Introduction
Mallet fractures are caused by avulsion of the extensor tendon from the distal phalanx and may be associated with distal interphalangeal (DIP) joint subluxation. Treatment aims to improve the early clinical outcome and prevent long-term arthritis, deformity and pain. Maintenance of range of motion (ROM), strength and function, with absence of deformity or complication, is key to patient wellbeing.
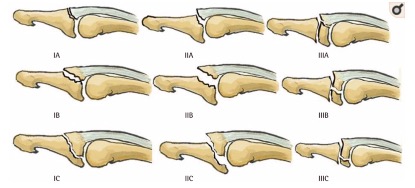
Mallet fractures range in severity from small, minimally displaced avulsions with enlocated joints to large, displaced fracture fragments with associated joint subluxation.1,2 The Wehbé and Schneider classification for bony mallet injuries assigns a number to reflect joint subluxation and a letter to reflect the percentage of joint surface involved (Figure 1).3,4

Various surgical techniques have been described in mallet fracture treatment. Frequently a trans-DIP joint Kirschner (K) wire is employed. Ishiguro first described the closed extension block pinning technique, which adds a second blocking K-wire, a technique modified by other authors since.5,6 Alternatively Kronlage, Teoh and Theivendran have all illustrated open reduction and internal fixation with screws or a plate.7–9
Currently, published evidence does not clearly define the role of surgery in managing mallet fractures. Handoll and colleagues attempted a Cochrane review in 2004 to assess the efficacy of different treatment methods. They concluded that many studies were methodologically flawed, due to inadequate outcome assessment. As a result, only four studies were included, all published prior to 1993, and only one compared surgery and splinting.2,4,10
There is no universal measure of a successful outcome for mallet fracture treatment.4 The most frequent outcomes reported are joint enlocation or Crawford’s criteria.2,4,11,12 Using joint enlocation alone lacks patient focus and using Crawford’s criteria lacks reproducibility, defining a poor outcome as extensor lag > 25 degrees and persistent pain, without detailing how pain was assessed. We have combined these into a defined and reproducible outcome measure.
The purpose of this study is to provide a patient-focused, multifaceted assessment of surgical and non-surgical treatment of acute mallet fractures. We compare continuous external splinting, primary surgical intervention plus splinting and delayed surgery which follows a failed attempt at splinting. We aim to answer the question: Is splinting or surgery the best treatment for acute mallet fractures?
Methods
Between June 2012 and June 2015, adult patients presenting with mallet fractures, in Auckland and Counties Manukau District Health board regions of New Zealand, were identified by their treating clinician and referred to our research team. A written consent process was undertaken. Table 1 details inclusion and exclusion criteria. Weekly review of discharge coding minimised missing potential participants.
The research team prospectively populated a database using clinical records and radiographs, becoming involved in patient assessment only after three months. At enrolment, the first author reviewed the best available, splint-free lateral radiograph, and the injury was classified according to Wehbé and Schneider classification.
The study was observational. Enrolment did not alter the patient’s treatment. We measured patient experience and outcomes over time, following initiation of either surgery or splinting. We did not analyse the clinical decision-making process.
The splinting protocol involved maintenance of continuous DIP joint extension for six to eight weeks using a custom-made thermoplastic splint. Daytime splint weaning with night splinting until 12 weeks followed this. Surgically fixed fractures were splinted for six to eight weeks postoperatively with a similar weaning program.
Surgical technique for each fracture was selected by the surgeon as most appropriate for the fracture characteristics. These are detailed below.
Clinical and patient-reported outcomes were collected by the research team and recorded in a standardised manner. Early assessment was performed three months post treatment initiation and late assessment at six to 12 months. Patients were deemed lost to follow-up if at 273 days (nine months) post initiation of treatment they had failed to attend any research follow-up appointments.
Overall treatment success was defined as achieving a minimum standard in three key outcomes, as noted below. The criteria for success were chosen using a consensus of the research group to be patient-focused, reproducible and aligned with previous literature:
-
DIP joint not subluxed
-
< 25 degree extension deficit at the DIP joint
-
< 20/50 pain score using the Patient-Rated Wrist/Hand Evaluation (PRWHE) pain assessment.
Secondary outcomes included isolated assessments of subluxation, pain score, extension deficit, flexion deficit, and functional disability. Range of motion was assessed using a dorsally placed hand-held goniometer. An illustrated protocol promoted consistent measurements between researchers.
