Introduction
First described by Koshima in 2004,1 a classical superficial circumflex iliac artery perforator (SCIP) flap differs from a conventional groin flap in that it includes only a short distal segment of the superficial circumflex iliac artery (SCIA) system with a dominant perforator.
The SCIP flap has gained in popularity due to its thinness and superior donor site scar. The inguinal region is one of the thinnest areas of skin (dermis to epidermis: 625.9 to 273.4 μm in a Korean population) and is the ideal flap for soft-tissue defect reconstructions that are contour-essential.2 The scar of the SCIP flap is also well hidden within the underwear line. Like all perforator flaps, the SCIP flap can be customised to include different composition of tissues from skin, bone, subcutaneous fat, lymph nodes, vascularised nerve and fascia.3–9 The variations of the SCIP flap and their clinical applications have been well summarised by Iida and colleagues.10
There exist inconsistencies in the description of the surface location of the SCIA perforators and the attainable pedicle length for such flaps. The aim of this review was to provide a summary of published evidence regarding the surgical anatomy, preoperative imaging and surgical approach to safely identifying SCIP flaps.
Methods
This study collates all publications on free SCIP flap reconstruction, with a particular focus on flap surgical anatomy, preoperative imaging and surgical approach to flap elevation. This review adheres to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines. This review and its authors also conform to the ethical principles of the Declaration of Helsinki of the World Medical Association.
The literature search was performed by two independent reviewers through the MEDLINE® and Cochrane databases. The medical subject headings (MESH) search terms included ‘superficial circumflex iliac perforator’, ‘SCIP’ and ‘groin perforator’. A free text search or a MESH term search was used wherever appropriate, and Boolean operators were used to combine the terms. There were no restrictions on publication date or status.
Eligibility criteria
The inclusion criteria consisted of any meta-analyses, systematic reviews, case-control and cohort studies, or case reports involving SCIP flap surgical anatomy, preoperative imaging and surgical dissection. Articles excluded for surgical anatomy were those that involved paediatric patients, flaps raised without a cutaneous component and studies that did not include flap pedicle dimensions. Chimeric flaps were also excluded from the study.
Study selection and data collection process
Citations found by means of searching the databases were screened for eligibility by title and/or abstract. Full-text articles were then appraised for final inclusion in the quantitative analysis. The two reviewers listed extracted data separately, and discrepancies were reviewed and discussed until a consensus was accomplished.
