
Introduction
Postoperative management of lower leg split-thickness skin grafts (SSGs) has traditionally involved the use of bolster-style dressings and immobilisation of the patient for five to 10 days before the patient resumes ambulation. However, evidence suggests that such prolonged bed rest provides no significant improvement in graft take or overall patient outcomes and increases the risk of venous thromboembolism (VTE),1–3 as well as reducing mobility4,5 and increasing the risk of deconditioning. This adversely affects patients and generates a significant burden from the health costs associated with prolonged hospitalisation.4 Despite this evidence showing advantages in early mobilisation, in the literature there is a paucity of information as to whether early mobilisation is actually implemented in practice.
Negative-pressure wound therapy (NPWT) has become a useful option in the armoury of dressings for SSGs. Several studies have shown NPWT to improve the rate of graft success,6 improve qualitative graft take7,8 and reduce the need for repeat grafting9 when compared with standard dressings when used as a graft bolster or fixation. Specifically, NPWT reduces graft lift-off secondary to oedema or haematoma, and actively removes exudate.10 NPWT improves the tissue-to-graft interface immobility and conforms to irregular surfaces, thus providing a secure bolster to prevent shearing of the graft, which is particularly useful for limb wounds.10,11 Conversely, other studies report no improvement in graft take with NPWT (as shown later in Table 2).
There are many reasons for surgeons to resist change. Cabana and colleagues reviewed 76 papers and found multiple barriers to change including lack of awareness, familiarity with current methods and inertia to change, lack of agreement and self-efficacy, and absence of external barriers to perform recommendations.12 Changing clinical practice in line with up-to-date literature is a slow process, with the time lag from evidence to practice estimated at 17 years.13,14 Clinicians are slow to take up new practices but they are even slower to eliminate entrenched practices that have lost value or been replaced by improved treatments.15,16
The aim of this study was to evaluate the practice preferences of Australian plastic surgeons for dressings and postoperative protocols after lower limb SSGs, and to evaluate whether these practices have changed over a five-year period and whether their practice was in line with current evidence recommendations.
Methods
Current trends in postoperative management of lower limb SSGs by Australian plastic surgeons were investigated electronically by inviting members of the Australian Society of Plastic Surgeons (ASPS) to participate in a questionnaire regarding their postoperative regimens for lower limb SSGs. This survey was performed in 2013 and repeated in 2018 using the electronic platforms Surveymonkey® and Google Forms, respectively. A literature review was performed to establish whether surgeon-reported practice was in line with current evidence for early mobilisation of lower limb SSG and also for NPWT on SSG. Searched databases included MEDLINE® (1950–2019), EMBASE (1980–2018), PubMed and Cochrane Database of Systematic Reviews.
Statistical analysis was performed using STATA v14 (StataCorp LP, Texas, USA). Data were analysed using 𝜒2 analysis and logistic regression. Statistical significance required p < 0.05.
Analysis
A total of 311 survey invitations were sent to current members of ASPS in 2013, and 119 (38%) completed responses were received. This survey was repeated in 2018 with 110 (35%) responses received. The proportion of ASPS members who responded to the survey in 2018 was not statistically significantly different from that in 2013 (p = 0.51).
Rate of NPWT use in 2013 compared with 2018
The proportion of respondents who used NPWT over the five years did not change significantly (p = 0.33 by 𝜒2 test), as summarised in Table 1. In both surveys, those surgeons who answered that they never use NPWT for a skin graft to the leg, 36 (30%) in 2013 and 29 (26%) in 2018, were asked to bypass all questions regarding NPWT thereafter. The remainder of respondents used it intermittently, with only a small percentage always using it. Of the surgeons who responded that they used NPWT, 67 per cent in 2013 and 72 per cent in 2018 felt that SSGs did better with NPWT. Reasons given for a better outcome were that the grafts were splinted and conformed to the wound bed better, especially over joints or complex wound beds, allowing earlier mobilisation; and that the grafts were better at managing exudate with less risk of seroma and haematoma, along with earlier revascularisation of the SSG resulting in better initial graft take.
Contact layer with NPWT dressings
The choice of contact layer was similar in both survey responses with approximately 38 per cent of surgeons using paraffin-impregnated gauze and about 34 per cent using a silicone net such as Mepitel®. Other dressings used included silver mesh such as Acticoat® and other non-adherent dressings such as Adaptic® and Cuticerin® (Table 1).