Patients completed validated patient-rated outcome questionnaires at each of their research appointments, these being the Quick Dash (Q-DASH), PRWHE and Patient Evaluation Measure (PEM) parts II and III. We used the PRWHE to assess pain. It is multidimensional and easily reproducible, assessing pain frequency, severity and timing over five questions to give a score out of 50.
Outcomes were analysed according to treatment received in three treatment cohorts—continuous external splinting (splinting cohort), primary surgical intervention plus splinting (surgery cohort) and delayed surgery, which followed an attempt at splinting (delayed surgery cohort). For inclusion in the outcomes analysis, patients required a lateral radiograph taken at least 70 days after surgery. Where multiple radiographs had been taken, the most recent was used to grade outcome. The first author reviewed the final radiograph for each patient and recorded DIP joint subluxation in a dichotomous manner—subluxed or non-subluxed. Patients had no additional radiation exposure for the study.
Biostatisticians performed comprehensive statistical analysis of primary and secondary outcomes including subgroup analysis for injury types IB and IIB. Kaplan-Meier estimates of overall success (primary outcome) and subluxation outcome at different follow-up times were reported for the different treatment groups. Cox regression was applied to compare risk of failure between the three groups. All potential confounders were assessed in separated regression models. Confounders with p < 0.25 in the univariate results were selected for the final model. Hazard ratios with 95 per cent confidence intervals are reported. Quantile regression was used to compare the distribution of pain score and Q-DASH score at early and late follow-up between the three groups and adjusted for confounding factors.
The study was registered with our local research facility and ethical approval was granted by the New Zealand Northern B Health and Disability Ethics Committee Health and Disability Ethics Committee (HDEC) #13/NTB/202.
Results
Between June 2012 and June 2015, 109 patients with 113 mallet fractures were enrolled in the study. Of these 109 patients, 24 failed to attend any research appointments within 273 days (nine months) of treatment initiation so were deemed ‘lost to follow-up’ and excluded from analysis. Thus 85 patients with 89 mallet fractures completed the study (Table 2).
Patients in the surgery cohort were significantly younger than those in the splinting cohort, mean ages 33 (SD = 13) and 42 (SD = 16) years, respectively.
The median time from injury to presentation was three days (0–38). Splinting was most frequently initiated on the day of presentation, median 0 days
(0–34). Surgery was performed a median of 5.5 days post presentation (0–41).
Follow-up timescale
Research-specific clinical follow-up occurred twice: early follow-up at a median 91 days (63–186) post treatment initiation and late follow-up at a median 190 days (95–354). The final X-ray was taken a median 160 days post treatment initiation (range 73–335 days).
Treatment groups
Of the 89 fractures included, 55 were initially managed with splinting and 34 were initially managed surgically with postoperative splinting (surgical cohort). Of the splinting cohort, nine (16%) failed splinting and required surgery within six weeks of treatment initiation; these patients were subsequently analysed in a separate delayed surgery group (Table 2).
Surgical technique
The operative techniques used included 15 open reduction and single-screw fixation, 10 K-wire and single screw, eight closed reduction with two K-wires (Ishiguro or modification of Ishiguro technique), five open reduction and multiple screws and four ‘other’ (hook plate/tension band wire).
Injury classification
Of the 89 fractures, 77 (87%) were Wehbé and Schneider subtype B (fragment size between one and two thirds of the joint surface), 40 (45%) were type IB (without subluxation) and 37 (42%) were associated with type IIB (with subluxation). These two groups were large enough for subgroup analysis. Significantly more type IIB injuries were treated surgically than with splinting alone (28/40) (Table 2). The splinted group comprised 46 patients—eight type IA fractures, 27 type IB, two type IIA and nine type IIB.
Of the 10 IIB fractures initially managed with splinting, one was operated on at three weeks to reduce the subluxation (moved to the delayed surgery group), two presented late and another was deemed unfit for surgery, so subluxation was accepted. Of the remaining six, five were reduced and maintained enlocation with a customised splint. The sixth was pain free with DIP joint ROM 0/65 so the result was accepted.
Nine fractures (in nine patients) underwent delayed surgery following a period of splinting alone. Of these eight were initially classified as IB fractures, but subluxed after commencing splinting, and one was IIB (mentioned above) but a trial of splinting failed to maintain reduction.
