
Introduction
Lighted retractors are used in a wide variety of surgical fields. They allow illumination of surgical fields that would otherwise require more extensive access incisions and dissection. Their use enhances patient outcomes and recovery from surgery by reducing scar burden, pain and surgical errors caused by poor visualisation. In aesthetic and reconstructive breast surgery the most common type of lighted retractor is the Tebbetts retractor with fibre optic illumination. However, both anecdotally and in the literature, a recurring issue has occurred with fibre optic illumination—latrogenic burn injury. The heat generated at the tip of the optical cable at its connection to the retractor may cause a thermal injury if it comes into contact with the patient, either directly or through the drapes. Prompted by a recent case in our unit we sought to confirm if our current set-up generated temperatures sufficient to cause thermal injury and, if so, whether changing to a smaller calibre of optical cable would minimise this risk.
Methods
In this study we compared two different calibre Stryker® (2825 Airview Boulevard Kalamazoo, MI 49002. USA) optical cables, 3.0 mm and 5.5 mm. Each cable connected a Stryker® L9000 light-emitting diode (LED) light source to a Snowden-Pencer™ (5175 S Royal Atlanta Dr Tucker, GA, 30084-3053 USA) 88-1088 Tebbetts lighted retractor with 3.5 mm light port. The same light source and retractor were used for each cable.
Temperature measurements were recorded at multiple points along the connection between each optical cable and the lighted retractor using Philips 21091A (65 Epping Rd, North Ryde NSW 2113, Australia) small bead type temperature sensing probes connected to an Omega (800 Connecticut Avenue Suite 5N01, Norwalk, CT 06854, USA) OM-DAQPRO-5300 Datalogger (Figure 1). Ambient temperature was also measured. For each cable, we measured the change in temperature at each point for 120 minutes after the light source was turned on. After 120 minutes the light source was turned off and the temperature continued to be recorded until it returned to baseline. In order to determine if the size of the optical cable affected the quality of the light produced, we also measured light intensity using a YEW 3281 Lux Meter (Yokogowa Australia Pty Ltd, Level 3, 66 Waterloo Road Macquarie Park, NSW 2113 Australia).

Results
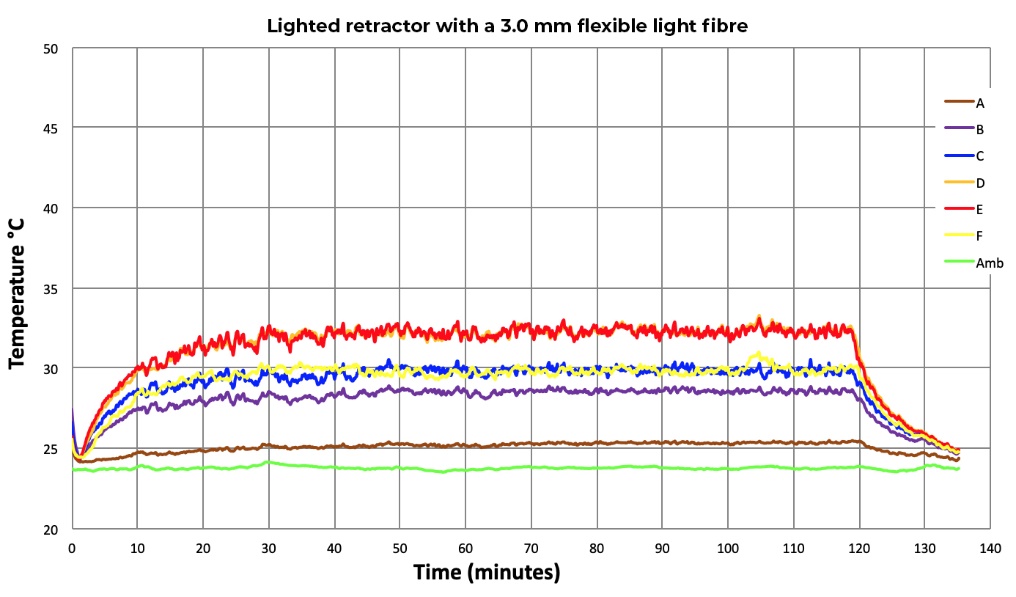
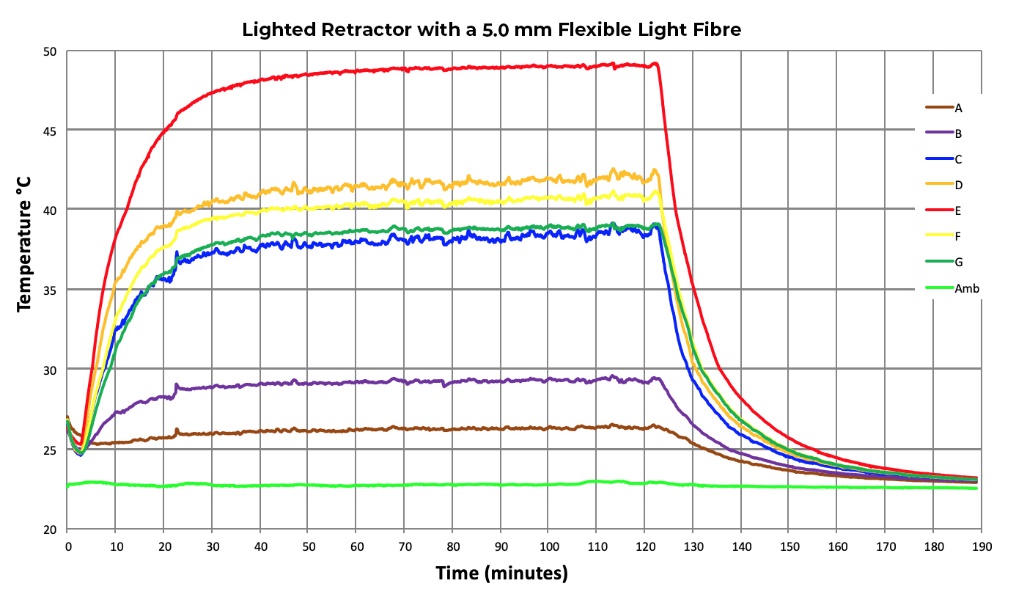
Both optical cables showed temperature rises. The 3.0 mm optical cable reached a peak temperature of 33.29 °C after 44 minutes and 47 seconds (Figure 2). It took 14 minutes and 28 seconds to return to baseline temperature (defined as less than 25 °C). The 5.5 mm optical cable reached a peak temperature of 49.23 °C after 53 minutes and 19 seconds (Figure 3). It took 35 minutes and six seconds to return to baseline temperature. Light intensity for the 3 mm optical cable was 2500 lux (adjusted for background light). Adjusted light intensity for the 5.5 mm optic cable was 2450 lux. This demonstrates that the 3.0 mm optical cable generates less heat at the connection between the cable and the retractor without compromising the quality of light emitted.


Discussion
Our study was prompted by a recent case in our unit of a patient who sustained a partial thickness burn to the right breast from the use of a lighted retractor during alloplastic reconstructive breast surgery. We reviewed the literature and found several case reports of iatrogenic full thickness burns from the use of cold light sources and optical cables during orthopaedic arthroscopic surgery.1–3 A review of the US Food and Drug Administration (FDA) adverse event report database also confirmed that our case was not an isolated incident. The FDA database has logged greater than 30 occasions where a patient undergoing breast surgery sustained a burn from the heat generated at the connection between an optical cable and a lighted retractor.4 In 2012, in response to reports of these injuries, the manufacturer of Snowden-Pencer™ Tebbetts lighted retractors issued an urgent safety notice to all of its distributors advising them not to use an optical cable with a calibre greater than 3.5 mm with their retractor due to the risk of thermal injury.5 Unfortunately, this warning has not prevented thermal injuries from the use of lighted retractors in breast surgery, as reflected in the FDA database and our recent case.4