Results and discussion
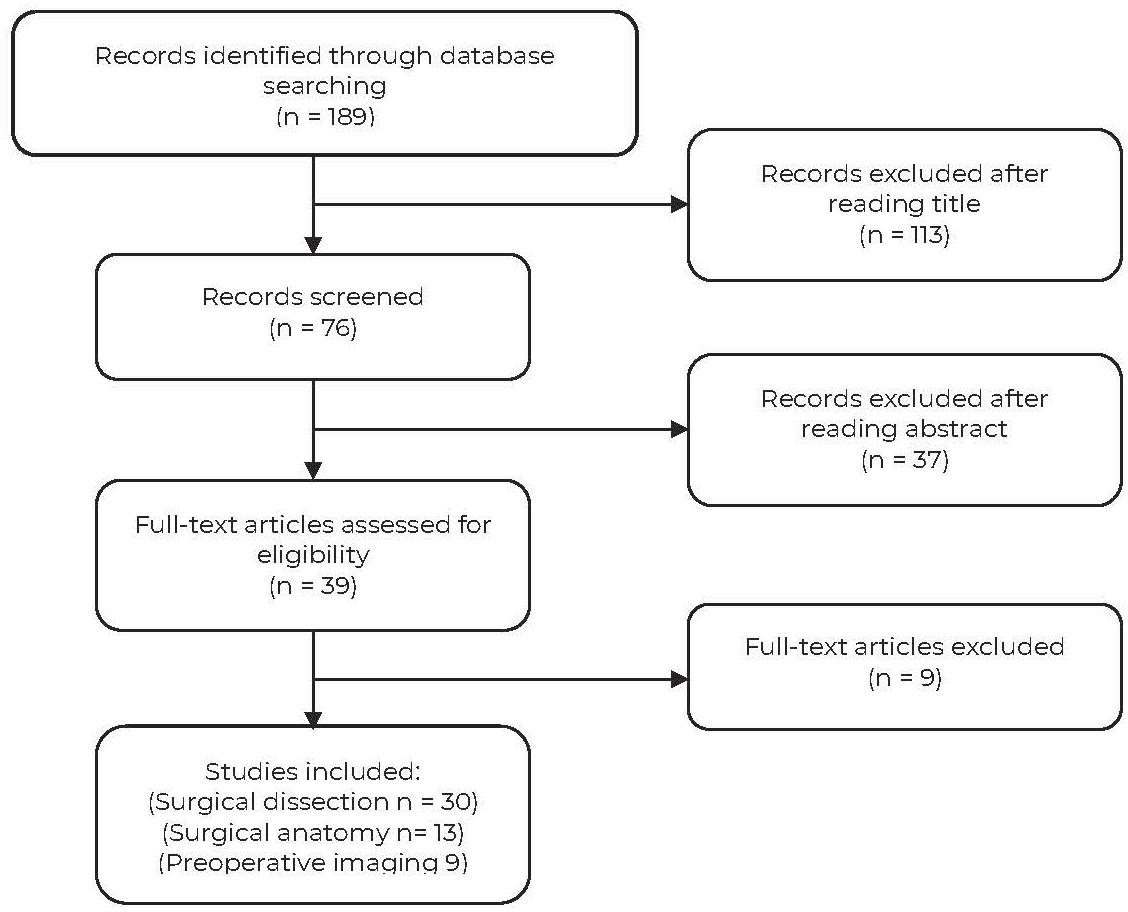
Through the initial search, 189 articles were identified (Figure 1). After screening the titles, 76 publications remained. This number was further reduced to 39 articles after reading the abstracts. Of these 39 articles (not mutually exclusive), 30 fulfilled the criteria for surgical dissection, 16 for surgical anatomy and nine for preoperative imaging. A total of 587 dissections were evaluated for the results of this study.

Groin perforator flap surgical anatomy
We summarised the literature on SCIP flap surgical anatomy and studies identified from the literature search were included if they described information on perforator origin, pedicle length, arterial diameter, flap size and thickness, and vein harvested for anastomosis.
There are multiple blood supplies in the groin region, with contributions from the SCIA, superficial inferior epigastric artery (SIEA), fourth lumbar artery, deep circumflex iliac artery and superior gluteal artery systems.11 For the purpose of relevance to this review, only the anatomy of the SCIA and SIEA are described. The course of the SCIA remains variable. Taking advantage of the advent of preoperative computed tomography angiography (CTA), Suh conducted the largest study of SCIA anatomy.12 Of 284 SCIA in 142 patients, most originated from the femoral artery (83.5%), while some originated from the superficial femoral artery (8.5%) or deep circumflex femoral artery (7.0%) and only a few (1.0%) originated from the lateral circumflex femoral artery. There also remains variability as to the origin of the SIEA. In 38 dissections, the origin of the individual SIEA arose directly from the common femoral artery (CFA), a common trunk with the SCIA, a common trunk with the pudendal artery and the superficial femoral artery in 22 (57.9%), seven (18.4%), two (5.3%) and five (13.2%) of 38 dissections, respectively. In the remaining two cases, the SIEA originated from the external iliac artery or the lateral circumflex femoral branch of the deep femoral artery.13
In relation to the SIEA, the SCIA was described as sharing a common origin in 48 per cent of cases, as a large SCIA without a SIEA in 35 per cent of cases and both a SCIA and a SIEA with separate origins in 17 per cent of cases.11
In some instances, groin perforators can be supplied by the SIEA system rather than the SCIA system.14–16 The anatomical variation encountered during this systematic review could not be explained better by Pan’s study of angiosomes in the thigh and buttock, which found that the origin of the source arteries and their branches was subject to considerable variation, while the area of skin supplied by each cutaneous perforator was relatively constant.17 Therefore, the terminology ‘groin perforator flap’ is more appropriate than ‘SCIP flap’.