Contact layer with standard dressings
For standard dressings, paraffin-impregnated gauze was used by more than 70 per cent of respondents. The next most popular contact dressing was a silicone net such as Mepitel® (Table 1).
First dressing change
The first dressing change was consistently earlier when a NPWT dressing was used. In the NPWT group in 2013, 65/79 (83%) dressings were changed at or before day five postoperatively versus 72/111 (65%) in the standard dressing group (p = 0.01). In 2018, 62/80 (78%) of NPWT were changed on or before day five compared with 66/110 (61%) in standard dressing group (p = 0.01).
Immobilisation with NPWT and standard dressings
Surgeons reported immobilising their patients longer with standard dressings than with NPWT dressings (p = 0.003 by multinomial logistic regression). Respondents immobilised 26 per cent of NPWT patients for more than 48 hours compared with 55 per cent of standard dressing patients in 2013, while the figures for 2018 were 22 per cent and 44 per cent, respectively. In the NPWT group, compared with the standard dressing group, significantly fewer patients were immobilised for three to five days postoperatively (p = 0.016 by multinomial logistic regression) and for more than five days (p = 0.001 by multinomial logistic regression). In 2018, significantly fewer patients were immobilised for more than five days than in 2013 for both dressing groups (p = 0.005 by multinomial logistic regression). This alteration in surgeon behaviour is especially apparent in the standard dressing group, with a reduction in immobilisation for more than five days from 30 per cent to 9 per cent over the five years occurred (p = 0.001). This is summarised in Figure 1.

Hospital stay with NPWT vs standard dressings
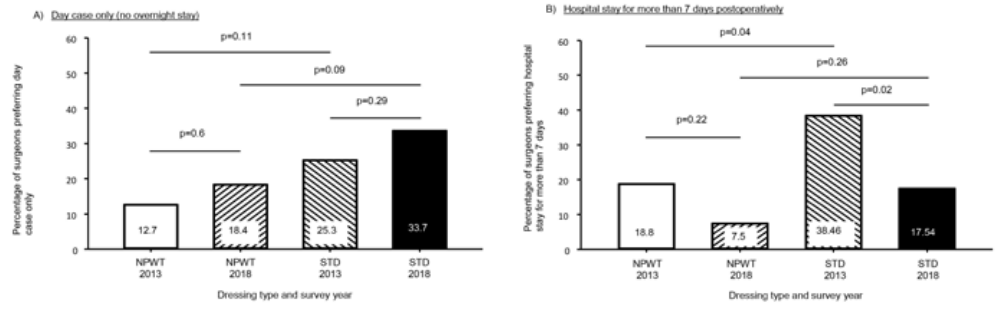
In both 2013 and 2018, surgeons were more likely to treat patients with standard dressings as day cases than those with NPWT, although this was not statistically significant (Figure 2a and b). Conversely, there were more overnight stays when NPWT was used compared with standard dressings. Significantly more surgeons preferred a hospital stay of more than seven days with standard dressings (38.5%) than with NPWT (18.8%) in 2013 (p = 0.04). There was a subsequent significant reduction in the length of stay for standard dressings between the surveys, reducing from 38.5 per cent in 2013 to 17.5 per cent in 2018 (p = 0.02). Hospital stay preferences are summarised in Figure 2a and b.

Deterrents for NPWT use
The most commonly selected deterrent to NPWT was high cost, with 65.9 per cent of surgeons (56/85) choosing this option in 2013 and 63.2 per cent (55/87) choosing it in 2018 (p = 0.92 by 𝜒2 test). Other reasons included difficulty with application, difficulty with removal, satisfaction with their current technique with no reason to change, the NPWT unit was too bulky for patients to move around, belief that NPWT results were not any better and belief that NPWT results were actually worse (4 of 86 responses in 2013, 6 of 87 in 2018). Belief that NPWT results were not any better and belief that NPWT results were actually worse did not significantly change from 2013 to 2018 (p = 0.76 by 𝜒2 test).
Discussion
Early mobilisation following lower leg SSG
The current literature shows significant evidence that early mobilisation after SSG to the lower leg reduces potential harm and reduces costs.
