
Introduction
The number of elective plastic and reconstructive surgery procedures being performed around the world is increasing. According to the American Society of Plastic Surgeons (ASPS), there were 17.7 million surgical and minimally invasive procedures undertaken in the USA in 2018, an overall two percent increase compared with 2017 and a 163 percent increase from the year 2000.1 Surgery can enhance self-esteem, body image perception and ultimately quality of life in mentally healthy surgical candidates.2 However, patients seeking surgery to alter a particular part or region of their body can be motivated by a high level of negative body image perception. This was reported by Sarwer and colleagues who found that these patients also had an increased rate of underlying psychiatric disorders including body dysmorphic disorder (BDD) and eating disorders.3 Identification of patients with a psychiatric illness, and those who may have undiagnosed BDD in particular, is critical for plastic surgeons, as operating on these patients can present a number of risks both to the surgeon and the patient.
Patients with some types of mental illness can have unrealistic expectations of what can be achieved and dissatisfaction with their surgical outcomes, despite objectively good surgical outcomes. This can in turn lead to deterioration of the mental state of the patient, with increasing anxiety, low self-esteem, depression and even suicide in patients with BDD.4,5 For the surgeon, operating on these patients while unaware of their mental illness can put them at risk of legal action or interpersonal violence. Sweis and colleagues reported that two percent of plastic surgeons had been physically threatened by patients and 10 per cent had received threats of violence and legal action from patients who were unhappy with their surgical results.6 At least two patients with suspected BDD have been involved in the homicide of their treating plastic surgeon.6 Most elective plastic surgery procedures, including those done for predominantly functional or even oncological reasons, affect appearance, so plastic surgeons working in non-cosmetic environments still need to be aware of mental illnesses that impact body image.7
The reported rate of psychiatric illness among patients seeking plastic surgery is varied. Often the reported rates do not distinguish between plastic and reconstructive surgery and cosmetic surgery. One report by Hayashi and colleagues found that between 30 to 70 per cent of patients seeking plastic and cosmetic surgery had a psychiatric diagnosis.8 However, Sarwer and colleagues reported a much lower rate of 7 per cent for patients seeking plastic surgery and 16 per cent for patients seeking cosmetic surgery.9,10 Although there are publications on the prevalence of psychiatric illness in surgical candidates8 there is little in the literature on the progress of these patients through a surgical unit and their management using a model where referral to psychiatry is surgeon-driven and where there is a joint psychiatric/surgical approach.
Brunton and colleagues have looked at the evidence for psychological and psychiatric predictors and outcomes for ‘cosmetic surgery’ but found that the literature was too heterogenous to draw firm conclusions.4 Interestingly, they included breast reduction surgery as a cosmetic procedure whereas it has now been clearly demonstrated to be a functional procedure for pain relief.11 They emphasised the potential role for screening questionnaires and patient reported outcomes measures for improving knowledge in this field.
Hayashi’s prospective cohort study of predominantly facial cosmetic surgery found that 32 per cent of patients who met their initial screening criteria were diagnosed with a psychiatric disorder and 18 per cent had BDD.8 They highlight the role of a formal psychiatric screening interview and also found that in some cases the request for cosmetic surgery seemed to be the first manifestation of serious mental illnesses such as schizophrenia. They also point out that a diagnosis of mental illness is not necessarily a contraindication for surgery but that combined care of patients between psychiatry and surgery is beneficial.
The distinction between elective plastic surgery to treat a functional problem such as abdominoplasty for an abdominal apron that is causing rashes and purely cosmetic surgery may be important in this field. A study by Javo and colleagues in Norway found that women seeking abdominoplasty were likely to be less psychologically complex and have fewer body image concerns than those seeking liposuction, rhinoplasty or breast augmentation, suggesting that ‘abdominoplasty surgery is more often sought for functional reasons.’12 A Finnish study of 64 women undergoing abdominoplasty found significant levels of preoperative psychopathology but found that there was an improvement in mental health following surgery.13
Although not the most common psychiatric diagnosis in the cohort of this study, BDD is of particular interest due to its potential for devastating impact to both patient and surgeon if the surgical journey is embarked upon without full knowledge of the condition.