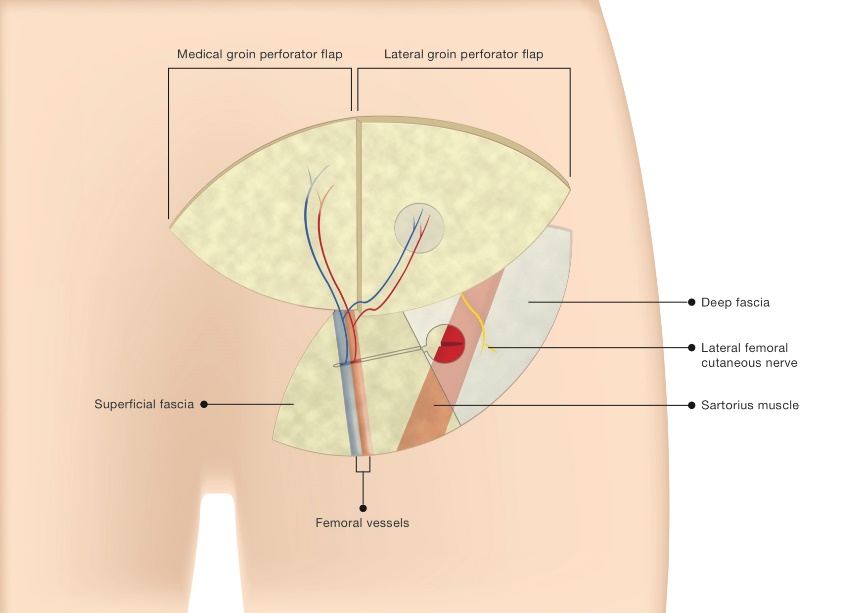
Figure 2 illustrates the two variations of the groin perforator flap when basing it on either the medial or lateral perforator. In most cases, the medial perforator of the groin arises about 1.5 cm distal to the SCIA origin from the femoral artery. In Suh’s study, it originated from the SCIA in 134 of 142 (94.4%) patients, the SIEA in five (3.5%) patients, the superficial femoral artery in two (1.4%) and the superficial pudendal artery in one (0.7%).18 It then penetrates the deep and superficial fascia directly after it branches from the SCIA.18,19 The lateral perforator follows a musculocutaneous course superolaterally beneath the deep fascia, parallel to the inguinal ligament. It then pierces the Sartorius muscle medially and perforates the deep fascia at its lateral border.1,19–21

Table 1 summarises the variability in the literature regarding the description of the surface location of either the medial or lateral groin perforators.1,10,14,15,22–25 It can therefore be challenging to suggest precise anatomical landmarks for the perforators. However, what remains consistent is that the lateral perforator lies directly above the Sartorius muscle in the groin region, while the medial perforator lies in close proximity to the inguinal ligament and is medial to the Sartorius muscle. This accentuates the value of CTA as it aids preoperative perforator marking with a Doppler probe.
Groin perforator flap anatomy and outcomes
A total of 584 flaps from 16 studies were included in this anatomical systematic review of SCIP flaps (Table 2).14,15,19,23–25,27–36 Of these, 579 (99.1%) were based on the SCIA while five were based on the SIEA (0.9%). The arterial diameters ranged from 0.3 mm to 1.8 mm, flap size from 2 cm to 224 cm2 and flap thickness from 3 mm to 23 mm. Medial perforator flap pedicle length ranged from 20 mm to 90 mm. For lateral perforator flaps the range of pedicle length was 26 mm to 100 mm (where 100 mm was achieved when based on reverse flow via the transverse branch of the lateral branch of the SCIA).14
Multiple studies describe achieving a longer pedicle length by dissecting the lateral perforator. However, the results displayed in Table 2 are inconsistent with this: Jin reported a 69 mm (range 48–90 mm) pedicle length for a medial perforator flap when dissected down to the SCIA origin.35 In contrast, Feng reported a mean length of 59 mm (range 26–100 mm) for lateral perforator flaps that were ligated at the SCIA origin.14 In fact, patient build and variability in groin arterial anatomy may be the determining factors for absolute pedicle length.
All but two of the 16 studies reported flap outcomes.23,36 From a total of 554 flaps, 520 had complete flap survival (93.3%), 20 had partial necrosis (3.6%) and 14 were a total loss (2.5%). Donor site morbidity was reported by two studies with a total of three cases of complication (0.5%). Goh and colleagues performed 210 flaps and reported one case each of donor site-related seroma and lymphorrhoea,31 while Lee and colleagues performed 41 flaps and reported one case of donor site seroma postoperatively.25
Flap venous anastomosis
Table 3 depicts seven studies with a description of their venous anastomoses for groin perforator flaps based on the SCIA.14,23,24,31,32,34,36 In comparison with the arterial anatomy, there remains a relative scarcity in the anatomical description of the venous system of the SCIP flap. Of 407 flaps, 132 (32.4%) venae comitantes (VC) and 251 (61.7%) superficial circumflex iliac veins (SCIV) were used for venous anastomosis. Goh concluded that in a series of 210 SCIP flaps, the flap outcomes of single (144) and dual venous anastomosis (66) were no different (4.5% and 4.9% flap success, respectively).31
Preoperative imaging
As discussed above, variability in the course of the source arteries (SCIA/SIEA) and the groin perforators justifies a preoperative CTA. This confers easier flap dissection and can aid in Doppler ultrasound preoperative marking. CTA (augmented with multi-detector rows) provides useful three-dimensional mapping of the SCIA and vessel calibre. It identifies the course and branching pattern of the SCIA, which is important for flap design, decreasing the harvest time and improving the safety of the flap.35 A systematic review of perforator flap preoperative imaging concluded that CTA is the gold standard in terms of accuracy, reproducibility and lower inter-operator variability.37 With the utility of CTA, this negates the unpredictability of the dominant perforator of the flap and the need to change flap design based on intraoperative findings. However, tracing of the perforators becomes challenging if the subcutaneous adipose layer is very thin or in the presence of a haematoma collection.12,38 In obese patients where anatomical landmarks cannot be accurately located, CTA can been used to radiologically pin-point where the perforators pierce the superficial and deep fascias. This is important in such instances, as excess adipose tissue can make perforator dissection challenging. A technique using the umbilical button as a reference point to mark the critical points where the perforator penetrates both fascias in CTA has been described.39
The Doppler probe is a fast, non-invasive and portable preoperative tool that remains crucial for surface markings of perforators of interest and can be quickly guided by CTA. Duplex ultrasound remains inferior to CTA in three-dimensional mapping and is operator dependent. However, it does provide information on vessel calibre and flow velocity, although it may become less useful with vessel diameters smaller than 0.5 mm.40 It has been shown to be able to detect hypoplasia in the SCIA/SIEA network and therefore can be beneficial in locating the source artery of the groin perforator, especially when CTA fails to do so in patients with a paucity of subcutaneous fat.