Chilvers and Freeman first described successful lower leg skin grafting without postoperative immobilisation in 1969.17 This observational study of skin grafts for chronic venous ulcers to lower limbs included 25 patients, 23 of whom had successful initial graft take while two had immediate failure due to infection. All patients were mobilised postoperatively. A retrospective review by Bodenham and Watson in 1971 recorded three SSG failures due to seroma or haematoma from a total of 25 patients who underwent immediate mobilisation postoperatively.18
Evidence for early mobilisation was further supported in 1993 by Budny and colleagues, who conducted a randomised controlled trial (RCT) comparing immediate mobilisation with bed rest.4 Twenty-one cases of pretibial injury requiring SSG were immediately mobilised compared with 40 cases that required SSG and seven days bed rest. There was no significant difference in graft take or overall complications between the two groups. The percentage area of graft take was not statistically significantly different at one week (93.7% with bed rest compared with 88.7% having early mobilisation, p = 0.29) or at three weeks post-surgery (92.8% having bed rest compared with 89.7% having early mobilisation, p = 0.55). However, the length of hospital stay was much longer in patients who underwent bed rest compared with those who had early mobilisation (average 12 days versus two days). This study also reported the deconditioning of patients who underwent bed rest as a patient-reported outcome measure. Deconditioning was reported in 32 per cent of patients who underwent bed rest compared with 0 per cent of patients who underwent immediate mobilisation.
Wallenberg randomised 50 consecutive patients undergoing SSG to lower limb to either early mobilisation or four days bed rest.19 Blinded clinicians found no statistically significant difference in graft take at day 14 post-surgery.
A systematic review by Smith provided a thorough overview of evidence for early mobilisation.20 Smith concluded that patients should begin walking immediately or at the earliest possible opportunity after lower extremity SSG surgery.
Luczak and colleagues reported outcomes from 48 cases of SSG retrospectively reviewed.5 Outcomes reported showed no difference in graft take between patients who underwent early mobilisation (≤ 3 days bed rest) compared with patients who had late mobilisation (≥ 4 days bedrest), where p = 0.43. However, significant benefits of early mobilisation were identified in this study: those patients who had early mobilisation had significantly less deconditioning and reduced hospital length of stay (p = 0.008).
Southwell-Keely and colleagues performed a meta-analysis comparing early mobilisation and bed rest following SSG to the lower leg.21 This study analysed the outcomes from all available RCTs and prospective cohort studies. From the studies included, 70 cases had undergone early mobilisation and 93 had undergone bed rest. There was no difference found in graft healing at seven or 14 days post-procedure (odds ratio = 0.74). There was also no difference noted in postoperative complications.
Thus, there is a long history of strong evidence for the benefit of early mobilisation whether with standard dressings or NPWT. Our results showed that current postoperative management of lower leg skin grafts among Australian plastic surgeons has improved to better reflect current evidence and recommendations, but there are still a significant number of surgeons who routinely maintain patients in bed postoperatively. Even accounting for the reported 17 years for clinician practice to change to reflect evidence,13,14 surgeons still order postoperative bed rest despite 50 years of evidence to the contrary.
The reason behind lack of early mobilisation in the standard dressing group was not evaluated in the current survey and requires further study. We can only state at this stage that we have defined a link between NPWT and an increased tendency to allow early mobilisation. The evidence and surgical experience support that with NPWT there is better immobilisation of the graft, especially over joints or muscles, with fewer shear forces and so allowing earlier mobilisation.
NPWT for SSG
The use of NPWT for SSGs has been described extensively in the literature since its introduction by Argenta in 1997.22 There are many reports on its use and its perceived benefits but there are few prospective randomised controlled trials (PRCTs).6,7,23–25 A systematic review and meta-analysis by Yin and colleagues in 2018 was able to identify only seven PRCTs and five cohort studies that were suitable for analysis.26 Their analysis showed a seven per cent improvement in SSG take with NPWT compared with standard dressings (p < 0.0001) and a concomitant reduction in the need for a regrafting procedure (RR 0.28, 95% CI 0.14–0.55, p = 0.0002). There was no significant difference in infection rates between the treatment groups. Randomised controlled trials and cohort studies comparing graft take after SSG in NPWT compared with standard dressings are summarised in Table 2 with all, save Leclercq and colleagues,27 showing improved graft take with NPWT when used in acute and chronic wounds but not with free flap donor sites. Other advantages have been noted in regard to reduced time to total healing,6,23,28,29 reduced re-grafting procedures,30–32 reduced length of hospital stay30 and reduced infection rate.33
The free radial forearm donor site has been studied by multiple groups (Table 2).34–38 The majority of these studies do not show a significant improvement in graft take, though other advantages have been reported including improved early function.36 A similar result is seen with the donor area for a free fibula flap, with two studies showing no significant difference in graft take.25,28 Bach28 and Clark36 did, however, find a significantly shorter healing time in the NPWT group—67 days compared with 163 in the bolster dressing group (p < 0.02). Kim used a one-stage Alloderm and SSG procedure comparing NPWT with standard dressings and achieved significantly better results.6 Most of these studies are limited by being small series and are underpowered to show a significant difference.