Overall success
Overall treatment success was defined as achieving a minimum standard in three key outcomes (joint enlocation, pain score and extensor lag). Of the 89 fractures, four fractures in three patients had insufficient data for assessment of all criteria—two lacked radiographs at > 70 days post injury and two failed to complete pain score questionnaires.
When all injury grades were combined, no significant differences in success were seen between treatments—80 per cent success for splinted versus 85.7 per cent for surgical patients (hazard ratio 7.88, CI 2.14–29; p = 0.09 [adjusted for confounders]).
Primary outcome analysis
Type IB (without subluxation, moderate fragment)
No significant difference in final overall treatment success was seen between the splinting and surgery groups for IB fractures (hazard ratio 0.91, CI 0.10–8.28; p = 0.93).
Type IIB (subluxed, moderate fragment)
Type IIB injuries treated with splinting alone were five times more likely to fail to meet our minimum criteria for success than those in the surgery group (hazard ratio 5.04, CI 1.24–20.5; p = 0.03).
Secondary outcome analysis
Type IB (without subluxation, moderate fragment)
Of the 40 IB fractures, 35 were initially splinted and five were operated on. No surgically managed fingers subluxed following treatment (0/5). Of those IB fractures managed with splinting, 37 per cent (13/35) subluxed during treatment. Eight of these were re-allocated to the delayed surgery cohort. The remaining five either were not detected or the decision was made to continue splinting.
Type IIB (subluxed, moderate fragment)
Of the 37 IIB fractures, 27 were operated on from the outset and 10 were initially managed with splinting. Of those surgically managed, 20 were without subluxation on final radiograph (20/27), six subluxed and one failed to complete the final radiograph. Of the 10 splinted, one was operated on within the first week of splinting and this was without subluxation at six months. Five of the nine that continued splinting were without subluxation on final radiograph. Kaplan-Meier estimates were used to account for the different follow-up dates and revealed that the likelihood of a joint being without subluxation at six months with splinting versus surgery was 52 per cent versus 80 per cent (p = 0.11, log rank test).
Predicting subluxation
The size of the fracture fragment is correlated to the risk of subluxation, with larger fragments more likely to sublux. In those that did not sublux at any point, the fracture fragment occupied a mean of 42 per cent of the joint surface (SD = 12.7) compared with a mean of 48 per cent in those that did sublux during treatment (SD = 9.1, p = 0.02). Fractures occupying over 46 per cent of the joint surface have a significantly increased chance of subluxation compared with those occupying less than 46 per cent (67% versus 42%). Every one per cent increase in fracture fragment size increases the risk of subluxation by five per cent (OR 1.054 (1.01, 1.10)). Despite enlocation at presentation, when a grade 1B fracture fragment reaches 43 per cent of the joint surface, the fracture has a 50 per cent chance of subluxation.
Pain score (PRWHE pain assessment)
There was no significant difference in pain scores between the splinting and surgery groups at late follow-up (median score 6, IQR 1–13 and 12, IQR 4–18, respectively)
Range of motion
Mean extension deficit was 9.53 degrees (SD = 9.5) in the splinted fractures and 10.9 degrees (SD 12.2) in surgically managed fractures. The difference was not significant. An apparent difference of mean flexion deficit between the splinting group (13.4°, SD = 19.2) and the surgery group (26.1°, SD = 12.9) did not reach statistical significance when adjusted for covariates in injury type, follow-up time and delay in treatment.
Quick-DASH scores
There was no significant difference in subjective functional outcome between the splinting and surgery groups or in subgroup injury grade analyses when measured with Q-DASH. Quick-DASH scores remained stable at early and late follow-up. At late follow-up, the splinting group Q-DASH mean score was 6.8 (SD = 8.96) and for the surgery group it was 13.6 (SD = 13.5). These scores suggest that patients in both treatment groups achieved normal mean
Q-DASH subjective function scores.13
Satisfaction
With all injury grades combined, significantly lower PEM2 satisfaction scores were found in the surgery group at six months (median 79%; IQR: 59.1, 89.4) compared with the splinting group (median 91%; IQR: 82.6, 98.5), with a median difference in score of 11 per cent (1.18, 21.1, p = 0.029). A higher PEM2 score means a more satisfied patient. When injury grades were analysed separately, no significant differences were noted between the treatment groups.
