
Introduction
Skin flap necrosis (SFN) in skin-sparing mastectomies is a known complication that can range from mild to severe full-thickness necrosis in 2 to 22 per cent of patients.1–6 Several methods of assessing flap viability in the intraoperative setting have been utilised. However, they are expensive and often not readily available. Two recently published papers have demonstrated that glyceryl trinitrate (GTN) ointment, used as part of the dressing to cover the entire skin flap, can markedly reduce the incidence of SFN.1,2 This case report of immediate implant breast reconstruction following bilateral skin-sparing mastectomy highlights the utility of infrared imaging to target topical treatment and reduce potential treatment side effects.
Case report
A 53-year-old female underwent a prophylactic bilateral skin-sparing mastectomy indicated by a genetic risk of breast cancer. Her comorbidities were otherwise unremarkable, and she was a non-smoker. Her preoperative bra size was 12DD. A small transverse elliptical incision included the entire nipple–areolar complex. A total weight of 611 g and 601 g was removed from the left and right breasts, respectively. Mastectomy was followed by an immediate bilateral breast reconstruction with pre-pectoral 285cc nano-textured Motiva Ergonomix® round implants and Flex HD dermal matrix (Establishment Labs, Coyol Free Zone, Alajuela, Costa Rica). An infrared imaging tool known as FLIR (forward-looking infrared) was used intraoperatively to aid in skin flap tailoring and removal of potentially threatened skin edges. The patient followed an uncomplicated intraoperative course and was reviewed day one postoperatively.
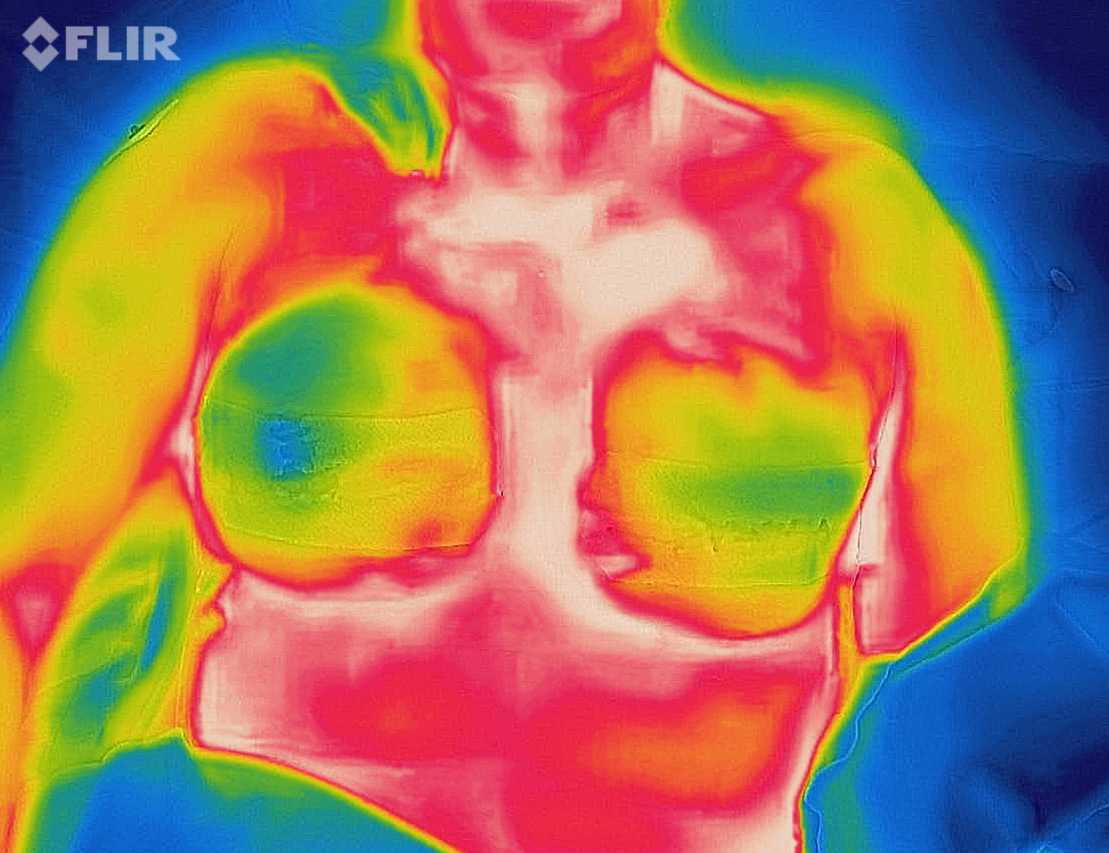
On review day one, FLIR was used to take an infrared image of the operative site at a distance of 1.5m. The upper outer quadrant of the right breast was shown to have a reduced temperature, in addition to a capillary refill of 2.5–3 sec, suggesting an area of compromised blood supply. The patient’s blood pressure was 104/57 mmHg and her heart rate was 57bpm at the time of the initial infrared assessment with a room temperature of 24 °C. A 1.5cm strip of topical GTN (0.2%) ointment equating to 0.4mg of GTN was applied to the area. A repeat infrared image taken 30min after application of the GTN ointment showed a marked improvement in the temperature of the area as well as an improvement in capillary refill and overall skin colour. Her blood pressure remained stable at 108/64 mmHg and her heart rate at 69 bpm with no change in ambient room temperature. The GTN cream was therefore applied three times daily over a 48-hour period as per eTG guidelines for topical use. The patient’s blood pressure throughout the 48-hour period remained constant. However, she did suffer from the common side effect of headache.
