Background
Cleft lip is the most common congenital malformation of the head and neck, affecting one in 700 births.1 Unilateral cleft lip deformity occurs with the failure of fusion of the medial nasal and maxillary prominences during early gestation. The result is an aberrant insertion of the orbicularis oris muscle as well as myriad of changes to the lip and nose construct.2 There is often an association with a cleft palate with the combined treatment requiring multi-disciplinary care that continues into adulthood. The aims of treatment are to attain normal oral occlusion and speech as well as reconstruction of the affected facial units.3
Modern cleft lip surgical technique reflects the evolution of repairs used over many decades. The rotation-advancement principle was first described by Millard.4 Many modifications have since been described, including techniques described by Fisher that emphasise scar placement, in the ideal line of repair as defined by aesthetic subunits, and the importance of pre-planned markings over ‘cut as you go’.5
Regardless of the technique used, upper lip scars are at risk of hypertrophy and widening. The incidence of hypertrophic scaring in cleft lip surgery is 11 per cent in the Caucasian population and up to 36 per cent in the Asian population.6
In an attempt to modulate scar formation, postoperative management typically includes massage with moisturising cream, scar taping and the use of topical silicone. Previous studies have found that topical silicone does not form stable adhesion on small and irregular upper lip areas.7 The implementation of any physical scar treatment in cleft lip repair scars is challenging due to the age of the patients, and the pain and distress associated with lip massage.
As clinicians, we recommend scar massage as it has little clinical downside, gives the parents ownership of the scar and has no financial cost. We all hear anecdotal experience of hypertrophic scars that seem to improve with this intervention, hence a reluctance to discard this recommendation. However, many of us have also experienced a vastly improved scar where parents have admitted to little or no massage. There is no conclusive experimental evidence supporting scar massage in the cleft lip population. Thus, the aim of this study was to measure the effects of postoperative scar massage on the appearance of unilateral cleft lip scars.
Methods
Between May 2009 and August 2011, 33 unilateral complete cleft lip repairs were performed at Royal Children’s Hospital Melbourne by four different surgeons. All patients were fitted with arm splints following the operation. Patient demographics, type of suture material used and technique of repair were recorded. Patients were professionally photographed preoperatively and then postoperatively at approximately three, six, 12, and 24 months by a single photographer.
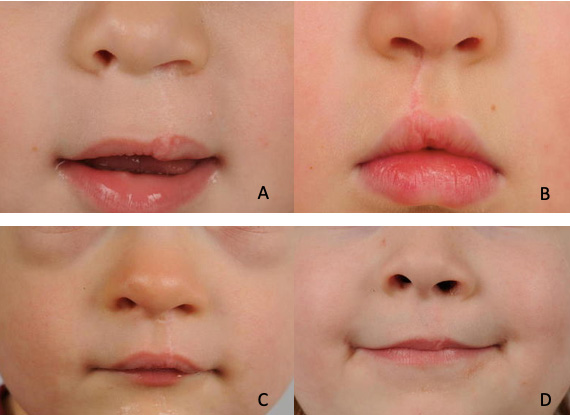
A panel of eight blinded observers comprising four plastic surgeons and four surgical allied health workers were selected to participate. Observers were shown a slideshow containing de-identified photographs of patients 24 months postoperatively, distributed in random order (Figure 1). They were instructed to rate each photo on a scale of one to five based on the quality of the scar alone, with one equal to ‘very poor’, two to ‘poor’, three to ‘good’, four to ‘very good’ and five to ‘excellent’ (see Appendix 1). To standardise the method of ranking, clear written instructions were provided to each member of the panel making clear that the study was solely looking at the appearance of the scar and that the result of the cleft lip repair itself (symmetry, alignment, etc) should not be taken into consideration.
_and_patient.jpg)
Scar massage data was obtained retrospectively via telephone questionnaire. Parents were asked whether lip scar massage was performed ‘every day’ (score of one), ‘sometimes (2–3 times per week)’ (two), or ‘never’ (three). Statistical analysis was conducted using Stata software (version 15; StataCorp LLC 4905 Lakeway Drive, College Station, Texas 77845-4512, USA). Group data was compared with one-way ANOVA. P-values less than 0.05 were considered significant.
