



Introduction
Several techniques are described for chest wall contouring in female-to-male (FTM) transgender patients, each with specific applications and limitations. The principal aim in mastectomy for FTM transgender patients is to masculinise the chest by removing the female contour. Subcutaneous mastectomy is usually the first surgical procedure to be completed by FTM transgender patients and is an important procedure in the transition to obtain a more male-like physique.1–3 Factors to consider in FTM mastectomy are the aesthetic requirements of the male chest, elimination of anatomical female breast features, operative technique, scar minimisation and success of outcome.4–6 Current techniques described have different applications depending on breast size, ptosis and skin laxity. We describe a new technique for FTM patient chest wall reconstruction known as the ‘flying brevet’.
The purpose of the study was to describe the flying brevet technique for FTM mastectomy and present a single surgeon’s 15-year experience with 113 consecutive cases. The flying brevet gained its name fortuitously due to the pattern of skin excision resembling a set of wings awarded to pilots. The flying brevet is an alternative to existing FTM mastectomy techniques and can be used for a wide range of breast morphologies. It is a procedure designed to maintain NAC viability while facilitating the removal of glandular tissue and a moderate amount of skin. We present a description of the flying brevet technique and single surgeon experience to offer an additional technique for mastectomy in FTM chest reconstruction.
Methods
A retrospective review of all flying brevet FTM mastectomy cases performed by the senior author in private practice from 2004 to 2019 was done. All patients included in the review presented for chest reconstruction for FTM transitioning; patients presenting for gynaecomastia management were excluded. One hundred and thirteen consecutive patients underwent the flying brevet procedure at three private hospitals in Brisbane, Queensland. Ethics approval was obtained from Greenslopes Private Hospital research and ethics committee [HREC 17/41].
Prime outcome measures included surgical technique, complications and revision surgery. Demographic data (age, self-reported preoperative cup size, smoking status) was obtained from retrospective review of medical records. Descriptive statistics of demographic, operative and outcome data were reported as a mean (range) or as a percentage of patients having that characteristic. Complications were recorded at follow-up reviews. Follow-up was for a period of at least six months after the last surgical procedure.
Prior to operative intervention for FTM mastectomy, patients have undergone psychiatric counselling, hormonal therapy and are living in transition as a male in the community. Hormonal treatment is continued throughout surgery and chest compression garments are worn postoperatively in all cases. Patients consent to have clinical photographs taken pre and postoperatively for clinical purposes.
Surgical methods
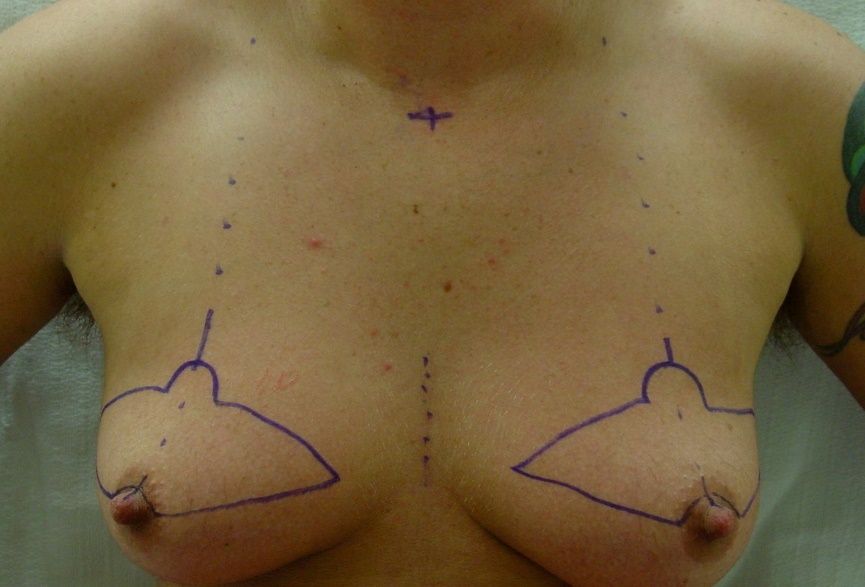
The flying brevet FTM mastectomy is performed under general anaesthesia with tumescent local anaesthetic infiltration and is performed as an overnight hospital stay or as a day procedure in a licensed day procedure unit. Preoperatively, the awake patient is marked in the sitting position, with a superior semicircular areolar incision, from 3–9 o’clock. This facilitates a degree of areolar reduction. The nipple height is dependent on patient height and from 17–19 cm from sternal notch to nipple. The incision extends bilaterally, with a soft arc joining the two sides and a semicircular hood for the new nipple position (Figure 1).

