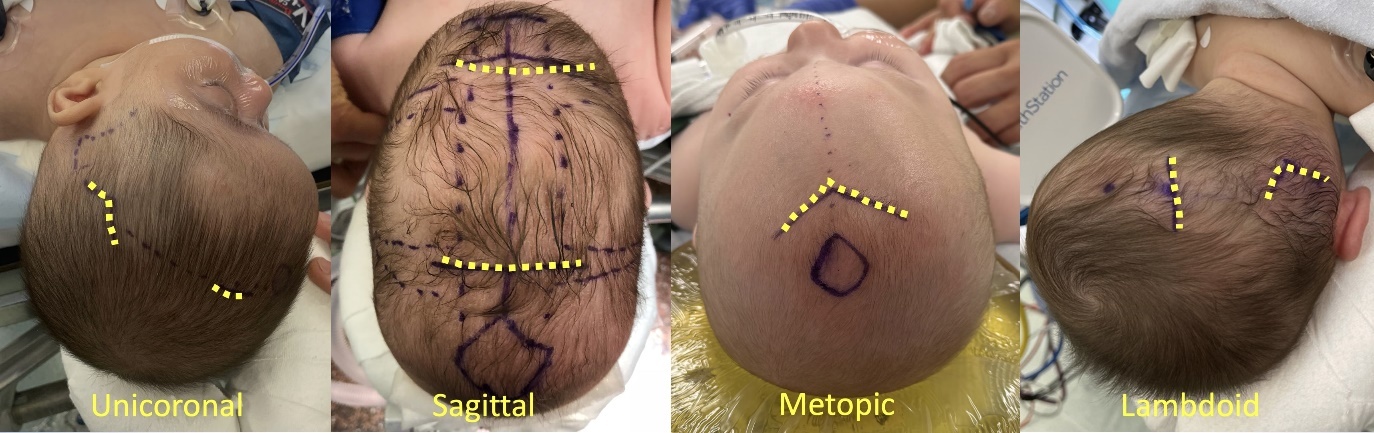
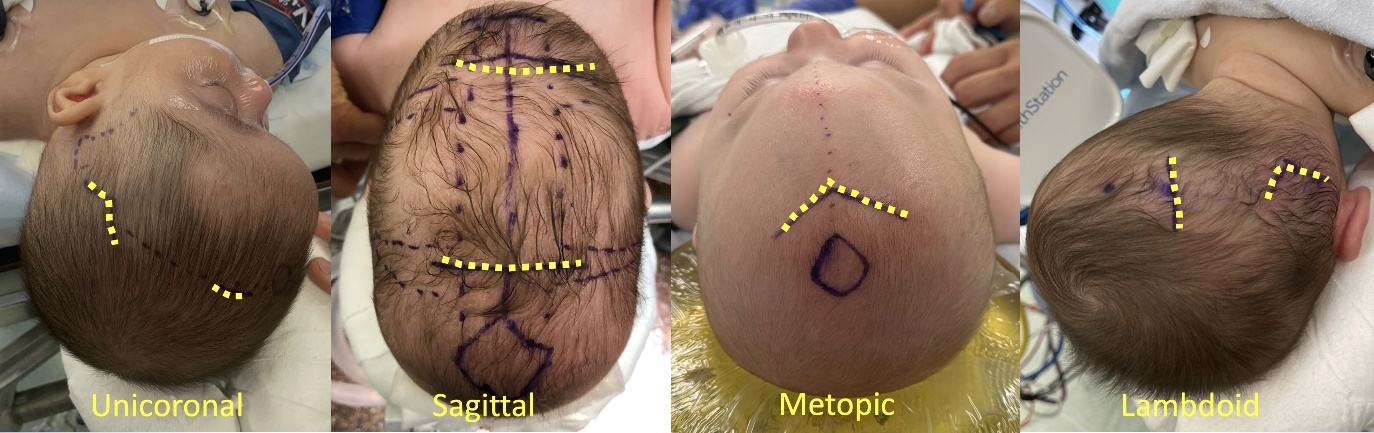
Incision placement was tailored depending on the affected sutures (Figure 1). For sagittal craniosynostosis, both the anterior and posterior fontanelles were located, and two 4 cm transverse incisions, 8 cm apart, were made between the fontanelles. For metopic craniosynostosis, the anterior fontanelle and frontonasal sutures were located and marked, and a midline 4 cm V-shaped incision was made just behind the hairline. For unicoronal craniosynostosis, the anterior fontanelle was marked, and a 3 cm incision was made just lateral to it, on the affected side. Another 3 cm V-shaped incision was made in the temporoparietal area just above the temporal squamosal line. For lambdoid craniosynostosis, the posterior fontanelle was marked and an incision was placed just lateral to it, on the affected side. A V-shaped incision was also placed just above the mastoid bulge.