This study sought to understand the psychiatric and surgical outcomes of patients that were deemed by their plastic surgeon as requiring a psychiatric assessment in the context of their evaluation for elective plastic surgery in a public hospital, with the rationale that this evaluation could assist in delivering better services as well as reducing risk to the patient.
Methods
This is a retrospective cohort study. All patients requesting elective plastic surgery who had an initial consultation with one consultant plastic surgeon and were referred to a consultant liaison psychiatrist for preoperative psychiatric evaluation between June 2010 and June 2016 at Flinders Medical Centre in South Australia were eligible for inclusion. In the public hospital system in Australia, ‘elective’ means planned surgery (as opposed to emergency surgery) but does not include purely cosmetic surgery. It is mandated by the state health departments that the patient must have a physical pathology or functional problem to be eligible for elective surgery.14 There were no selection criteria around types of presentation, meaning patients with a wide variety of primary pathologies were eligible as well as those with problems secondary to previous trauma or surgery. Referral letters to and from the plastic surgeon and the psychiatrist were reviewed for each patient and details relating to psychiatric diagnosis and recommendations around surgery were recorded. Those who were diagnosed with BDD had a more detailed analysis of their treatment course. Their medical records were reviewed to determine if all of the psychiatric recommendations were followed and to determine if these patients had gone on to have surgery. Psychiatric disorders diagnosed by the psychiatrist were grouped as: major depressive disorders (MDD), post-traumatic stress disorder (PTSD), eating disorders (ED), BDD and other.
To aid communication with the psychiatrist, the referring plastic surgeon assigned patient’s physical indication for surgery as ‘good’, ‘moderate’ or ‘no physical indication’. Patients assigned a good indication were referred for psychiatric assessment when the surgeon felt that adjunctive therapy may assist them in coping with their physical changes. Patients assigned a moderate indication had some physical grounds for surgery but the surgeon felt that there may be other non-physical reasons for requesting surgery. Where the surgeon could not identify any physical need for the surgery and was concerned that there may be a body image disorder driving the request, patients were assigned no physical indication for surgery. These ratings were recorded, as well as the psychiatrist’s recommendation for psychiatric treatment, prior to or following surgery. Details were recorded as to whether the desired surgery went ahead as well as if the psychiatric evaluation was pre- or post-surgery. Attendance at the arranged psychiatric consultation, and compliance with recommended psychiatric treatment, were reviewed.
Results
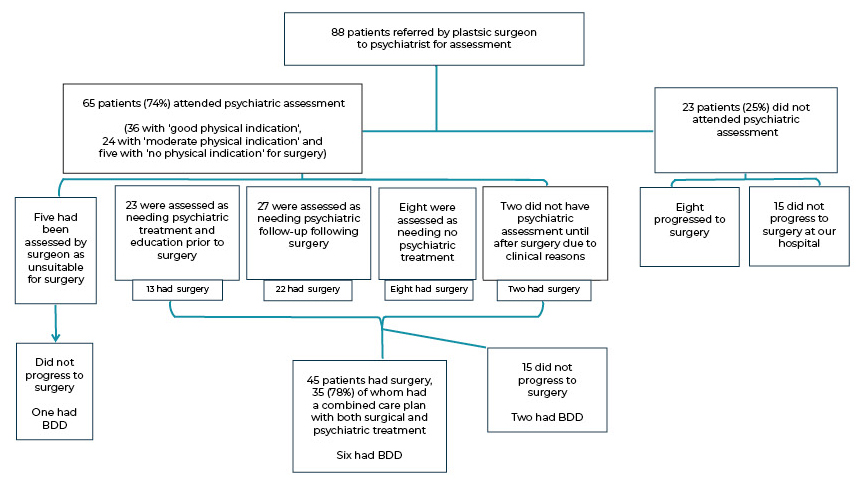
Between June 2010 and June 2016, 88 patients were referred by their plastic surgeon for psychiatric assessment prior to being considered for surgery. These patients were predominately female (87.5%) and between 20 and 50 years of age (77.3%). Of the 65 (73.9%) patients who attended their psychiatric evaluation, 54 (83.1%) were given a diagnosis of a mental illness. Age, sex, type of surgery requested and psychiatric diagnoses are shown in Table 1.