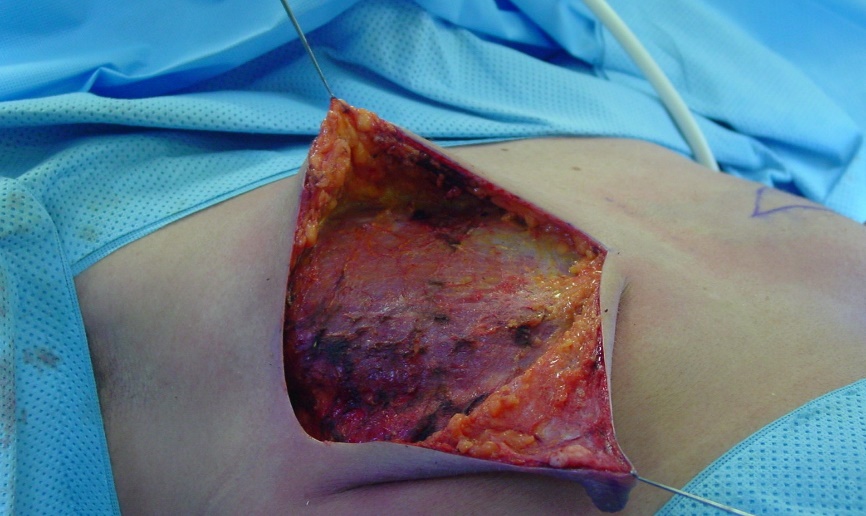
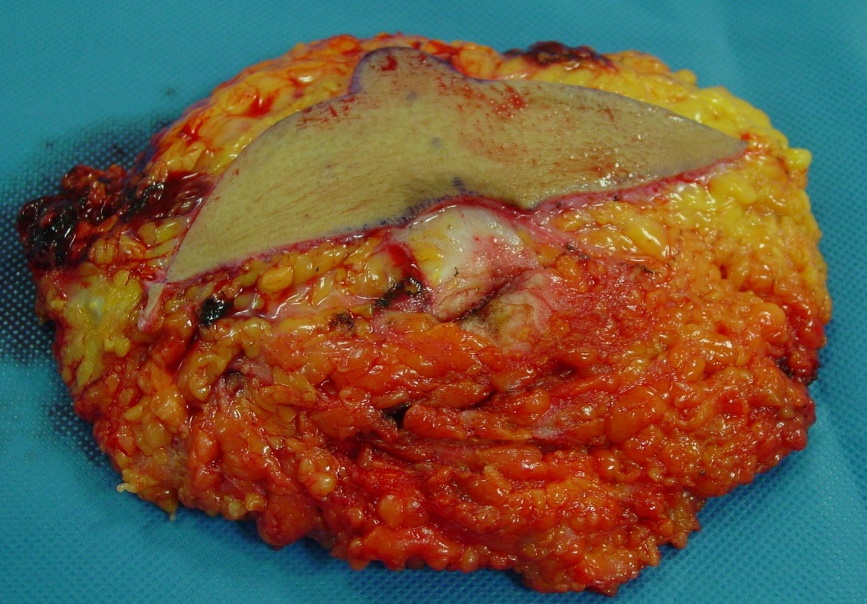
Under general anaesthesia, mastectomy is carried out to the level of the pectoral fascia with obliteration of the inframammary fold (IMF) (Figure 2). The superior skin paddle is removed along with the glandular tissue and the most redundant and stretched skin in ptotic or larger breasts. Specimens are sent for histopathology (Figure 3). The defect can be directly closed with one layer (3–0) medial and lateral incisions and (4–0) periareolar, either Monosyn (Braun; Bella Vista, NSW, 2153) or Monocryl (Ethicon; Preston, VIC, 3072).


Liposuction may be performed during the initial procedure to smooth chest wall contours although in recent years (since 2014) the senior author has elected to no longer perform preoperative liposuction as he did not believe that it aided significantly in flattening the chest and rather contributed to the risk profile.
Drains are routinely required. Patients wear fitted garments for the following six weeks and are seen at day eight, day 22 and four months postoperatively. On further assessment, nipple sensitivity is documented.
If a second operation for chest wall reconstruction is required, it is based on an inferior semicircular areolar incision (Figure 4) and the use of existing scars permits removal of any redundant skin and definitive NAC remodelling. The wound is closed with Monosyn/Monocryl sutures (3–0, 4–0) and drains are routinely used. There is a delay between procedures of six to nine months if a second operation is required (Figure 5). This is to allow wound healing and development of a new superior dermal neurovascular pedicle.


