

Introduction
Two in three Australians will be diagnosed with keratinocyte cancers in their lifetime.1 Basal cell carcinomas (BCCs) and squamous cell carcinomas (SCCs) occur most commonly in the head and neck region, particularly the nose, due to its prominent position on the face.2 The nose represents a unique reconstructive challenge because of its three-dimensional convexity, composite tissue structure and high aesthetic demands. In addition, the lower-third aesthetic subunit of the nose presents unique challenges, arising from its thick, sebaceous skin and limited laxity.3
Since its modification by Zitelli in 1989,4 the bilobed flap has been a workhorse local flap for nasal reconstruction of small-to-medium-sized defects, primarily at the nasal tip. The bilobed flap is a double transposition flap, classically composed of a primary lobe of similar size to the defect and a secondary lobe that creates a donor site defect that can be directly closed. Despite its popularity, several technical nuances are required to achieve optimal results, particularly in the nasal ala, where it can blunt the alar groove and produce asymmetric aesthetic outcomes.5
We present the senior author’s experience with medially-based bilobed flaps for nasal alar reconstruction.
Operative technique
The flap is designed medially-based and a burrow’s triangle is created cranially at 45–60° (Figure 1). The primary lobe is designed in the standard fashion. The secondary lobe is designed perpendicular to the lower eyelid-cheek junction to ensure that the final scar does not cause cicatricial medial ectropion. The alar groove is not undermined in order to preserve its role in maintaining facial symmetry.
The operation is performed using diathermy on a low setting and the wound is closed in layers, with non-dissolvable sutures placed in the epidermis to minimise perisutural inflammation (Figure 2). The wound is dressed with Mepitel (Mölnlycke Health Care, Gothenburg, Sweden) at the primary layer and gauze with Hypafix (Essity AB, Stockholm, Sweden) at the secondary layer to provide pressure and prevent haematoma formation. Patients are advised to avoid wearing glasses for at least two weeks until scar maturation.
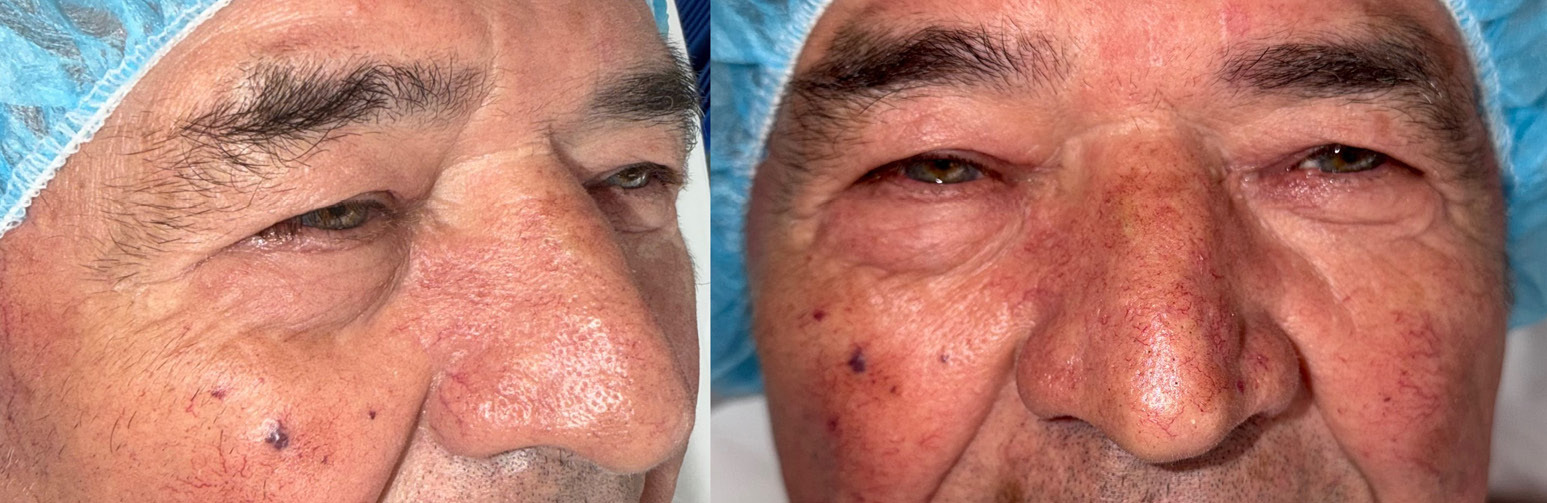
We have successfully performed this technique in a series of 15 patients and report no complications (Figure 3).



Discussion
Nasal alar reconstruction poses a significant aesthetic challenge to the plastic and reconstructive surgeon due to its unique fibromuscular structure, which dynamically alters form during respiration, and its complex three-dimensional shape.3–5
In 2014, Tregaskiss and colleagues described the nasal sidewall island inversion flap, an innovative, single-stage technique for alar reconstruction using an angular artery branch–based island flap.6 While promising, this flap is technically demanding, carries a risk of webbing at the alar groove, and may not adequately cover anterior alar defects.
Bilobed flaps remain a cornerstone of nasal reconstruction for small-to-medium defects following oncological resection. Zitelli’s 1989 modifications4 improved aesthetic outcomes and reduced donor-site morbidity, particularly standing cone deformities. His principles included: limiting the total arc of rotation to 90–110°; wide undermining, laterally-based lobes; restricting use to defects ≤ 15 mm in diameter; and ensuring that the primary lobe matches the defect size. These principles are straightforward in theory but often difficult to apply in practice due to the three-dimensionality of nasal anatomy and variability in skin quality/sebaceousness. In less experienced hands, bilobed flaps may result in complications such as pincushioning, prominent standing cone deformities and nasal asymmetry from scar contracture.
We propose three modifications that, in our experience, improve reconstruction of the nasal ala, particularly for anterior defects:
-
a medial-based flap design allows the primary lobe to transpose into the defect without effacing the alar groove
-
the primary defect is triangulated at 45–60° cranially and the secondary lobe is placed perpendicular to the lower eyelid-cheek junction
-
the alar groove is preserved and not undermined.
Potential limitations of our modifications include scar sensitivity along the secondary lobe donor site in patients wearing glasses. However, this typically resolves with scar maturation. Upon rotation of the primary lobe, some bulging at the supratip region may occur from standing cone deformity. This can be adequately prevented by cranial triangulation of the flap, although in our series it ultimately resolved with scar maturation. Sometimes tumours may need to be re-excised and a well-healed flap may make this challenging. We would recommend surgeons record clinical photographs of their design prior to performing this flap.
Conclusion
Keratinocyte cancers are highly prevalent in Australia and the bilobed flap remains one of the most appropriate local flap options for post-oncological nasal reconstruction, particularly at the tip. Despite multiple refinements, the bilobed flap remains technically challenging for inexperienced surgeons because of the complex three-dimensionality of the nasal tip and the nuanced movements of the flap across a convex surface. We present three modifications that are practical, reproducible and straightforward to apply, each contributing to consistently improved aesthetic outcomes following flap inset.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship and/or publication of this article.
Revised: March 12, 2026 AEST