Introduction
Lentigo maligna (LM) is a form of melanoma in situ that predominantly occurs on the exposed and sun-damaged skin of older people. It is associated with a higher incidence of local recurrence than other common melanoma subtypes.1 LM can be light brown, darker brown, black or skin-coloured and can have small clusters of melanoma cells located in a scattered fashion around the main lesion, making it notoriously difficult to define the edges of the lesion with the naked eye. Management of LM is often complicated by its large size and anatomical predilection for the face, which has significant aesthetic implications with surgical excision.
Traditionally, LM has been managed by surgical excision, with current Australian guidelines recommending 5 mm margins as adequate.1 However, topical agents such as imiquimod and radiotherapy have been implemented as alternative treatments in some centres.2 LM carries up to a 4.7 per cent lifetime risk of developing an invasive melanoma.3 Recurrences of LM often occur at the margins of previously treated areas, either as a result of inadequate surgical margins or by ‘field cancerisation effect’ in secondary procedures, as supported by Agarwal-Antal and colleagues’ findings, which demonstrated that 5 mm margins cleared less than 50 per cent of the LM lesion—92 cases excised with these margins demonstrated a clearance rate of 42 per cent at the first procedure and 69 per cent at the second procedure.3
With the aim to increase the accuracy of surgical excision margins, marking the lesion with the aid of loupe magnification, dermatoscopy and Wood’s lamp imaging have been employed. Dermatoscopy has a sensitivity of 83.2 per cent and a specificity of 85.5 per cent for melanoma.4 An alternative modality of imaging, reflectance confocal microscopy (RCM), has been found to have higher sensitivity (97.3%) and similar specificity (83%).5
Although the general principles of RCM were described by Marvin Minsky in 1957, it is only in the past decade that RCM has become a recognised emerging technique for clinical use in skin cancer. Its main advantage is that it offers a unique opportunity to evaluate skin morphology in vivo.5 This ‘virtual biopsy’ aims to avoid unnecessary excisions. While biopsies and excisions are not complex procedures, the associated morbidity and cost of histological examination are important aspects from the perspective of both the patient and the healthcare system.
To date there have been cohort studies, but no randomised controlled trials reported in the literature to inform guidelines for surgical technique or excision margins in the management of LM.4–6 Suggestions to overcome the high rates of incomplete excisions or inadequate margins include staged surgical resection or the use of Mohs surgery7; however, these procedures are labour-intensive, expensive, require a very specific level of expertise and are not generally available or recommended in Australian public hospital settings. As described above, the use of RCM may provide a non-invasive alternative to these methods.
In the current literature there are a small number of case series demonstrating the potential utility of RCM in marking the preoperative margins of LM excisions.8 The largest prospective series to date by Guitera and colleagues demonstrated that 17/29 patients with LM marked with RCM demonstrated disease > 5 mm beyond the dermatoscopy margin (which would, according to current clinical guidelines, result in an inadequate excision). They successfully demonstrated that RCM mapping changed the management in 27 patients (73%): 11 patients had a major change in their surgical procedure due to aesthetic considerations when accounting for wider margins.9
This pilot study aimed to identify the key differences in histopathological margins obtained for LM based on surgical and RCM markings performed prior to surgery on site-matched lesions. If RCM is in fact useful in identifying more widespread LM, thereby increasing the surgical margin of excision, this would be demonstrated in measurements defined as RCM excess or surgical deficits. This relative excess may also help to form future guidelines for increasing margins of excision for LM based solely on clinical markings (for hospitals where such facilities are not available), if longer term follow-up demonstrates improved rates of recurrence.
Methods
Ethics approval for the study was obtained from the research governance unit of The Alfred Hospital, Melbourne [HREC No 196/16].