The numbers of patients referred to psychiatry and their management in the model of care is shown in Figure 1. The majority (45/60, 75%) of the patients deemed to have a good or moderate physical indication for surgery went on to have the planned surgery. Many of these patients had a diagnosed mental illness and supplemented their surgery with adjunct psychiatric treatments.

Nine of the patients reviewed by the psychiatrist were diagnosed with BDD (13.8%). The types of surgeries being requested by these patients included abdominoplasty, breast augmentation and reduction, fat transfer, scar revision, mons pubis reduction, augmentation of shoulders and eyelid surgery. Of the patients diagnosed with BDD, most were considered to have a good or moderate physical indication for surgery. However, psychiatric care during the surgical journey was recommended in each situation. One patient had their BDD diagnosis made after their initial surgery (for cancer) was completed but, on review by the psychiatrist, was considered a good candidate and went on to have more surgery after the study period. Figure 2 shows the surgical journey of one patient with BDD who initially presented with scarring following a traumatic facial injury and went on to have a number of corrective surgeries, as shown. She received cognitive behavioural therapy (CBT) throughout this surgical period that helped her to manage her expectations and was happy with her long-term outcome.

Of the nine patients with BDD, six went on to have surgery. Four of these continued to receive psychiatric treatment after surgery. None of the nine patients with BDD refused psychiatric assessment or treatment. Of the three patients who did not undergo surgery, each received CBT instead of surgery. Each achieved a good outcome and did not present to the plastic surgery unit again.
Discussion
This retrospective review of a model of care where there is surgeon-driven psychiatric assessment of elective plastic surgery candidates has shown that the majority of patients referred for assessment prior to surgery were diagnosed with a mental illness that required some form of management before or after surgery, and in a number of cases, both. This indicates that surgeons can be effective at identifying vulnerable patients with respect to mental illness. Appropriate psychiatric assessment and diagnosis allows diversion of unsuitable patients away from surgery and allows those who require psychiatric treatment to receive it in parallel to surgical care. This process shows that where the physical indications for surgery are good, most patients are able to proceed with their requested procedure.
Rates of BDD have been reported in the general population between 0.7–2.4 per cent.15 However, for candidates seeking cosmetic surgery, the reported prevalence rates for BDD have a much wider range of between 2.9 and 53.6 per cent.15,16 Differences in sample size, patient selection criteria and methodology can account for much of this range. Our finding of a rate of 10.2 per cent of patients referred for psychiatric evaluation is within the range of these previous studies, however, in patients who were reviewed by our psychiatrist, the rate of BDD increased to 16.7 per cent. The majority (71–76%) of patients with BDD will primarily seek non-psychiatric medical treatments rather than psychiatric care which is concerning given the number of studies that suggest that these patients require psychiatric treatment rather than, or alongside, medical treatment, including surgery.5,17–23 Our study supports other evidence that an integrated approach between surgical and psychiatric doctors can avoid the previously documented catastrophic outcomes of BDD patients presenting to surgeons.7
The majority of patients in this study exhibited degrees of body image dissatisfaction. The definition of BDD, however, requires that the patient exhibit a number of behaviours that are repetitive and clinically significant as well as behaviours that are not better explained by an eating disorder.24 Most of the patients in this study did not meet the specific criteria required for a diagnosis of BDD. However, nearly one fifth of patients had a diagnosed eating disorder, indicating a strong degree of body dissatisfaction. When combined with the patients diagnosed with BDD, they accounted for nearly one third of the total group reviewed by our psychiatrist.
