Aim
The aim of this article is to introduce a discussion on more objective ways to assess scars as impairments in the Australian legally-compensable insurance schemes for workers compensation and motor vehicle accidents. The following is the opinion of the author, who has five years’ experience in the field of scar assessment for compensable schemes, as well as over 30 years’ experience as a consultant plastic surgeon.
Introduction
Plastic surgeons who perform impairment evaluations in the medico-legal jurisdictions covered by motor vehicle third party or workers compensation insurance schemes in Australia must be accredited to do so in their areas of expertise. One area they are called upon to assess is that of scars.
Whole person impairment (WPI) measures degrees of impairment that may be combined with assessments of impairments to individual body systems, such as limb injuries, neurologic injuries and injuries to other body systems. The assessment tools used for both workers compensation and Compulsory Third Party (CTP) insurance schemes in the various states of Australia historically relied upon the American Medical Association’s Guides to the evaluation of permanent impairment, with some notable variations. The main editions used are the fourth edition (AMA4)1 and fifth edition (AMA5).2
In New South Wales (NSW) the pitfalls in the AMA guides led to the introduction of new tables in both the workers compensation guidelines3 and motor accident guidelines4:
-
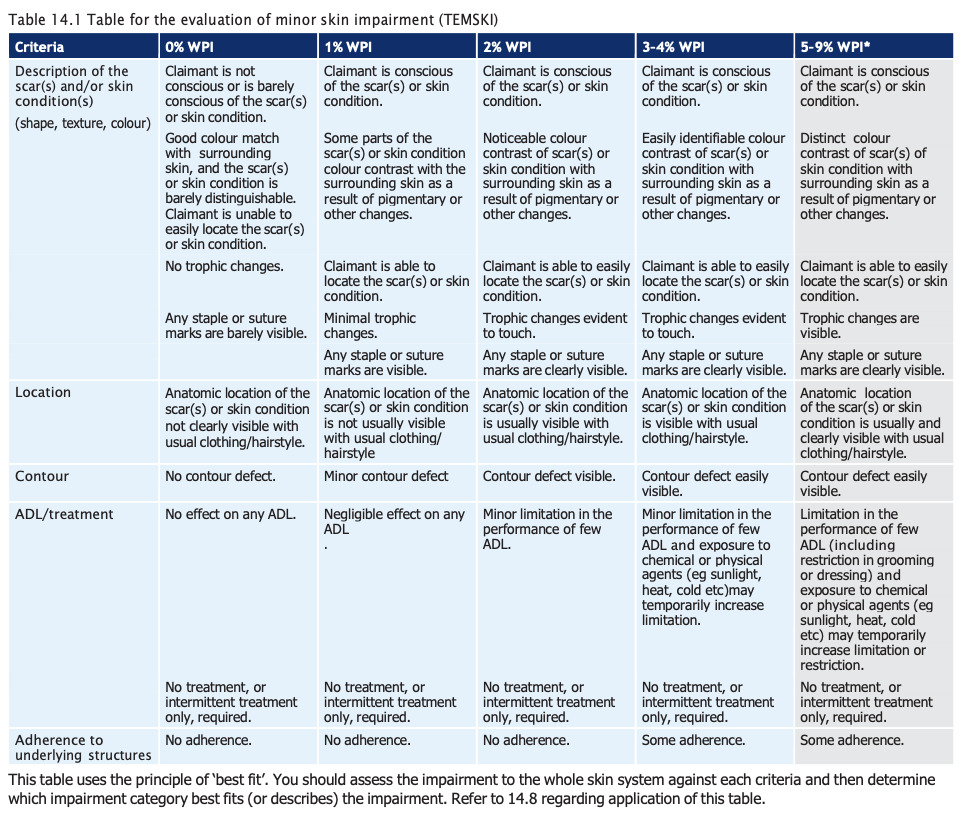
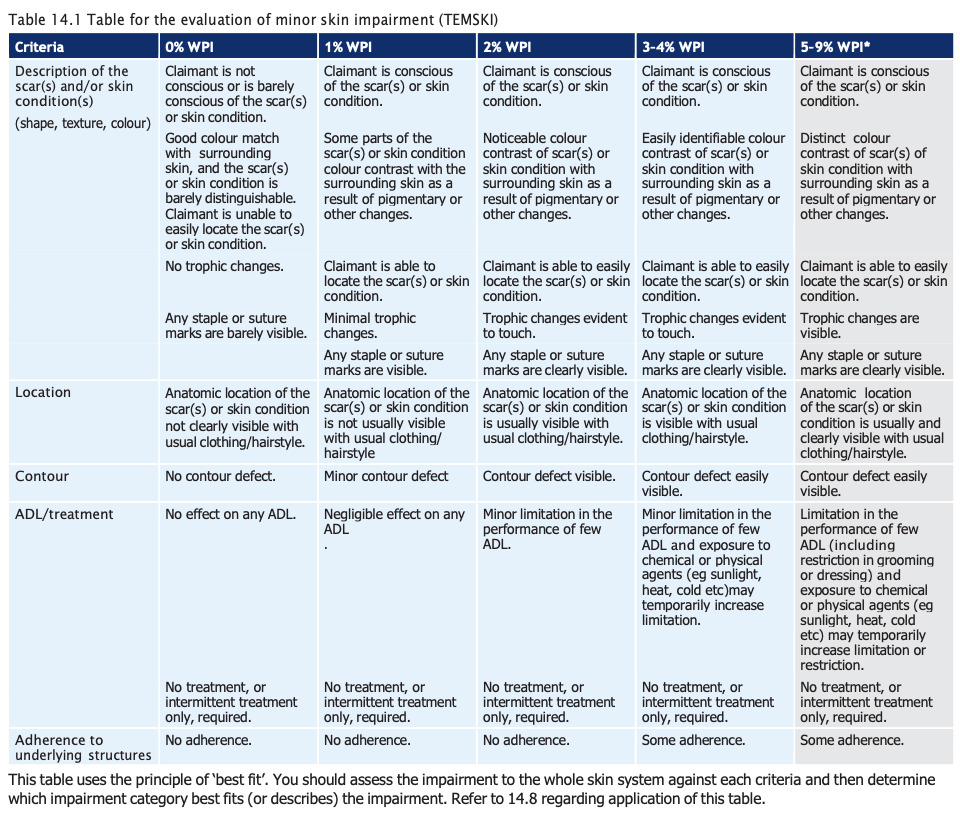
In the workers compensation guidelines, Table 6.1 replaces AMA5 Table 11-5 for the evaluation of facial disorders and disfigurement. Also, Table 14.1, Table for the evaluation of minor skin impairment (TEMSKI), modifies AMA5 Table 8.2 for 0–10% WPI. The TEMSKI gives five categories of ‘minor scars’, with WPIs varying between 0% and 9%.
-
The motor accident guidelines do much the same, using the TEMSKI but retaining AMA4 Chapter 13 on its own for facial disfigurement.