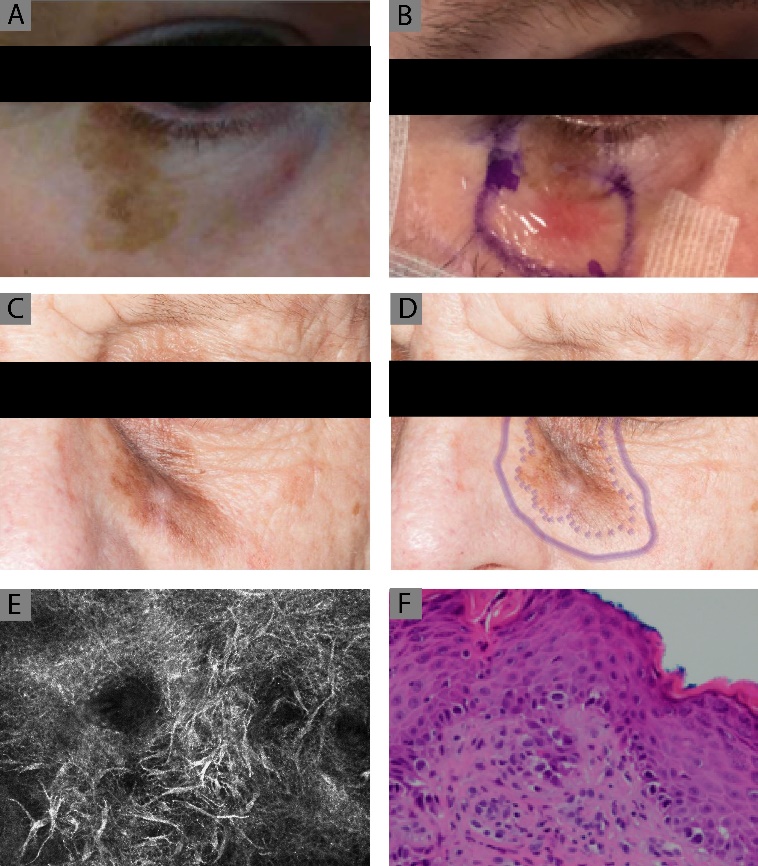
Patients were prospectively recruited from the Victorian Melanoma Service (VMS) clinic between May 2017 and May 2019. Patients with a biopsy-proven head or neck LM, amelanotic melanoma or poorly defined LM were eligible for the study (Figures 1a and 1c). Patients were placed in two groups based on the availability of RCM—Group 1, RCM-guided surgical excision, and Group 2, standard surgical excision (marked with loupe magnification in theatre). The locations of lesions on the head and neck were comparatively matched between the two groups to remove any bias due to anatomical site.
_clinical_photograph_of_a_lower_lid_lm_melanoma_which_was_biopsied_in_the_vms_clinic_after.jpeg)
Study protocol
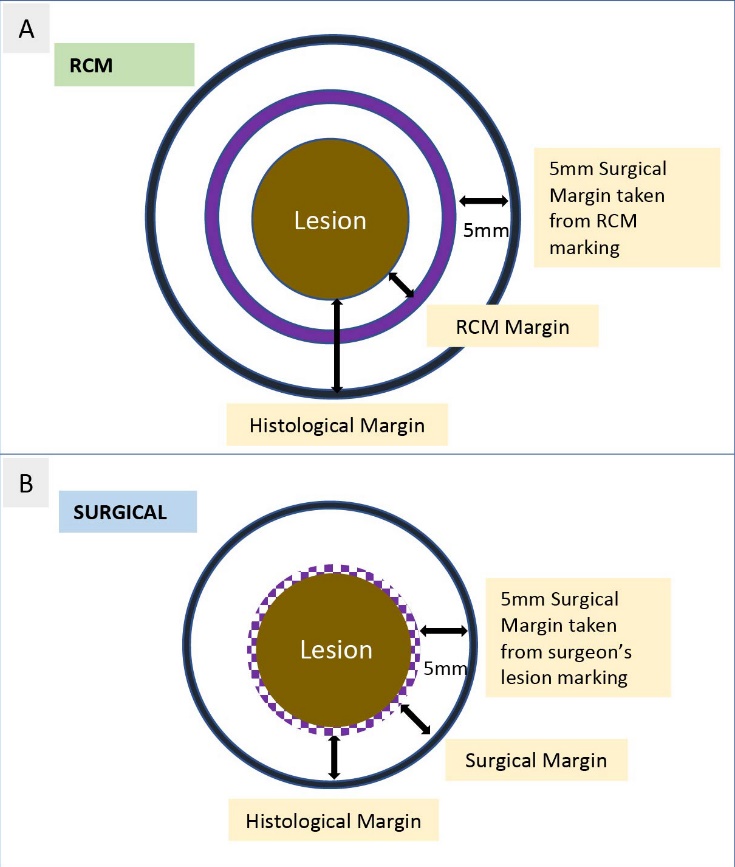
Patients were recruited by the VMS dermatology team and referred to the plastic surgical unit for surgical excision. For patients in the RCM group, a preoperative consult was organised on the day of surgery, whereby they underwent RCM assessment with a single operator and the lesion was marked and dressed (Figure 1b) (for full RCM methodology, see Rajadhyaksha and colleagues7). The 12 o’clock margin was highlighted for surgical marking and the lesion photographed with markings. Maximal dimensions at 3–9 o’clock and 6–12 o’clock were recorded on a data collection sheet. At the time of surgery, a 5 mm margin was taken from the external edge of the RCM margin (Figure 2a). A surgical suture was placed at 12 o’clock corresponding to the 12 o’clock margin on RCM marking. The excised specimen was sent fresh in a sterile container (to preserve markings) directly to the care of a single pathologist. The pathology department scored the skin markings as per the RCM to facilitate reporting of RCM excess and deficit. Figures 1e and 1f demonstrate representative samples of LM on RCM and histopathological analysis.