Ethics approval was obtained from The Royal Children’s Hospital Melbourne Research Ethics and Governance office with HREC reference number QA/60562/RCHM-2019.
Results
Twenty patients responded to phone questionnaires and formed the study group. All patients had their cleft lip repair between the ages of three and nine months with an average of 5.3 months of age. The most common type of cleft lip repair used was based on Fisher’s technique which comprised of 12 patients, followed by Millard’s technique with seven patients and one patient having an operation based on the technique described by Mohler.8 Eleven patients were treated with absorbable sutures and nine had non-absorbable sutures with removal at a second operation. No postoperative complications such as infection or wound dehiscence were recorded in the cohort.
On questioning, six patients never had any cleft lip massage and formed the ‘no massage group’, seven patients had massage every day (massage group) and seven patients formed the ‘sometimes group’ (performing massage less commonly than every day). Length of time of each massage session and total length of time massaged were not recorded due to the difficulty in recollection and consistency. Qualitative analysis showed that some massage sessions were aborted early due to child distress.
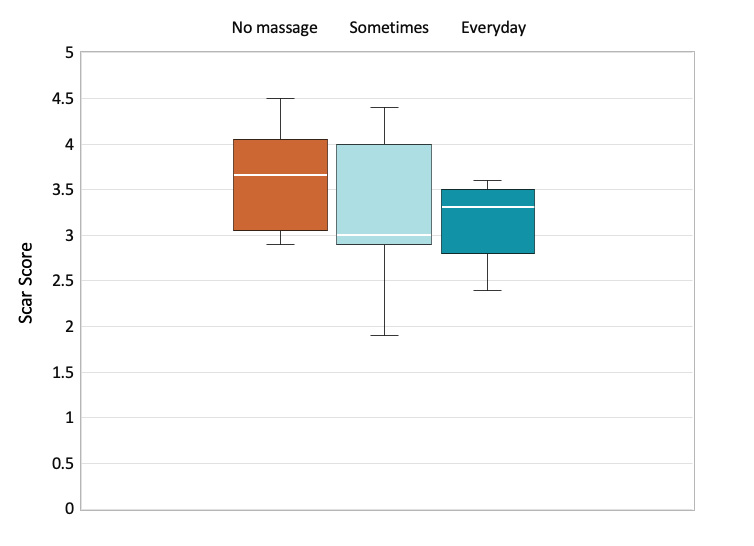
Box plot of scar scores for each group is found in Figure 2. Average scar score for the no massage group was 3.62 (SD ± 0.58), 3.16 (SD ± 0.43) for the massage group and 3.17 (SD ± 0.82) for the sometimes group. On statistical analysis, frequency of scar massage was not associated with a better scar score (p = 0.36). Every day massaging was also not statistically better than no massage (p = 0.41).

Regarding other potential variables affecting cleft lip scar, patients undergoing cleft lip repair with Fisher’s technique had better scar scores than patients undergoing Millard’s repair (p = 0.027). Scar scores were also better when non-absorbable suture material was used (p = 0.0013).