The calibre of optical cable contributes to the risk of thermal injury due to the size mismatch between the cable and the retractor connector. When the optical cable is of greater calibre than the connector, light is lost as heat when it passes from the cable to the lighted retractor.6 This risk is greatest when optical cables are new as the fibres in older cables become damaged over time, reducing the amount of light that is transmitted at the connector.6
The degree of thermal injury depends on the temperature generated and duration of exposure. In a porcine model Moritz and colleagues demonstrated that partial or full thickness burns from hot water can occur at temperatures as low as 44 °C with prolonged exposure (6 hours). Every 1 °C increase in temperature reduces the time to cause thermal injury by approximately half.7
Prompted by our patient’s injury and our review of the literature we sought advice from our hospital’s biomedical engineering department regarding the safest calibre of optical cable for our retractor that would still provide adequate illumination. They recommended the use of a 3.0 mm optical cable. Given the risk is greatest with a new cable we chose to compare our current, older, 5.5 mm optical cable with a new 3.0 mm cable in order to investigate our hypotheses that our current cable could generate sufficient heat to cause thermal injury and that the use of a 3.0 mm cable would prevent this from occurring.
Our study confirmed that a 3.0 mm optical cable prevents the connection between the cable and the Snowden-Pencer™ Tebbetts lighted retractor from reaching temperatures that can cause thermal injury. We used an LED light source as previous studies have confirmed the superior safety profile of LED light sources to Xenon high intensity discharge light sources in terms of heat generated.8 By avoiding Xenon light sources, and using an appropriately sized optical cable for the lighted retractor, we avoid our reliance on human factors to prevent injury to our patients. Since this study our unit has converted to using only 3.0 mm optical cables and has found no disadvantages to this change in practice. However, our analysis was limited to a single cable of each size. Further testing of different brands, calibres and ages of optical cables as well as different brands and types of lighted retractors would add further weight to these results.
Conclusion
Despite the documentation of the risks in the literature, and recommendations by manufacturers to avoid large calibre optical cables, many plastic surgery units continue to expose their patients to the risk of thermal injury by using inappropriately sized optical cables with Tebbetts lighted retractors. We recommend that hospitals have a range of optical cables available for use with lighted retractors and endoscopes, and use a 3.0 mm optical cable with the Tebbetts lighted retractor in order to reduce the risk of thermal injury from this instrument. Alternatives such as headlights or, if available, cordless lighted retractors should also be used where appropriate to further minimise the risk to patients from the use of cold light sources and optical cables.
Acknowledgements
Tony Carlisle, Biomedical Engineer, Flinders Medical Centre.
Disclosure
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.
Revised: 2021 January 25; February 18 AEST