Similarly, patients in the standard surgical excision group were marked preoperatively by the surgical team using theatre lighting and loupe magnification (Figure 1d). The margin of the lesion was dotted and a 5 mm excision margin was formally excised (Figure 2b).
_the_lesion_was_excised_with_a_5_mm_margin_from_the_rcm_margin_(black_outline)._the_histol.jpeg)
Analysis
The expected histopathological margin for the RCM group was deemed as 5 mm from the RCM marking with anything < 5 mm reported as a deficit and > 5 mm reported as an excess. In addition to this analysis, a further measurement of surgical markings was taken and defined as RCM excess or deficit (Figure 2a). The expected histopathological margin for the surgical group was deemed as 5 mm, with anything < 5 mm reported as a deficit and > 5 mm reported as an excess (Figure 2b). Statistical analyses were performed using Student’s t test (GraphPad Prism, USA).
Results
Patient and lesion demographics
Seven patients were recruited for RCM marking of their LM during the study period. This group was directly compared with seven anatomical site-matched surgically marked patients. The average age of patients in the surgical group was 68 years vs 73 years in RCM group (Table 1). The average dimensions of the RCM-marked excisions were 3574 ± 1274 mm3 and the surgically marked excisions were 3113 ± 711 mm3, three with the difference demonstrating a trending increase in the confocal group that did not reach statistical significance.
RCM marking and surgical excisions
The aim was to report four margins (3, 6, 9 and 12 o’clock) per specimen for the seven RCM-marked and seven surgically excised lesions. However, during the processing of these fresh specimens 5/28 RCM margins were not able to be accurately determined, so 23/28 were presented.
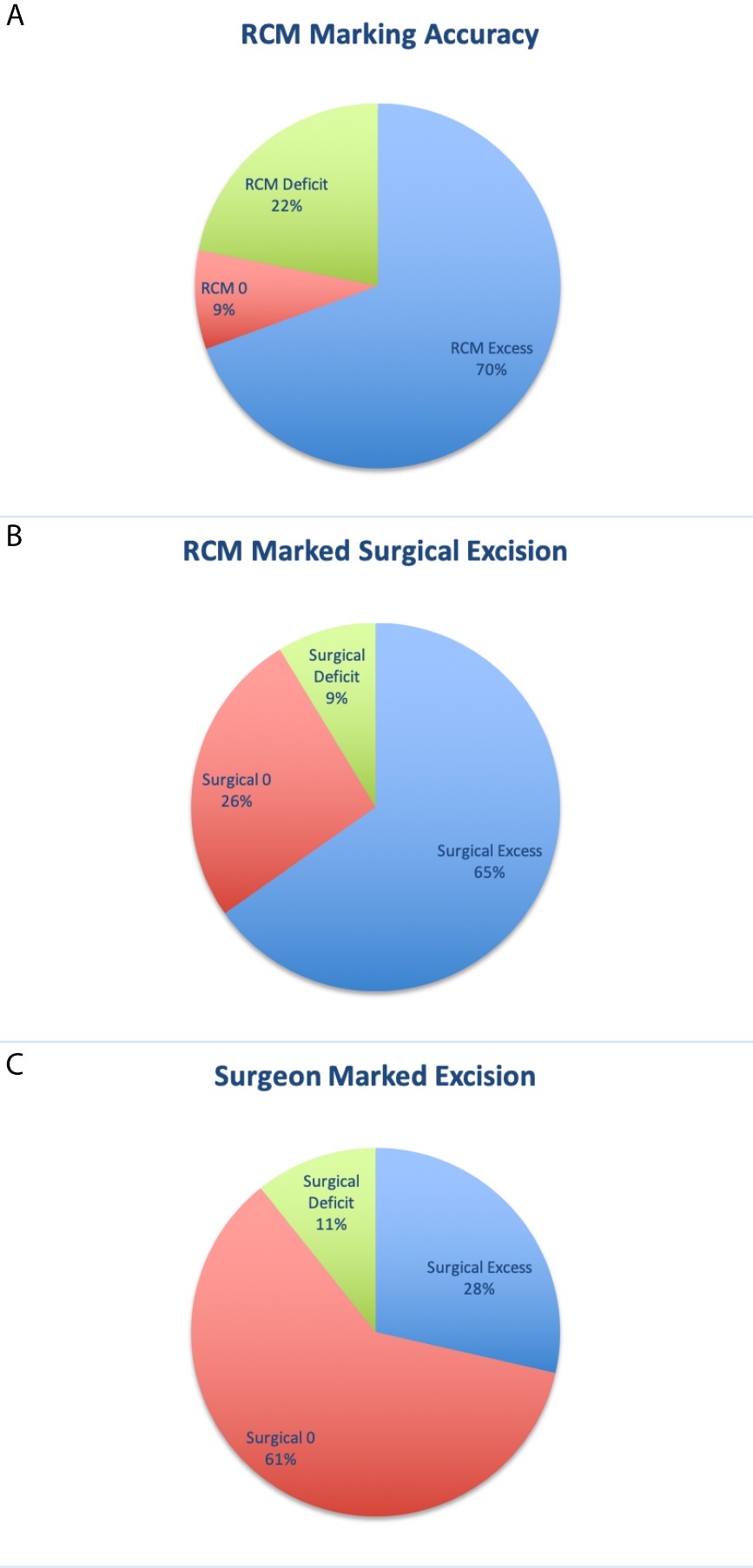
The results in the RCM group were analysed to assess (1) the accuracy of the RCM marking in identifying lesion boundaries and (2) the margins achieved on surgical resection based on the RCM markings. RCM marking of the lesion was found to be in excess in 69 per cent of margins, resulting in a mean RCM lesion excess of 3.09 ± 0.58 mm. RCM marking accurately defined the lesion in 9 per cent and was found to be deficient in 22 per cent, with an average RCM lesion deficit of 2.10 ± 0.52 mm (Figure 3a).