Surgical dissection
The limitation of a short pedicle in Koshima’s original description of the SCIP flap can be overcome by including the entire length of the SCIA. This has the dual effect of increasing vessel diameter size and pedicle length.29 There is also the option of pedicle elongation through reverse arterial flow from the distal deep end of the lateral SCIA branch and selecting the medial groin perforator (if anatomically supplied by the superficial branch).14,32
Inferolateral dissection of the SCIP flap remains a popular approach with right-handed surgeons due patient positioning and it also aids easy identification of Scarpa’s fascia over the anterior superior iliac spine (ASIS) due to the loose subcutaneous areolar connective tissue. However, novice surgeons may miss the medial perforator (supra-Scarpa’s fascia course) after dissecting out the lateral perforator (sub-Scarpa’s fascia course) and a superomedial approach would be safer. This becomes even more challenging in skinny patients with thin fat planes. In general, the flaps are elevated in the suprafascial plane to avoid the need for flap debulking. This plane can be identified by the difference in fat lobule sizes as they are smaller superficially and larger in the deeper plane.26,41
Earlier SCIP anatomical studies reported that the SCIA medial branch at times was hypoplastic or absent.1,19 However, Suh’s study demonstrated its ubiquity in the SCIA system on CTA.12 The finding that the branch appears hypoplastic intraoperatively may in part be due to the vasospasm that occurs during surgical dissection. In addition, as mentioned above, a deep and lateral approach to flap dissection may fail to identify the course of the vessel due to its medial and supra-Scarpa’s fascia course. A medial dissection approach, in addition, may keep the lateral perforator preserved should a bail-out option be required if the medial perforator is damaged iatrogenically.15 As such, there are no long-term data yet to recommend one approach over the other. Therefore, while bearing in mind the key advantages of each approach, the microsurgeon’s comfort with either technique should take precedence. A comprehensive video illustration has been included in a previous paper.31
For the lateral groin perforator, attention must be given to the lateral cutaneous nerve of the thigh, which transverses the branch anteriorly, after the vessel travels along the lateral border of the Sartorius muscle.11
Evaluation of the risk of lymphoedema
The risk of iatrogenic lower limb lymphoedema is difficult to quantify due to the paucity of cases reported. It is also confounded by the possible existence of a genetic predisposition to secondary lymphoedema.42 Vignes and colleagues reported two patients (out of 26) suffering from lower limb iatrogenic lymphoedema after inguinal lymph node harvest.43 However, no information was provided about which group and the number lymph nodes that were harvested. A case report saw ipsilateral leg lymphoedema as a complication when harvesting a lymph node-SCIP flap based on the medial branch.44
Sentinel lymph nodes in the superficial groin are mostly located at the saphenofemoral junction and the quadrant inferomedial to this (78%).45 A study that evaluated donor site lymphatic function changes after lymph node harvest in the groin recommended avoiding the lymph nodes and lymphatic vessels located under the inguinal ligament and medial to the femoral artery, and that unnecessary surgical trauma in this area should be avoided.46 Another study, in an attempt to preserve the superficial inguinal nodes, harvested lymphatic vessels from the abdomen for a chimeric SCIP flap.7 It has also been suggested that preoperative indocyanine green (ICG) lymphography could be used to identify dominant lymph nodes that should be preserved during lymph node transfer.47
Limitations
There were limitations of the SCIP flap anatomical review. In some instances, information that was not available included whether the flap was based on medial or lateral perforators, and whether pedicle dissection was down to the SCIA origin or just to the branch origin. Ideally a formal statistical analysis comparing the success rates of medial and lateral groin perforator flaps should be undertaken, but there was insufficient detail in the relevant studies to do so. In addition, heterogeneity in flap design and variability, and small study numbers precluded any meaningful qualitative analysis. Also lacking was a description and the outcomes of venous anastomosis, which would have been useful to evaluate postoperative flap congestion. Long-term outcomes of SCIP flap utilisation in the various reconstructive fields have yet to be established.
