


Introduction
Fractures of the triquetral bone are the second most common isolated carpal bone fracture behind fractures of the scaphoid.1–3 The most common triquetral fracture are volar avulsion fractures, fractures through the triquetral bone and cortical fractures of the dorsal surface of the triquetral.3,4 These fractures are attributed to various injuries including compression by a prominent hamate through wrist hyperextension,5 impaction by the ulnar styloid,3 and damage to the dorsal cortex of the triquetrum associated with dorsiflexion and ulnar deviation of the wrist.1,3,6 Dorsal cortex avulsion fractures of the triquetral most commonly occur by the transmission of force through the dorsal radiocarpal ligament (radiotriquetral) and dorsal intercarpal ligament (triquetroscaphoid).1,3,7,8 These fractures are generally associated with forced wrist flexion.5 Fractures through the triquetral bone are generally associated with extreme, high energy, dorsiflexion of the wrist but can be associated with extreme axial loading, causing the ulnar to impact the triquetral.5 High energy direct blows to the wrist can also result in a triquetral bone fracture in a number of planes.5
Each of these triquetral fractures types is commonly associated with swelling and tenderness along the ulnar aspect of the wrist. This pain is more readily elicited with the wrist in radial deviation.5
Ideal imaging for fractures of the triquetral is the anteroposterior (AP) projection of the wrist view radiograph,5 although dorsal chip fractures are more readily viewed on lateral projection radiographs. A volar avulsion injury may more easily be detected on wrist view radiographs with the wrist in radial deviation.5 In cases where the fracture is difficult to see on radiographs alone, CT imaging may be required to confirm the diagnosis.
The management of triquetral avulsion fractures is generally non-surgical and involves immobilising the wrist for three to four weeks to allow the ligaments to heal followed by a progressive return to the normal range of motion and gradual strengthening,3 with pain generally subsiding within six to eight weeks.3,9
Triquetral bone fractures, which are commonly associated with crush injuries, axial dislocations or high energy trauma,3 are managed based on the degree of displacement and presence of other associated injuries.3 As a result, CT imaging may be required to show the full extent of the injury. Non-union of the triquetrum fracture following four to six weeks of immobilisation, is rare.3,10,11 However, triquetral bone fractures associated with high energy trauma and crush injuries resulting in instability of the lunotriquetral ligament may require surgery to re-align and fix the bone (open reduction and internal fixation or ORIF).3
Where a volar avulsion fracture of the triquetral involving the palmar ulnar triquetral ligament or the lunotriquetral ligament and is associated with carpal instability, MRI may be beneficial to reveal the full extent of the injury to ligaments. In this instance, treatment is directed to the management of carpal instability with secondary consideration given to the avulsion fracture.3 When there are other bony or ligamentous injuries, non-union of the fracture and other complications such as persistent ligamentous instability and future pisotriquetral arthritis, are more common.3
Methods
Data of emergency department and outpatient clinic presentations for the period of 2009–2018 was obtained from hospitals within the Blue Mountains and Nepean local health district of New South Wales, Australia (Nepean Hospital ethics approval no: NBM18/805). Records with a triage/diagnosis category of triquetral fracture or carpal bone injury were selected for review (n = 1293). Those patients with a radiological diagnosis of triquetral fracture (121, 9.4%) were selected for further data analysis.
Results
Cohort
Of the 121 patients with fractures of the triquetrum were identified during the study period (2008–2019), 111 were followed up clinically for an average period of 46 days (6.6 weeks), with a range of seven to 98 days of follow-up. Of these, 46 were female (41.4%) and 65 male (58.6%).
Mechanism of injury
As seen in Figure 1, falling onto an outstretched hand was the most common mechanism of injury in the cohort (84 patients, 75.7%), followed by motor vehicle accidents (13 patients, 11.7%). A fall from a height ranging from 1.5–5 m accounted for the triquetral fracture for six patients (5.4%). The remaining triquetral fractures were sporting related (three patients, 2.7%) or unspecified (five patients, 4.5%).

Fracture classification
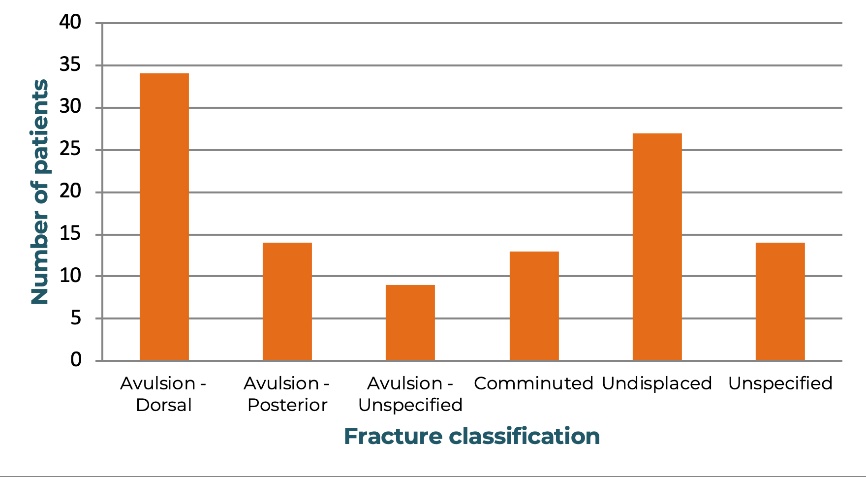
The triquetral fractures were classified into four groups based on radiological findings. As seen in Figure 2, avulsion (dorsal) fractures were the most common triquetral fracture (62 patients, 55.9%), followed by avulsion (volar) fractures (19 patients, 16%) and other avulsion (radial or ulnar aspect) fractures (10 patients, 9%). Comminuted fractures were seen in 20 patients (18%), indicating that avulsion type injuries are much more commonly seen in triquetral fractures. Figure 3 demonstrates the common patterns of triquetral fracture on radiograph and CT scan, highlighting that these fractures are often difficult to identify.