A 5 mm margin was measured from the RCM marking to perform the surgical excision. Based on these preoperative measures the expected histological margins were 6.70 ± 0.62 mm; however, the actual histological margins obtained were 7.82 ± 0.66 mm in the RCM-marked surgically excised group. Surgical excision of RCM-marked lesions was found to be in excess in 65 per cent of margins, with an average surgical excess of 1.9 ± 0.32 mm. It was accurate in 26 per cent of margins and deficient in 9 per cent of margins by an average of 1.25 ± 0.25 mm (Figure 3b, Table 2), resulting in one patient requiring re-excision to obtain adequate margins.
Surgically marked excisions
There were four margins (3, 6, 9 and 12 o’clock) per specimen reported for the seven surgically excised lesions. On average a histological margin of 5.70 ± 0.36 mm was achieved across all excisions. The expected surgical margin for all lesions was determined as 5 mm as per the documented measures on the operative note. For the seven lesions, 28 per cent of margins reflected a surgical excess with an average of 3.0 ± 0.76 mm, 61 per cent were accurately excised to obtain a 5 mm histological margin and 11 per cent were deficient, resulting in an average surgical deficit of 1.50 ± 0.50 mm (Figure 3c, Table 2) and resulting in one patient requiring re-excision to obtain adequate margins.
__accurate_(red)_and_de.jpeg)
Comparison
Analysis of margins comparing RCM-marked and surgically marked excisions demonstrated a significantly greater histopathological margin in the RCM group of 7.82 ± 0.66 mm (6.45–9.18 95% CI) vs 5.70 ± 0.36 mm (4.96–6.44 95% CI) (p = 0.0045).
Discussion
Facial LM presents multiple challenges in management, from diagnosis to marking the surgical excision margins, obtaining histopathological clearance and monitoring for recurrence. Cotter and colleagues conducted a study where LM was treated with topical imiquimod therapy applied 2 cm peripherally around the lesion. In this cohort, 90 per cent of recurrences were detected at the edges of the topical field, at times > 2 cm wider than the macroscopically visible lesion.2 Reported rates of recurrence at these typically indistinct borders of LM can be between 6 and 20 per cent.10–13 These particular findings demonstrate the nature of LM and the difficulties that can be encountered with preoperative marking and incomplete or inadequate excision margins, particularly in cosmetically sensitive areas such as the head and neck. This pilot study aimed to overcome some of these challenges by incorporating RCM (a non-invasive tool) to aid in preoperative surgical marking of LM in the head and neck region to obtain clear histological margins.