Discussion
Problematic scarring following facial surgery is a challenging complication often causing significant distress.9 Scar forms between the three phases of healing: inflammatory, proliferative and remodelling. The final appearance of a scar depends on the level of cellular activity within each phase and is influenced by multiple genetic and environmental factors.7,9 Exactly how massage modifies the construct of a scar is not completely understood. Shin and colleagues have suggested the application of mechanical force in a scar alters the molecular signalling responsible for the formation of connective tissue growth, which in turn downregulates fibrosis.10 Reno and colleagues suggest that scar massage induces fibroblast apoptosis, thus reducing collagen deposition.11
Shin and colleagues 2012 systematic review showed that scar massage can have significant efficacy, mainly in the treatment of postoperative scars, but little effect was seen in equivalent traumatic scars.10 The authors describe vast inconsistencies regarding treatment protocols, duration of therapy sessions and how outcomes were measured, hence evidence-based recommendations were difficult to make. Cho and colleagues 2014 randomised controlled trial in burn patients showed statistically significant improvement in scar pigmentation and skin elasticity with scar massaging albeit when conducted three times a week by a massage therapist.9 Despite encouraging evidence in other areas, minimal data exists on its use in postoperative cleft lip repair patients. We only found a single case-study regarding the use of massage therapy in a cleft lip scar.12 Other authors have recommended the use of cleft lip massage but no evidence has been documented.13,14
Scar management advice in our institution is usually based on surgeon’s preference, with common options being avoidance of direct sun exposure, scar taping and scar massage. Other options for scar management following cleft lip surgery have been explored in the literature with variable results. Intense pulsed light laser therapy has shown good short-term outcomes but long-term data is lacking.7 Botulinum toxin A has been trialled with a positive effect on cleft lip scar width, however, it did not have any statistically significant change in scar pigmentation, vascularity, pliability or height.15 Long-term data on botulinum toxin A effect on lip scaring is lacking and significant costs and the rare but significant side-effect of oral incontinence is often a barrier for use. One study explored the use of hydrogen peroxide washes, however did not use a control group.14 One author described the use of an ointment comprising of paraffin, tetracycline, petroleum jelly such as Vaseline® and lignocaine combined with a Logan Bow dressing.16 Silicon sheeting and silicone gel have also been explored but without a control group.17
We recognise the presence of confounding factors when assessing the effects massage in cleft lip surgery scars in our study. Surgeons’ experience, surgical technique, suture material, trauma sustained during scar maturation and surgical complications can all play a key role in determining the final look of a scar.6,7,10 Our study found a statistically significant improvement in scar scores when the Fisher’s technique of cleft lip repair was used. The results are in keeping with other evidence previously described by Kwong and colleagues and Mittermiller and colleagues.18,19 Further limitations include the retrospective nature of this study and reliance on parents’ recall. In our experience, massaging the lip was a particularly traumatic experience and parents were quite vivid in their recollections.
It is indeed possible that the positive effect of scar massage seen in other areas of the body is not replicated in our cleft lip cohort due to technical issues with massaging an infant’s lip. Qualitative feedback from the parents in our study certainly support the concept that children may become distressed during massage, and this may result in cessation or shorter therapy duration. Jin and colleagues systematic review identified therapy related factors responsible for early treatment discontinuation in patients.20 Long treatment duration as well as the side effect of pain could have a causative effect on the early cessation of cleft lip massage in our cohort. Furthermore, overcoming the parental instinct caused by a crying child can be challenging. Prolonged exposure to a crying child has the neuroendocrine effect of causing stress and placing demands on a parent to act, in this case, by discontinuing cleft lip scar massage.21
Our study is based on small numbers, however, regardless of surgeon or surgical technique, our evidence shows no correlation between the use of massage and the quality of the scar. Larger studies conducted in a prospective nature will commence at our institution in response to these initial findings.
Future studies will prospectively randomise patients, control for possible confounding factors and use an objective scar assessment scale such as the patient and observer scar assessment scale (POSAS).22
Conclusion
To our knowledge, this is the first study exploring the important subject of postoperative scar massage in the outcomes of unilateral cleft lip repair surgery. Our study did not find conclusive evidence to support the use of scar massage following primary repair of unilateral cleft lip. Our study revealed that many parents and children reported or experienced distress during lip scar massaging, thus warranting further evidence to support its use. Further studies are encouraged among other institutions to support the use of this potentially distressing postoperative intervention.
Acknowledgements
Statistical analysis was performed with support from Dr Vicky Tobin, Peninsula Health, Victoria, Australia.
Prior publication
This article was accepted for verbal presentation at the Annual Scientific Meeting for the Royal Australasian College of Surgeons.
Consent to publish
Patients/guardians signed informed consent regarding publishing their data and photographs.
Disclosure
The authors have no conflicts of interest to disclose.
Financial declaration
The authors received no financial support for the research, authorship, and/or publication of this article.