Diagnosis
As seen in Figure 4, triquetral fractures were diagnosed on radiograph alone in 72 patients (64.9%). A further 21 patients (18.9%) were deemed negative for triquetral fracture on initial X-ray and required CT imaging to make a definitive diagnosis. The remaining 18 patients (16.2%) proceeded straight to CT scanning for investigation and diagnosis. Of the whole cohort, a primary or secondary assessment by CT imaging was performed in the majority of patients (78 patients, 70.3%).

Management
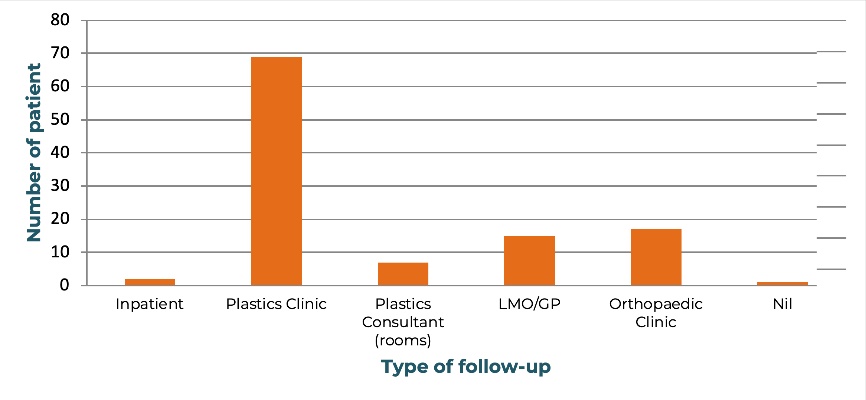
All patients in this cohort were treated with immobilisation through splinting/casting. For two patients, the follow up was performed as an inpatient (1.8%), due to the patients either representing to hospital for other medical issues or remaining as inpatients due to other injuries. The majority of patients in this study (69 patients, 62.2%) followed up through the plastic surgery outpatient clinic at Nepean Hospital. A number of patients (17, 15.3%) were followed up in orthopaedics clinics or with the patient’s local medical officer/general practitioner (15, 13.5%). Of the remainder, seven patients (6.3%) were followed up privately with a consultant plastic surgeon, or had no planned follow up at the time of discharge (one patient, 0.90%).
The mean time for an initial follow-up appointment was 1.6 weeks (range one to zero weeks). The mean time for a subsequent review was 4.5 weeks (range one to 12 weeks) with the mean total time for follow-up at 6.6 weeks, with a range of three to 14 weeks.
Patient outcomes
As seen in Figure 5, 94 patients (84.7%) returned to baseline wrist strength with range of motion (ROM) and were ultimately pain free following immobilisation and progressive treatment with hand therapists. For the 15 patients (13.5%) who did not returned to baseline function, there was one or more of either ongoing pain, reduced wrist ROM or reduced wrist strength. For the remaining two patients (1.8%) who were not at baseline at the time of reporting, further splinting or hand physiotherapy was still ongoing.

Patients were asked to complete activities of daily living (ADL) with each hand/wrist to assess ROM and strength following treatment. ‘Back to baseline’ conditions were considered to have been met when the affected side had similar levels of ROM and strength to the contralateral side, unless patients indicated that the contralateral wrist had undergone previous trauma. There was only one such case and in that instance, patient reported ADLs and strength were used instead. Patient reported pain was similarly recorded, where patients were asked if they had any pain at rest or during any of their ADLs.
Discussion
Triquetral fractures are the second most common carpal fracture and, when untreated, can result in significant pain and impaired function of the affected wrist,6,12,13 highlighting the importance of identification and appropriate management. It has been outlined previously that the mechanics of a fall, whereby the wrist is put into full extension, promotes a chisel action of the wrist resulting in a dorsal bone avulsion and other injuries to the triquetral bone.9 Our results indicate that identifying a triquetral fracture on X-ray imaging can be challenging as 18.9 per cent of our population required CT imaging to correctly diagnose triquetral fracture. This study supports the management of triquetral fractures without signs of wrist instability, through cast immobilisation for four to six weeks6,12,13 followed by progressive hand therapy exercises until return to function at six to eight weeks.
Conclusion
Triquetral fractures can be challenging to identify with radiography and are commonly identified as lunate fractures.13 If there are ongoing symptoms and a high clinical suspicion, CT may be indicated and, in future practice, may be justified as a first line imaging modality. This study also demonstrates that short arm-wrist immobilisation is an effective management option for triquetral fractures.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Revised: September 16, 2019; December 13, 2019 AEST