A 3–4 cm wide craniectomy was performed from the anterior fontanelle to the posterior fontanelle in cases of sagittal craniosynostosis with no barrel staves. For the remaining cases, a narrow craniectomy (typically 1–2 cm wide) was performed along the length of the synostosed suture, extending from the associated fontanelle(s) to the suture’s anatomical endpoints. In the case of unicoronal craniosynostosis, an extension to include the sphenofrontal suture was also created. A 30 degree endoscope may be employed to visualise the interface between the dura and bone, and assist in dissection and haemostasis. Haemostasis was achieved with bipolar cautery, bone wax and fibrin sealant as needed. The scalp was closed in layers with resorbable sutures. No head dressings or drains were used.
Patients were monitored on the floor and discharged on the first postoperative day.
Helmet therapy was initiated within one to two weeks. Patients were seen every six to eight weeks for helmet adjustments to optimise the cranial shape based on 3D photography and moulding. A CT scan was routinely obtained one year postoperatively and 3D photographs were obtained at each helmet moulding appointment. From one year postoperatively, patients were reviewed on a yearly basis.
Results
Patient demographics
A total of 82 patients who underwent ESC for craniosynostosis between November 2022 and January 2025 were identified in the dataset. There were 25 females and 57 males with a mean age at surgery of 3.4 months (range 2.2–6.2 months). Eleven (13.4%) patients were born prematurely, accounting for age outliers. Sagittal craniosynostosis was the most prevalent diagnosis (n = 39, 47.5%) followed by metopic craniosynostosis (n = 29, 39%) and unicoronal craniosynostosis (n = 11, 13%). Less common presentations included lambdoid craniosynostosis (n = 1, 1.2%), and multi-suture craniosynostosis (n = 2, 2.4%).
Ten (12.1%) patients had diagnosed genetic mutations and four (4.8%) patients had syndromic craniosynostosis including Beckwith-Wiedemann (n = 1), Saethre-Chotzen (n = 2), and craniofrontonasal dysplasia (n = 1). Mutations included an FGFR3 mutation, HTT gene chromosome 4 deletion, deletion of chrom15q11.2, PRRX1 deletion and 19p13.3 duplication. Average weight at time of surgery was 6.17 kg (range 4.27–8.25 kg). Sixteen (19.5%) patients had comorbidities, including gastro-oesophageal reflux, laryngomalacia, hip dysplasia, macroglossia and hearing loss.
Perioperative care
Mean anaesthetic time was 159 minutes (range 86–258 minutes) and mean surgical time was 82 minutes (range 38–224 minutes). Thirty-six (43.9%) patients received an intraoperative blood transfusion, while only four (4.9%) needed a postoperative transfusion for an overall transfusion rate of 48.7 per cent. The average volume of transfused blood (red blood cell) was 108.2 ml. Thirty-four (41.4%) patients received albumin infusions and one patient received plasma. Tranexamic acid was administered intravenously intraoperatively in 69 patients (86.3%). In our cohort, 99 per cent of patients received prophylactic intraoperative antibiotics. The mean length of stay was 1.6 days (range 1–12 days). Mean follow-up was 16 months (range 5–30 months), with 52 (62%) patients having a follow-up of at least one year.