The patient was followed up for three months postoperatively and showed no signs of partial or full-thickness flap necrosis or operative complications.
Discussion
Skin sparing mastectomy (SSM) with immediate implant-based reconstruction is increasingly being performed in Australia for breast cancer management. In one prospective study the overall SFN after mastectomy with implant reconstruction was reported at 14 per cent, with 5 per cent experiencing severe full-thickness necrosis.4
Several risk factors for SFN have been identified including smoking, obesity, incision type, specimen size, history of previous augmentation, nipple-sparing mastectomy and time from incision to specimen removal.1–7 Flap necrosis can have significant impacts on patient recovery physically and psychologically and on aesthetic outcomes. Often, patients will not wish to proceed with further reconstruction after implant failure.7
Two recent papers, a randomised controlled trial and a retrospective cohort study, have investigated the efficacy of using GTN ointment to reduce the rate of mastectomy flap necrosis.1,2 In these papers, GTN was used as part of the postoperative dressing regimen and patients in the treatment group received coverage of the entire operative breast with GTN ointment as a one-off dose. Turin and colleagues found an overall 22 per cent reduction in mastectomy skin flap necrosis.1 The rate of full-thickness flap necrosis was reduced by 44 per cent. This figure, however, represented only a trend towards statistical significance. Gdalevitch and colleagues found that some of their treatment group (15.3%) experienced skin necrosis, compared with a larger amount in the placebo group (33.8%), a difference of 18.5 per cent. This powerful vasodilator has been studied previously in skin flap survival and has demonstrated improved flap survival.2 GTN has been compared with other vasodilators such as oral phenoxybenzamine, oral nifedipine and intravenous allopurinol, yet GTN has been found to be superior compared with these medications.1,2
A small number of techniques have been described for assessing skin flap viability intraoperatively. These techniques include on-table intravenous fluorescein with Wood’s lamp assessment and laser-assisted indocyanine green (ICG) angiography. Both techniques have lower rates of skin flap necrosis and reoperation when compared with direct visualisation of the flap alone.6 Interestingly the fluorescein with Wood’s lamp technique showed the lowest rates of mastectomy flap necrosis over ICG angiography. As discussed by Rinker, this may suggest that the superficial vascular plexus, highlighted by fluorescein, is more predictive of skin viability that the deeper plexus.6 Despite these techniques being effective, they may not be an economically viable option in most centres due to the large cost involved.
In the case study patient, we aimed to target the areas of GTN used. The technology utilised was the inexpensive FLIR ONE Pro iPhone and android phone thermal imaging camera (FLIR Systems Inc., Mulgrave, Victoria, Australia). It can capture a wide range of temperatures but more importantly has a spot meter with a resolution of 0.1 °C. The accuracy, however, is dependent on factors such as distance from the object, ambient temperature and the emissivity of the object. These factors were controlled for, and images captured pre- and post-GTN application were at the same distance from the patient and within the same room 30 minutes apart (Figures 1 and 2). To take into account the possibility of overall bodily perfusion causing the improvement, the patient’s blood pressure variation was included in the analysis of results. Interestingly, the left breast also showed signs of improved perfusion despite only the right breast being topically treated. This is readily explained by systemic absorption of the drug with accompanying overall vasodilation. The well-documented side effect of headache experienced by the patient during treatment further supports this hypothesis. The local concentration, however, would be expected to be much higher than in the general circulation.


GTN is an affordable treatment option and the risk of complications is low, notably headache and hypotension (2.4%).2
Conclusion
This case report highlights how GTN ointment can be used to increase skin perfusion in immediate implant-based reconstruction and importantly outlines a simple cost-effective reproducible means of measuring treatment effectiveness with an infrared camera.
Patient consent
Written patient consent was obtained prior to taking any images, including the use of an infrared camera or digital camera. Additionally, written consent was obtained for the publication and reproduction of photographs, recordings and other audiovisual material related to the case and textual material.
The case report was sent to the local Human Research Ethics Committee for approval of publication.
Conflict of interest
The authors have no financial or commercial conflicts of interest to disclose.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Revised: April 28, 2020 AEST