The TEMSKI (Figure 1) is now used in the workers compensation guidelines of all Australian states except Victoria, and it is used in the Northern Territory but not the Australian Capital Territory.3,5–9 Victoria relies on AMA5 only.10 In the Australian Capital Territory there are two schemes, Private and Comcare.11 Comcare has its own evaluation scheme, which has advantages over the TEMSKI. In the jurisdictions using the TEMSKI, scar impairments are measured directly as WPI values and may be combined with other impairments at the WPI level to give final scores of impairment.
The WPI assessment of scarring is probably the least objective in the entire assessment process, either for workers compensation or CTP insurance schemes.
Scar assessment issues
There are some common pitfalls in assessing scars that may lead to poor and non-objective assessments. Some examples of these follow.
Assessments made online by Zoom or other audiovisual link
COVID-19 lockdowns were the spawn for online consultation in a wide variety of medical fields. Online assessments are now relatively commonplace, especially for claimants living remotely. However, the quality of video images can vary very widely, depending on the equipment used, the ability of the claimant to use it correctly and issues relating to ‘anatomical privacy’, for want of a better term.
The assessment of scars requires much more than a two-dimensional digital image. Excellent lighting, close inspection (sometimes under magnification), the ability to manipulate positions to obtain the best view and even palpability of scars are all factors that cannot be adequately controlled in an online assessment. In the author’s opinion, except in extremely rare circumstances, scar assessments done online are frequently inaccurate. The author refuses to do them for that reason.
Assessor’s emotional bias
Emotional bias is more difficult to avoid when assessing serious scars in children. It is also more common when assessing facial scars. As in clinical practice, it is important to maintain an objective and fully professional approach to the assessment. One tool that may help is an assessment of the scar’s effect on activities of daily living. However, that suffers from a degree of subjectivity and relies on honest reporting by the claimant.