Complications
Surgery had a high rate of complications, especially in the delayed surgery group. In fractures that failed initial splinting. Infection was frequent, occurring in 3/9 (33%) fractures. Failed fracture reduction occurred in 2/9 fractures (22%) (Table 3).
Discussion
Historically the treatment of mallet fractures has been conservative. A recent systematic review of 44 studies included just five comparing surgical interventions with splinting in acute mallet injuries, four of which were published prior to Handoll and colleagues 2004 Cochrane review10 and in total included only 90 mallet fractures.10,12 Current management is based on 40-year-old research, with the tendency to avoid surgery. A survey conducted in the United Kingdom in 2017 reported that 88 per cent of bony mallet injuries are being managed conservatively.14
This current study is unique. To the authors’ knowledge, it is the largest published prospective, comparative study of mallet fractures. In line with the Handoll and colleagues recommendations, defined and reproducible outcome assessments have been used, complications reported and thorough statistical analysis conducted. One of the strengths of this study is that it includes patients treated in hospitals and hand therapy practices in our region. We did not alter treatment or question the rationale of initiating certain treatments. This methodology highlights variation in practices and shows that rules which percolate surgical communities do not dictate all practices. We observed 10 IIB fractures that commenced splinting and six grade I fractures that were operated on from the outset.
We acknowledge that we did not find a significant difference in overall success between the splinting and surgery groups, which would align with existing literature. However, the surgery group consisted of more complex and unstable fracture patterns. Subgroup analysis showed that patients with type IIB fractures managed with splinting alone have a five times greater risk of treatment failure (hazard ratio 5.04, CI 1.24–20.5) compared with surgery. There is a higher likelihood that their joint will remain subluxed but the consequences of this long term are unknown.
As with any surgical intervention, the risks and potential benefits must be weighed up against the individual patient’s goals and comorbidities. While surgery may be advantageous in certain subgroups for certain outcome measures it leads to significantly lower satisfaction when all injury grades are analysed together. This may reflect worse fracture severity in the surgery group. No difference in satisfaction (PEM2) score was seen analysing the injury grades separately.
This study highlights the risk of subluxation in fractures initially presenting enlocated—37 per cent of the IB fractures in this study subluxed. Once the fragment exceeded 46 per cent of the joint surface, subluxation during treatment was significantly more likely (67% versus 42%). If not detected and corrected, that fracture will fail to meet our minimum standard of success. Surgery could be considered at an early stage. If splinting is commenced, we advocate early detection of subluxation as delayed surgery appears to be associated with more complications. We subscribe to Crawford’s recommendation to attain a lateral radiograph of the joint once in the splint, then weekly for the first three weeks.11
Although not statistically significant, surgery was associated with a high complication rate, especially in the delayed surgery group. These findings were not dissimilar to previous studies led by Wehbé, Kang and Yoon.4,15,16
We acknowledge limitations with our research. This is a non-randomised observational study and the surgical techniques used were heterogeneous—a reflection of the number of surgeons involved. This limits recommendations for specific surgical techniques. We achieved a median follow-up time of 190 days (six months) but it is the senior author’s opinion that further symptomatic improvement would occur beyond six months.
We believe that in certain fractures, with a large fragment and early subluxation, surgery must be considered and offers a significantly greater chance of treatment success than splinting alone.
Conclusion
In the treatment of bony mallet fractures, we strive for DIP joint enlocation, maintained range of motion and a pain-free outcome. Type IIB fractures are significantly less likely to meet our minimum standard of success with splinting alone and surgery is recommended. Type IB fractures can be treated successfully by splinting alone; however, this study highlights the significantly increased risk of subluxation as the fracture fragment size increases.
This is the largest recent comparison study for the treatment of bony mallet fractures and provides thorough, reproducible, patient-focused outcome measures. Our results provide guidance for surgeons who strive for joint enlocation, highlighting which fractures are likely to fail and providing clinicians with data to compare their own outcomes against.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
This work was supported by the Sir William and Lois Manchester Trust. Reduced radiology costs were offered by our local imaging providers Auckland Radiology Group, Mercy Radiology, The Radiology Group and Horizon Radiology.
Acknowledgements
The authors wish to acknowledge Irene Zeng, and Christin Coomarasamy, biostatisticians, for their invaluable assistance with this project.
Revised: September 17, 2020 AEST