Groin perforator flap literature review summary
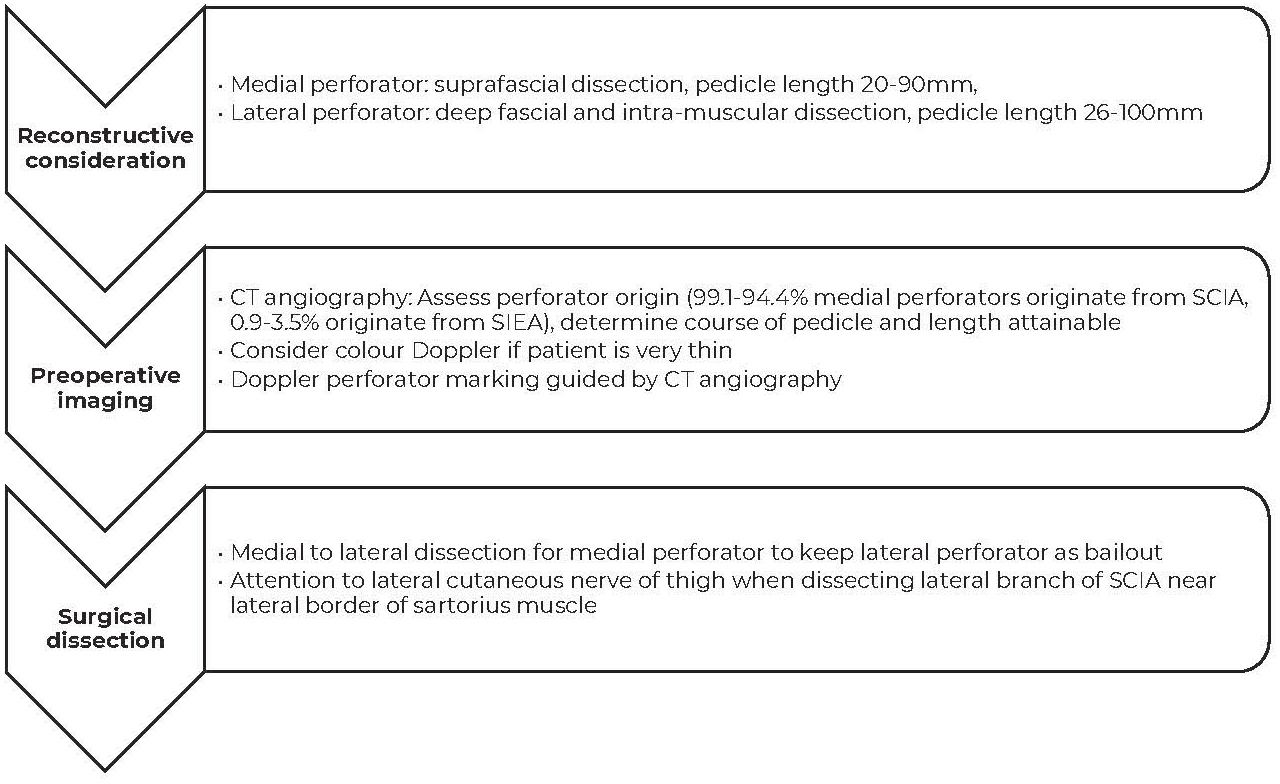
Based on the results of this systematic review, we have devised a step-wise summary (Figure 3) to the dissection of a groin perforator flap.

Conclusion
Distinct advantages for the free groin perforator flap include its thinness and concealed donor site scar. However, there remain concerns about a short pedicle length and variability in perforator anatomy. This quantitative review provides an algorithm that may grant safer flap harvest by providing strategic preoperative steps to negate the shortcomings of a potentially useful flap.
Acknowledgements
Thanks to Kaye Lirio, Medical Graphic Designer Medical Illustrations Department, Fiona Stanley Hospital, Murdoch, Western Australia for Figure 2.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.