When such adverse effects caused by the appearance of scars on a claimant’s social functioning or sexual activity become excessive or unusual, instead of including that as part of the physical assessment, such assessment should be, in the author’s opinion, undertaken by a psychologist. The scar assessment should be on the basis of objective physical findings only.
The ‘hired gun’ syndrome
Despite the legislative mandating of non-bias in expert medico-legal reports, certain contradictions and ‘fluidity’ in the criteria in the TEMSKI permit over- or under-evaluation of scarring, sometimes creating quite large gaps between the WPI assessments of experts for the claimant versus those for the insurer.
The effects of scars on function
When a claimant states that their scar affects certain functional activity amounting to an impairment, either work-related or otherwise, using criteria of functional loss to upgrade a WPI scar assessment is inadmissible. For example, if there is a scar contracture across a joint, that contracture should be assessed as a loss of active range of movement and not be part of the scar assessment. A facial scar that limits closing of an eye may require additional assessment by an ophthalmologist and one that affects eating by an otolaryngologist. The scar assessments should not be upgraded because of those impairments.
Another aspect is sensory change in or around scars. Sensory loss or dysaesthesia can only be assessed when it applies to a known anatomically-named nerve and is not assessable as part of a scar. Likewise, a painful scar cannot be objectively assessed, just like any other cause of pain, with rare exceptions. This is because of the subjective nature of pain and the unreliability of assessment tools, such as the visual analog scale.
The AMA4 and AMA5 chapters on skin tend to discuss medical, non-traumatic skin conditions in greater detail than scarring from trauma or surgery. That is one reason why the NSW State Insurance Regulatory Authority (SIRA) and other state authorities introduced the TEMSKI. It attempts to introduce more descriptors for scars and skin conditions and their impairments than are found in the AMA4 and AMA5 chapters on skin, with the aim of making evaluation more accurate and objective.
TEMSKI issues
Those of us regularly assessing scars using the TEMSKI criteria have noticed that it suffers from several flaws. In the assessment of scars or skin conditions, the TEMSKI relies on the concept of ‘best fit’, being the greatest number of descriptors or criteria in the column chosen that are relevant, compared to other columns with smaller numbers of relevant descriptors. However, the concept of best fit is not clearly defined and appears to clash with the claim that all criteria within the column chosen must be met, unless the assessor provides detailed reasons why all criteria have not been met. At times this introduces problems, which are further discussed below.
Scar description
In the author’s opinion, the descriptive language for a scar in TEMSKI could be tighter. The phrases ‘usually visible’, ‘not usually visible’ and ‘usually and clearly visible’ should be defined better. I would suggest three categories of visibility:
-
Not clearly visible from conversation distance of one metre in good light.
-
Just visible from conversation distance of one metre in good light.
-
Clearly visible from conversation distance of one metre in good light.
Trophic change
There is no definition of ‘trophic change’ in the abovementioned guidelines. Categories 2% WPI and 3–4% WPI talk about ‘trophic changes evident to touch’, whatever that means. Trophic change for a scar may mean atrophy or hypertrophy, whereas for a skin condition, such as severe contact dermatitis or actinic skin damage, it might mean another thing altogether. If the various state guidelines wish to have TEMSKI apply to both scars and other skin conditions, the text of the guidelines should clearly define what is meant by trophic change in either scars or typical skin conditions, preferably by giving their own examples and/or typical colour photographs.
Relative values
There is no relative value placed on each of the 10 criteria listed in each column of the TEMSKI. For example, what value for a WPI does the statement, ‘Claimant is (not) conscious or is barely conscious of the scar(s) or skin condition’ infer? This evaluation borders on a psychological evaluation, as some personality types will exaggerate their consciousness of even minor scars and some will ignore quite obvious scars. That category could be eliminated and replaced with an activities of daily living category, which is arguably more objective.
The ‘best fit’ and ‘all of the criteria’ quandaries
The NSW workers compensation guidelines state3:
14.8 The TEMSKI is to be used in accordance with the principle of ‘best fit’. The assessor must be satisfied that the criteria within the chosen category of impairment best reflect the skin disorder being assessed. If the skin disorder does not meet all of the criteria within the impairment category, the assessor must provide detailed reasons as to why this category has been chosen over other categories. [emphasis added]
There is wide variation amongst examiners as to what constitutes best fit. For example, the fact that a small scar on the back of a hand is ‘visible with normal clothing and hairstyle’ may force an examiner to increase an impairment to 2% WPI or even 3–4% WPI, when the majority of other criteria are not present and the real WPI is 1% or even less. In order to justify allowing an assessor to eliminate from the assessment one descriptor, such as visibility in usual clothing, the rules state that such a move must be justified by the assessor providing ‘detailed reasons as to why this category has been chosen over other categories.’ This introduces an unnecessary burden on the assessor, in the author’s opinion.