Lesion sites were matched between the RCM and surgically marked groups with the aim of reducing any discrepancies that resulted from difficult anatomical resections in the head and neck region. The study looked at the accuracy of RCM in identifying the borders of a LM compared with a surgically marked LM. The RCM group demonstrated 78 per cent adequate clearance of the lesions (69% excess and 9% accurate margins) but RCM was deficient in 22 per cent. This excess is largely attributed to confocal microscopic features of cells deemed ‘atypical’, lying outside the macroscopic margins of the lesion, thereby extending the marked lesion margin. However, the clinical relevance of including these atypical cells with histopathological clearance is yet to be determined. Surgical excision of RCM-marked lesions demonstrated 91 per cent adequate clearance of lesions with an acceptable margin of at least 5 mm (65% excess and 26% accurate margins), being deficient in 9 per cent of margins. Similar results were reported by Pellacani and colleagues, where RCM was unable to accurately mark the lesion in 9 per cent of cases; however, they reported a complete histopathological clearance in cases they deemed suitable.14 The surgically marked excision group demonstrated 89 per cent adequate clearance of lesions with an acceptable margin of at least 5 mm (43% excess and 46% accurate margins) and was deficient in 11 per cent of margins. Therefore, while the overall margin of at least 5 mm was obtained in both groups at a comparable rate, the surgical group obtained this with less excess and more accuracy. These rates are similar to those described by Kunishige and colleagues, who found in a cohort of 1500 LM patients that a 79 per cent clearance rate was achieved with a 6 mm margin.11
Surgically excised lesions achieved an average histological margin of 5.7 ± 0.36 mm compared with an average of 7.83 ± 0.66 mm for RCM-excised lesions. The recommended guideline for excision of LM and other melanoma in situ subtypes is still 5 mm,1 recognising that this margin might be inadequate in up to 50 per cent of lesions.3 No studies to date have specifically looked at routine margins > 5 mm, but several make recommendations to increase the margins from 5 mm to 10 mm for large indistinct, positive post-primary excisions or recurrent lesions.10–13
It is critical to note that LM is an in situ disease. Although it is a precursor for invasive disease (with a 4.7% rate of progression to invasive disease), it is rare to develop metastatic spread from the in situ form. Therefore, treatment should aim to excise the lesion completely with clear histological margins. The population of patients in this study with head and neck LM presented with lesions that were in cosmetically sensitive areas. Margins in excess of the recommended 5 mm might have resulted in increased distortion of soft tissues not amenable to direct closure and warranted more complex reconstruction with local flaps or grafts. Without evidence of a clear therapeutic benefit resulting from an excision > 5 mm, the RCM excess followed by confocally marked surgical excess might contribute to larger excisions, larger defects and more complex reconstruction with no additional oncological advantage.
This study does have certain limitations. Firstly, it is a single-centre trial and the number of patients enrolled was low. Secondly, the investigator performing RCM, the surgeons marking the surgical excisions and the pathologists examining the specimens have extensive experience and, as a result, it may not be possible to generalise these results to other services. Determination of a clear histopathological margin in LM can also prove challenging—Florell and colleagues demonstrated only moderate concordance of opinion between pathologists and found margin determination was aided with the addition of a control strip of tissue.15 Thirdly, on further analysis, if the surgical excisions between the two groups are compared, the RCM-marked surgical excision margins demonstrate an increase in surgical excess and a drop in surgical accuracy. This may be accounted for by an unconscious bias to excise widely based on the macroscopic RCM markings, which were, as shown in Figure 1b, often beyond the pigmented edge of the lesion. In terms of patient management, however, only one patient per group required further excision to obtain adequate margins. Fourthly, this is a pilot study that demonstrates some meaningful early findings which require further validation in a larger scale prospective randomised controlled trial. Lastly, the wider histopathological margins obtained as a result of RCM-marked lesions could reflect improved oncological control and lead to reduced recurrence, but to reliably draw such conclusions longer term follow-up is required. This is also lacking in the current literature.
Conclusion
Experienced surgeons, optimal lighting and loupe magnification in this small series have demonstrated accurate marking and excision of LM in the head and neck with predominantly optimal margins and accuracy. Larger randomised controlled trials may demonstrate the benefits of RCM, but at this stage this pilot study does not demonstrate a clear benefit for use of RCM in a routine setting.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Disclosure
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship and/or publication of this article.
Revised: December 20, 2019 AEST