Results
A total of 113 patients, with a median age of 27 years old (18–64) at the time of first surgery, have undergone the flying brevet procedure for chest wall reconstruction in FTM transitioning. Breast cup size of the patients undergoing the flying brevet procedure ranged from A to E, with the majority of patients being a size B or C cup: 30 (26.5%) and 51 (45.1%) patients respectively. The mean mastectomy breast weight for each breast was 462 g with the range being from 81 to 2662 g. Forty-four patients (38.9%) underwent preoperative liposuction prior to mastectomy. Since 2014, liposuction has no longer been performed preoperatively, as the senior author did not believe that it aided significantly in flattening the chest and rather contributed to the risk profile.
Thirty-four (30.1%) patients proceeded to a second operation for chest wall contouring; the majority of these patients were C cup size breasts and larger. The reason for proceeding to a second operation was to resolve lower pole skin excess that was persistent from the first operation. ‘Touch up’ procedures were performed in 13 (11.5%) patients; these procedures included excision of dog-ears under local anaesthetic (three patients), lipectomy of lateral chest wall subcutaneous tissue (five patients) and NAC reduction (five patients). There were no abnormal pathology results in any of the specimens sent.
Complications with this procedure included postoperative haematoma (7%),7 hypertrophic scarring (6%)8 and a single incidence of fat necrosis. Haematoma in our series occurred mostly following large (> 400 g) mastectomy. Hypertrophic scarring was treated with silicone dressings in our patients. One case of full NAC necrosis occurred in a patient who refused to follow recommendations for postoperative care and subsequently experienced a postoperative haematoma and infection. He was an active smoker with size A cup breasts, minimal ptosis and 136 g breast tissue excised from each side. He failed to attend any further appointments. There was one case of partial NAC necrosis. This event occurred in a patient with macromastia (2662 g and 2186 g excised each side), grade three ptosis, who was a smoker. This case was successfully managed with dressings. There was one postoperative infection in our series (previously mentioned). To date, there have been no cases of late onset of keloid scarring during follow-up of any of the patients
Discussion
Gender dysphoria is a severe form of gender identity disorder that can be treated with hormone therapy and sexual reassignment surgery.2 In FTM transgender patients, the first surgical procedure in their reassignment surgery usually consists of a subcutaneous mastectomy.8 Removal of the female breast is an important step in the transitioning process to a new gender identity and it is a procedure that has a high rate of patient satisfaction.3,8
Many of the techniques for FTM mastectomy have been adapted from the treatment of gynaecomastia.8 However, performing a subcutaneous mastectomy in a FTM transgender patient is more difficult than in a male with gynaecomastia. It should be noted, that in most cases, the FTM patient will have significantly more breast volume and a greater degree of skin excess and ptosis than a gynaecomastia patient.7,8 Objectives of the subcutaneous mastectomy are to masculinise the chest by removing breast tissue and excess skin, reducing and properly positioning the NAC and obliterating the IMF, ideally with minimal chest wall scarring.1,5,8
To date, there are a number of approaches for mastectomy for FTM gender reassignment surgery, including the semi-circular, trans-areolar, concentric circular and extended concentric circular approach, and the free nipple-areolar complex graft.7–9 These techniques have different applications depending on breast size, ptosis and skin laxity: smaller breasts may be approached via inferior semicircular technique7; transareolar technique allows immediate nipple reduction at the expense of more obvious areolar scar7; the concentric circle technique is for medium or smaller breasts excisions5; and for larger breasts, raising a NAC flap with areolar and inframammary incisions and free nipple grafting and breast amputation have been advocated.7–9 The challenge in FTM mastectomy is the compromise between minimal scarring and adequate tissue resection.
The flying brevet technique is a procedure tailored to FTM patients but it can also be used for large gynaecomastia patients. As a single stage operation, the technique is most suited to patients with large B or small C cup size with a moderate amount of excess skin where a technique with a lesser scar may not achieve the same glandular and excess skin resection (figures 6 and 7). Patients with C cup size or larger breasts, or with long nipple to IMF distance, often require a planned, two-stage procedure using the flying brevet technique, with the second stage performed to resolve any persistent excess lower pole skin following the first operation.


The flying brevet gained its name fortuitously due to the pattern of skin excision resembling a set of wings awarded to pilots. The incision has some similarities to the ‘omega’ or ‘batwing’ technique described by Christianson10 in 2007 for breast reduction following radiation therapy that involves superior incisions for elevation of the nipple.10 The flying brevet technique involves inferiorly angled lateral and medial incisions to aid scar camouflage and also aims to place the NAC more laterally.
The flying brevet procedure is presented as an alternative technique for FTM mastectomy that can have good results for a variety of breast morphologies but with its own limitations. The scar is potentially better than that of breast amputation and free nipple graft but for larger breasts, a two-stage approach may be necessary to manage excess lower pole skin. In addition, minor ‘touch up’ procedures under local anaesthetic may be required to achieve the final result.
Results show a similar profile of complications compared with other techniques including sensory problems, necrosis and adverse scar formation. An unfortunate weakness of this study is the absence of recording of the NAC position postoperatively and the lack of patient satisfaction data. As the study was a retrospective review, the reliance on case notes made it difficult to report on outcomes for patients that failed to present for follow-up.
Conclusion
The flying brevet technique provides a consistent method of mastectomy for FTM chest wall reconstruction. It permits large glandular and skin resection in ptotic breasts with preservation of NAC circulation. Major complications included postoperative bleeding, as recognised in other methods. The flying brevet procedure is an additional technique that can be added to the current options for mastectomy in FTM chest wall reconstruction.
Acknowledgments
The authors thank Dr Amy O’Connor for previous research contribution.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Revised: August 11, 2019 AEST
Updated: June 23, 2021 AEST—new formatting