Helmet therapy
Helmet therapy was initiated for all patients following surgery; however, information on duration of therapy, compliance and number of helmets was only available for a subset of patients. Helmets were worn between six to eight months postoperatively and discontinued at about 12 months of age. Five (6.1%) patients were documented as not tolerating helmet therapy. Two (2.4%) patients developed dermatitis due to the helmet therapy. One (1.2%) patient developed full-thickness pressure ulceration related to helmet use. Patients who completed helmet therapy needed an average of 3.5 helmets and 10 appointments for various helmet adjustments.
Complications
Intraoperative complications were reported in five patients (6%) and included venous air embolism (n = 1), accidental extubation (n = 1), laryngospasm or airway obstruction (n = 2), and radial artery vasospasm resulting in an abandoned procedure (n = 1). None of these complications led to intraoperative mortality or immediate reoperation. Postoperative complications were documented in 12 (14.6%) patients. Two patients required reoperation for infected seroma and hematoma management. Seromas were the most common complication, occurring in five patients. Superficial wound infections requiring antibiotics occurred in three patients. Less frequent complications included pneumonia (n = 1), subglottic oedema (n = 1) and a single case of intraventricular haemorrhage (n = 1).
Intracranial pressure
Preoperatively, fundoscopic examination showed evidence of papilloedema in only one patient with multi-suture craniosynostosis (lambdoid and bicoronal). Four patients (4.8%) had mildly prominent lateral ventricles on the preoperative CT scans but no papilloedema. Postoperatively, three (3.6%) patients required surgical intervention due to raised ICP after undergoing an ESC. One patient with sagittal craniosynostosis underwent ICP monitoring, which subsequently led to anterior cranial vault reshaping. Two patients (sagittal and multi-suture craniosynostosis) required ventriculoperitoneal shunt insertion due to the development of hydrocephalus.
Long-term outcomes
Only one patient underwent secondary cranial vault remodelling due to persistent cranial dysmorphology after helmet therapy. Interestingly, three patients were noted to have developed secondary suture fusions on one-year follow-up CT scans without any evidence of associated skull dysmorphology.
Discussion
Strip craniectomy as a treatment of craniosynostosis is not a new concept, but the technique has evolved considerably since the efforts in the 1890s of Lannelongue9 and Lane.10 Since Barone and Jimenez reintroduced this procedure with postoperative moulding helmet therapy in 1999, it has become an effective tool in the armamentarium of procedures to manage craniosynostosis.5 However, it was not until late 2022 that the Sydney Children’s Hospitals Network modified its treatment algorithm to include this as an age-dependent (< 4 months of age) treatment opportunity for infants with craniosynostosis. Our findings support existing evidence that early, minimally invasive intervention can achieve excellent surgical outcomes with low complication rates and short hospital stays.8,11–14
The technique is dependent on performing a suturectomy at an age where the velocity of brain growth is high and the bone is reasonably thin, allowing for the soft tissue functional matrix to remodel the calvarium with the assistance of an external moulding helmet. Previous studies in the literature have reported its effectiveness in single-suture, multi-suture and syndromic craniosynostosis with shorter procedure times, shorter length of stays, lower transfusion rates, lower complications and significant cost savings compared to open vault remodelling procedures.14,15
Successful adoption of this approach requires several caveats. It is necessary to have a comprehensive and dedicated orthotics service who can scan the infant heads, create the helmets and be available for adjustments every six to eight weeks. Financial support to pay for the helmets may also be an issue. The postoperative burden of care placed on parents to assess their child daily for helmet fit and skin breakdown, and travel to up to 10 postoperative appointments, can impose a notable strain, both logistically and financially. Geographical distance from the hospital may be an issue for rural families. It is necessary to confirm parental compliance before embarking on surgery. Finally, some patients may not tolerate the helmet: there were five (6.1%) patients who did not successfully complete postoperative helmeting. It is unknown if these were due to parent-related or patient-related issues. However, we feel that doing an ESC does not preclude the opportunity of performing an open vault reshaping procedure at a later date, as was the case in two of our patients.