An International Expert Panel on NPWT published guidelines in 2011.39,40 The panel recommended consideration of NPWT to improve the rate of graft success (grade A recommendation), and that NPWT be considered in wounds/patients with high risk of graft loss (grade B recommendation).40 They recommended that NPWT should be left undisturbed for three to seven days post-grafting SSG (grade B recommendation).40 NPWT has also been shown to reduce costs compared with conventional wound therapy through reduced use of nursing resources and improved patient outcomes.39
Azzopardi and colleagues reviewed the literature investigating the use and mechanism of action of NPWT over skin grafts.8 All included articles were reviewed according to level of evidence, allowing graded recommendations to be made accordingly. Firstly, they proposed that increased microcirculatory flow and angiogenesis stimulation may be attributed to NPWT (grade C evidence). Secondly, they stated that complications such as graft lift-off by oedema or haematoma and graft sheering were significantly improved compared with standard dressings (grade B evidence). Most significantly, they found that NPWT promoted qualitative improvement in the final SSG result studies (level 1B).8
Despite the evidence supporting NPWT use for SSGs, in our study 33 per cent (2013) and 26 per cent (2018) of Australian plastic surgeons reported never using NPWT for SSGs on the lower limb. Our survey identified many deterrents that prevent surgeons from instituting NPWT into everyday practice, despite the majority of those who use NPWT feeling that SSGs do better with NPWT. Cost has always been a major reason preventing the use of NWPT by surgeons. However, from this study significantly fewer patients are hospitalised for more than seven days when NPWT is used compared with standard dressings. Prolonged hospital stays in Australia are in the order of $1800 per day compared with NPWT costs of $180 per unit per day, thus a major cost saving can be achieved, with reduced inpatient costs outweighing any rental cost/consumables associated with NPWT.
In Australia, the funding of NPWT for patients in the community setting relies on funding from the public hospital system. Many private health funds will not fund the unit outside the hospital environment. This may be a major deterrent to the routine uptake of NPWT and may explain why day case patients are given standard dressings over NPWT. The different rates of NPWT use in the public versus private setting are multifactorial and outside the scope of this study.
It was unclear why significantly more surgeons reported preferring a hospital stay of more than seven days with standard dressings than with NPWT in 2013. The length of stay is principally determined by the patient’s mobility, their social support network and, if using standard NPWT, the funding of the unit.
Many deterrents to NPWT use will persist, such as surgeon preference regarding technique and perceived success with their current protocol. Other deterrents rely on future advancements of the technology. For example, many surgeons cited the bulkiness of the NPWT units as a deterrent, but new low-profile NPWT units are available that should reduce these concerns. In 2018, 49 per cent of surgeons used these smaller units in some of their cases, but they are limited by the size and depth of wound they may be used on. Several studies suggest a benefit from NPWT but multiple studies also show no benefit. This is reflected by the diversity of management protocols followed by Australian plastic surgeons.
Conclusion
The rate of postoperative early mobilisation of lower leg SSGs by Australian plastic surgeons improved from 2013 to 2018 to better reflect current evidence, but a significant number of surgeons continue to maintain patients routinely in bed postoperatively. There is a link between NPWT use and an increased tendency to early mobilisation. The most common stated deterrent to NPWT use is cost, despite evidence supporting NPWT as more cost-effective than standard dressings.
Acknowledgements
We acknowledge Peninsula Health Department of Surgery Research Co-ordinator Dr Vicky Tobin for statistical assistance and Professor Warren Rozen for editorial assistance.
Disclosure
The authors have no conflicts of interest to disclose.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Revised: June 26, 2020 AEST