Moreover, when highly visible and otherwise disfiguring scars on say, the forearm or leg, are covered by ‘normal clothing’ (eg, long trousers, long sleeves), they are disallowed by the ‘all of the criteria’ rule for all categories above 1% WPI. That forces the assessor to downgrade an obvious assessment that may exceed 2% or considerably greater, back to 0% or 1%, which are the only categories where ‘Anatomic location of the scar(s) or skin condition is not usually (or clearly) visible with usual clothing/hairstyle’ apply.
In the author’s opinion, the elimination of this descriptor altogether would make the assessment more objective.
Proposed scar evaluation method
Objective measurement
There is clearly a need to introduce a more objective measurement tool for scar evaluation than the current TEMSKI. Based on numerous assessments of scars, where the author has observed a wide variation of assessments made by fellow plastic surgeons, the author’s suggested criteria are set out in Table 1.
Firstly, the term ‘minor’ should be deleted from the description in the new table, which could be called ‘TESKI’ instead. A table which allows up to a 9% WPI for scars is clearly not referring to minor scars.
In respect of relative value, this article proposes a points system for each descriptor. Evaluation of final WPI would then depend on the summation of points for each category and would give a mathematical value to the concept of best fit. It is suggested that points could vary between 1 and 3 in order of importance/severity. Descriptors should be listed and each one given a range of values by the examiner. The WPI suggested should have a summation value within a range for each evaluation level. The total for 5–9% WPI should be a score greater than 20. For a 0% WPI the score should be less than 4. For other levels, see Table 2.
Further suggestions
Scar evaluation is very visibility-dependent. The author would suggest that visual examples be provided in any update of the NSW workers compensation guidelines3 and motor accident guidelines,4 and in other state jurisdiction guidelines. As these guidelines are now available largely online, the provision of suitable full-colour example photographs to guide assessors would be appropriate.
The proposed tables could be open for discussion with a panel of expert assessors. Then, after any modifications, they could be submitted to all jurisdictions where TEMSKI is used for consideration. The addition of examples including photographs of typical cases should, in the author’s opinion, be strongly suggested.
Scar assessments greater than 3% WPI should be confined to plastic surgeons or dermatologists.
Discussion
Objective evaluation of scar quality has been the subject of a large number of scientific articles. The main focus has been on evaluation of scars in clinical trials, be they about surgical or other techniques of scar management. The Vancouver Scar Scale12 introduced in 1990 has been accepted as a standard tool for scar evaluation in some clinical scenarios. However, it is mainly used to evaluate burn scars, which are in a minority in most compensable cases.
In a meta-analysis of 75 articles, Verhaegen and colleagues reviewed a number of sophisticated techniques for analysis of scar quality, some requiring highly technical equipment, such as tristimulus reflectance colorimetry and narrow-band spectrophotometry.13 Such tools measure scar characteristics like colour, thickness, relief, pliability and surface area. Inter alia, Verhaegen’s article makes the following conclusions:
For research purposes, objective quantitative data are generally considered most useful; but for clinical and practical purposes, subjective scar assessment scales are often more convenient and more frequently used. Furthermore, subjective scar assessment scales provide the possibility of including the patient’s opinion.
It is highly unlikely that the time, effort and cost involved in using these sophisticated techniques for scar assessment would be adopted by those agencies involved in scar assessments resulting from compensable injuries in Australia. Nevertheless, it is the author’s contention that the current system could be significantly improved at no extra cost.
Conclusion
Scar evaluation in compulsory compensation schemes in Australia currently has significant drawbacks. It is suggested that an updated version of the widely-used TEMSKI table could improve the objectivity and reliability of scar evaluations for permanent impairment assessment.
Conflict of interest
The author is a Health practitioner authorised to give evidence (skin, facial injury) in the NSW CTP scheme and a Permanent impairment assessor for the NSW workers compensation scheme (upper limb, skin and scars). SIRA had no involvement with the preparation of this article or its submission for publication.
Funding declaration
The author received no financial support for the research, authorship and/or publication of this article.
Revised: April 2, 2026 AEST