There remains considerable data to harvest from this patient cohort. Despite reports in the literature, the influence of early surgery on neurocognitive outcome remains a source of debate. Previous multi-centre studies spearheaded by John Persing at Yale have suggested that children undergoing surgery under six months demonstrated significantly higher full-scale and verbal IQ, as well as superior academic abilities in reading, spelling and mathematics, and that a whole-vault cranioplasty was associated with higher scores in visuomotor integration, full-scale intelligence quotient, verbal intelligence quotient and reading-related achievement compared with strip craniectomy.16,17 However, a recent multi-centre study by Magge and colleagues assessed long-term cognitive outcomes of school-age children with sagittal craniosynostosis who had undergone either endoscopic surgery or open calvarial vault surgery.18 It demonstrated there were no statistically or clinically significant differences in cognitive outcomes among school-age children associated with type of surgical procedure used to repair non-syndromic sagittal craniosynostosis. It will be interesting to examine neuro development in our cohort and compare to the traditional open techniques employed at Sydney Children’s Hospitals Network.
There were 11 patients with unicoronal craniosynostosis in our study. It has been reported for unicoronal craniosynostosis that children treated with ESC and helmeting had less severe strabismus and less need for surgical correction compared to those undergoing open frontal-orbital advancement.19 It was speculated this may be due to earlier timing of surgery or favourable improvement in orbital anatomy. We have not had the opportunity to determine if this was the case in our cohort.
Our blood transfusion rates (48.7%) are higher than those reported in the literature (11– 26%).14 This may be due to having multiple anaesthetists across two hospital sites with differing transfusion philosophies, as well as challenges in estimating blood loss in young infants. Interestingly, Thompson and colleagues compared endoscopic versus open repair for craniosynostosis across 31 different institutions and demonstrated that in low volume centres, transfusion rates were significantly higher than in high volume centres (47% versus 11%), suggesting that there is expertise gained with experience in this patient cohort.14 It is expected that transfusion rates will diminish with time at the Sydney Children’s Hospitals Network.
Although we did not measure parent satisfaction in this study, only one of our patients underwent a total cranial vault remodelling to improve head shape due to persistent cranial dysmorphology after undergoing an ESC with helmet therapy. This is in line with many papers in the literature supporting the effectiveness of ESC and helmeting in terms of normalisation of head shape.1,5,6,13–15
Complications in our cohort were infrequent and largely minor. The 2.4 per cent return to theatre rate in our series is consistent with the surgical literature. Massenburg and colleagues, in a large National Surgical Quality Improvement Program-based analysis, found a reoperation rate of 2.4 per cent and a readmission rate of 3.0 per cent across nearly 4000 patients undergoing craniosynostosis repair.20 Only one of our patients had elevated ICP preoperatively as detected by the presence of papilloedema but it was a concern in three (3.6%) patients post-ESC. Of the latter, two underwent ventriculoperitoneal shunting, and one required ICP monitoring followed by anterior vault remodelling. Previous studies have demonstrated that the incidence of postoperative late-onset intracranial hypertension ranged from 4 per cent to 7.1 per cent.2,21 Interestingly, Makoshi and colleagues demonstrated that ESC yields an immediate intraoperative reduction in ICP, with a 64 per cent mean decrease following suture release and no patients exhibiting ICP > 10 mmHg at closure.22 However, it is well recognised that these patients need to be monitored for several years.
Limitations
This study has several limitations. The retrospective nature introduces risk of selection and information bias. Data on helmet therapy duration and compliance were incomplete, which limits interpretation of long-term outcomes. Additionally, not all patients underwent postoperative imaging or ophthalmologic review, potentially underestimating the incidence of raised ICP. The absence of severity stratification; blinded morphometrics on the basis of scans or 3D photography; and standardised aesthetic ratings, limits conclusions about head-shape normalisation. This is a subject for future studies comparing ESC with helmet therapy with other techniques (including spring-assisted cranioplasty and fronto-orbital advancement and remodelling).
Conclusion
This study supports ESC followed by helmet therapy as a safe treatment for infants under four months of age with craniosynostosis and should be an available treatment option in craniofacial centres. We have demonstrated a low incidence of complications and short hospital stays. However, the need for frequent helmet adjustments poses a significant burden on families, which must be considered in preoperative planning and counselling. Increased attention to postoperative ICP surveillance may further optimise care and long-term prognosis.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship and/or publication of this article.
Revised: September 10, 2025 AEST; November 14, 2025 AEST