Other psychopathology such as anxiety and depression can also create significant dissatisfaction with physical appearance. In elective plastic surgery candidates, the reported rates of major depressive disorder are seven times higher, and anxiety disorders 1.7 times higher, compared to the general population of the USA.25–27 In this study we found rates of major depression and eating disorders similar to previous studies.
We found that the level of compliance with attending psychiatric assessment and with psychiatric treatment was high. This should reassure surgeons that they can refer patient to a psychiatrist without fear of causing harm to the doctor/patient relationship; most patients are accepting of the referral especially if it is couched in terms of recognising that they are distressed and that the referral is to help them with this distress.
Is BDD an absolute contra-indication for surgery? Not necessarily. Higgins and colleagues discussed the potential for BDD to be categorised into levels of severity and that the different levels had different indications for, and degrees of, satisfaction with surgery.28 Supporting this, Felix and colleagues reported that 81 per cent of patients with mild-moderate BDD had full remission of their symptoms after surgery and that 90 per cent reported that they were satisfied with their surgical outcome.29 Patients with severe BDD, however, show greater levels of impairment in their overall functioning. They have significant difficulties in their capacity to work, in their social life and intimate relationships. They often have delusional beliefs about their appearance and are more prone to compulsive behaviours like checking their appearance in a mirror, excessive grooming and skin picking.24 Careful management of these patients is needed to ensure they receive efficacious care.
The use of a screening tool that enables clinicians to categorise patients into various severity levels of mental illness would help ensure that surgery is available to all patients who would most benefit from it. It would also help direct patients in need of psychological treatment to be seen and cared for appropriately. There are a number of questionnaire-type tools available.30–32 As these tools vary in length and complexity, their application would largely depend on the amount of time available to complete them.
For patients with BDD or psychopathology involving severe dissatisfaction with physical appearance, Sarwer and colleagues found that surgery to enhance this rarely results in an improvement in their psychological symptoms.18 Patients with severe BDD have higher rates of suicide and there are documented incidents involving threats of violence, and even homicide, directly relating to the health care providers.6 This makes it particularly important to ensure that surgical services are identifying patients with BDD and helping them obtain appropriate psychiatric treatment, rather than just offering surgery.
This retrospective study has some limitations: only a select subset of all patients seeking elective plastic surgery in one Australian public hospital were included and only one main plastic surgeon was involved. Our results likely underestimate the real number of patients that would benefit from psychiatric input during their surgical journey and without assessing the whole cohort, we do not know how many patients were missed (false negatives). Unfortunately this was beyond the scope of the study. There were no standardised criteria for referrals to psychiatry. It is not standard practice for patients requesting elective plastic or reconstructive surgery to be reviewed by a psychiatrist before being considered for surgery in our institution. Indication for surgery was determined by the consulting plastic surgeon based on their clinical experience and judgement. Follow-up on the course of management was limited to information that could be found on the electronic hospital database. It was difficult to determine if patients had sought surgery or psychiatric treatment from providers outside the hospital unless this information was volunteered by the patient.
Conclusion
This model of care, where the plastic surgeon drives psychiatric evaluation of patients they are concerned about, resulted in an 83 per cent positivity rate in terms of a psychiatric disorder being present. The identification of patients with serious psychiatric illness facilitated appropriate treatment of their mental illness as an adjunct to indicated surgery in many patients. In patients with BDD this model of care led to diversion of one third of patients away from surgery, with successful treatment with CBT and to successful combined surgical/psychiatric treatment in a further six, who had a clear physical need for surgery. This model of care appears safe and effective for the management of elective plastic surgery patients in a public hospital setting, but could potentially be further improved by supplementation with a formal psychiatric screening test.
Consent to publish
Patients signed informed consent regarding publishing their data and photographs.
Disclosure
The authors have no conflicts of interest to disclose.
Financial declaration
The authors received no financial support for the research, authorship, and/or publication of this article.