
Dear Editors,
I was interested to read the perspective in the History section of this journal by Richard Hamilton and Ingemar Fogdestam ‘Australia’s contribution to the free abdominoplasty flap in breast reconstruction’.1 Perhaps few realise that the development of what became known as the free transverse rectus abdominis myocutaneous (TRAM) flap was a race involving not one but two surgical teams, one in Sydney and the other, with the aid of the Australian Richard Hamilton, in Sweden. It reminded me in a very small way of the race to characterise the structure of DNA, which was won by Watson and Crick. Then, in the early 1950s, several teams were working on both sides of the Atlantic to elucidate the structure and the race was very close.
I returned to Australia from the United Kingdom in late 1978 and in January 1979 joined the Plastic Surgery Department of Prince of Wales (POW) Hospital in Randwick, Sydney, as the Microsurgery Registrar. In those days the position was more like that of a Senior Registrar/Research Fellow. On the first day of my taking up the position, the Unit Head, Tony Pelly, asked me what my research interests were. I replied “Free flaps, Sir…in particular, a vascularised free sural nerve graft, possibly with overlying skin as a monitor”. I had been aware of the work of Taylor and Ham in that area,2 but felt there were some unexplored options. Pelly in his usual hyper-enthusiastic way, conducted me on a whirlwind tour of all departments that could assist this research, including the Radiology Department, where I would carry out injection studies of the superficial sural artery, a likely contender for a vascularised sural nerve graft.
Research began immediately, combined with a busy microsurgical load. Virtually all replants in New South Wales were done at POW, and there was a regular diet of free flap repairs, namely groin flaps and tensor fascia lata free flaps. To this was added the usual gamut of plastic surgery in a big teaching hospital. After determining that the superficial sural artery did indeed supply blood to the whole length of the sural nerve, we performed a free superficial sural artery flap of skin containing the sural nerve in the first half of 1979. Unfortunately, the artery was only about 0.8 mm in diameter and the flap did not survive.
Pelly immediately switched my research attention to the use of abdominal tissue as a free flap. Like the Swedish team, we were aware of the two possible blood supplies: from either the superficial epigastric system, which had been researched by Dr Bernard O’Brien’s Unit as early as 1972, or the deep inferior epigastric system, researched by Brown, Vasconez and Jurkiewicz in 1975.3 It was decided that I should perform a couple of cadaver studies to determine that there were significant perforators coursing through the rectus muscle to supply skin and fat from potentially a wide area of the lower abdomen (Figure 1a).

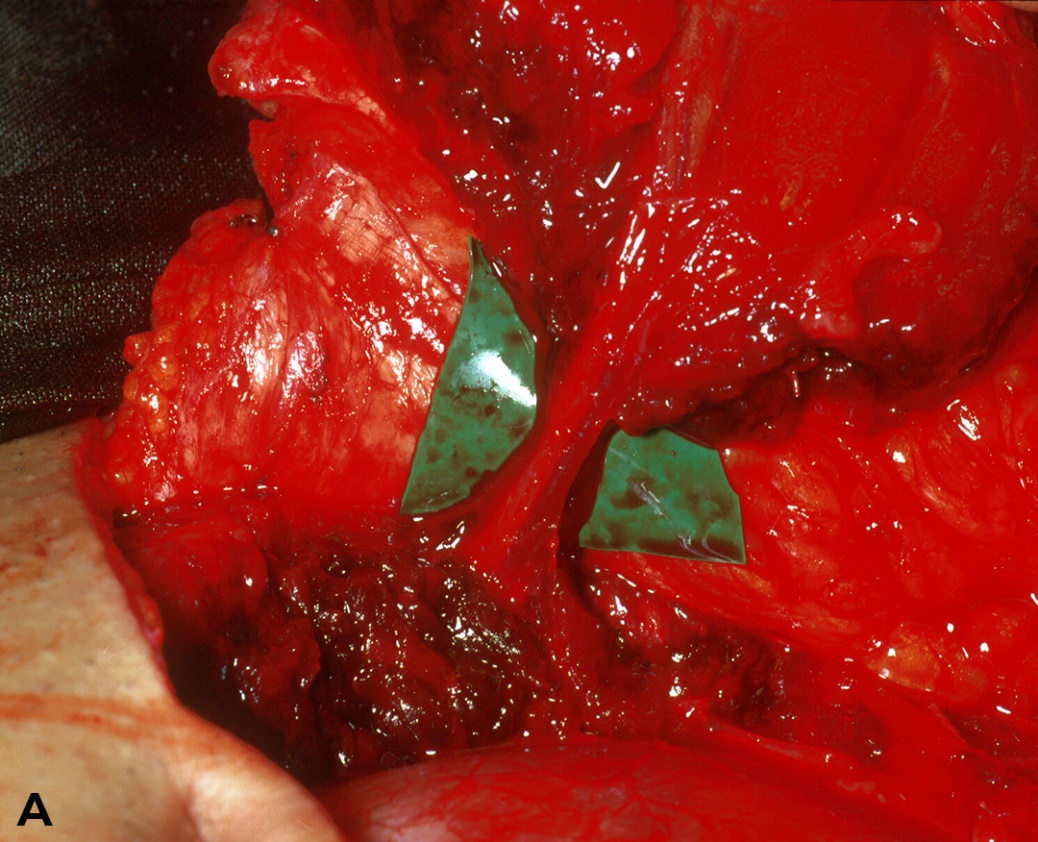
Restless as he was, Pelly persuaded a patient who was to undergo an abdominoplasty to allow us to inject the deep inferior system with a blue dye to determine the extent of perfusion while on the operating table. The patient’s entire mid and lower abdominal skin promptly went blue-green. Of course, most of this was removed by the abdominoplasty. As the dye suffused through the vascular system, the anaesthetist became somewhat alarmed by the patient’s bluish colour, which persisted for a couple of days postoperatively!
Shortly after, a male patient was found who had suffered deep scarring and unstable skin, with a significant contour defect over the clavicular region, the result of an old shotgun injury (Figure 1b). We performed Australia’s first free TRAM flap reconstruction of this defect, anastomosing the deep inferior epigastric vessels (Figure 1c). This was later published in 1980.4 At the time, I believed it was a world first, but soon discovered we had been ‘pipped at the post’ by Johanson’s team in Sweden, ably assisted by Richard Hamilton, hence the Australian connection.
_unstable_scar_and_contour_defect_of_right_clavicular_region_-mid_1979__and_(c)_ear.png)
Thanks to the pioneering work of Bernie O’Brien5 and Ian Taylor, Australia had had a jump on the rest of the world with a number of ‘world firsts’ to our credit. This included the world’s first free flap in 1973,6 the first scalp replant in 1976,7 and the first ear replant in 1979.8
The free TRAM flap became a standard method of breast reconstruction for many years, still in use in many places, although somewhat bettered by the DIEP flap. Despite Johanson’s use of the term ‘abdominoplasty flap’, the flap became widely known as the TRAM flap. Indeed, as noted by Hamilton, the TRAM was not used as a pedicled flap until two years after its first use as a free flap, most unusual in the normal course of flap design.
Published: March 31, 2021 AEST