



Introduction
Medication-related osteonecrosis of the jaw (MRONJ) is a recognised complication of anti-resorptive and anti-angiogenic therapies. The incidence of MRONJ appears to vary by mode of administration: high-dose parenteral agents used in the oncology setting have an incidence of one per cent,1,2 whereas oral agents used to treat osteoporosis pose a significantly lower risk (0.001–0.2%).3,4 Medication-related osteonecrosis of the jaw is defined clinically as exposed bone in the maxillofacial region, for a minimum of eight weeks, following recent or previous treatment with anti-resorptive or anti-angiogenic agents and no history of maxillofacial radiotherapy.5 Staging of disease involves assessment of surrounding tissue and extent of bony deficit. This disease is characteristically difficult to treat due to its debilitating symptoms and high relapse rate. Symptoms include pain, swelling, purulent discharge, halitosis, masticatory dysfunction and neurosensory deficit.2
The most recent 2014 American Association of Oral and Maxillofacial Surgeons position paper advises limited surgery involving local debridement with the aim to promote soft tissue healing over exposed bone.2 Radical surgery including elimination of all necrotic bone and soft tissue coverage is advised only for symptomatic patients with extensive MRONJ who have failed conservative treatment, with the aim of palliation of infection and pain, generally without consideration of cure.2
We proposed a shift from this standard of care whereby advanced MRONJ (stage II and above) is treated with excision of necrotic bone and reconstruction of residual defect with either local flap or periosteal forearm free flap coverage as appropriate. We hypothesised that this overall approach may halt disease progression more effectively than conservative dental measures alone. We further hypothesised that vascularised periosteal radial free forearm flap (RFFF) reconstruction to cover bone defects may promote new bone formation and prevent progression to pathological fracture.
Reliability of nasolabial flap reconstruction for soft tissue closure post-decortication in MRONJ patients has been previously described.6,7 Although composite vascularised periosteal RFFF have been described for the treatment of early mandibular osteoradionecrotic injury,8 our paper is the first description of its use for MRONJ.9
The aim of this pilot study is to describe the outcomes of advanced MRONJ managed with vascularised periosteal RFFF, local nasolabial flaps and conservative dental measures at a single institution over a 4.5-year period. The aim was to measure the outcomes of advanced MRONJ managed within these three treatment groups. The primary outcome measure was clinical evidence of healing at six months after initial treatment. Secondary outcome measures included radiological evidence of healing at six months as well as patient satisfaction.
Methods
This study was approved by the Alfred Hospital Institutional Ethics Review Board [611/18]. The investigators designed and implemented a retrospective comparative case series. The study sample was derived from the population of patients who presented to the Alfred Hospital for the evaluation and management of MRONJ between 1 January 2014 and 30 June 2018. Subjects eligible for study inclusion had MRONJ stage II or above and consented for enrolment. Included subjects were managed with either conservative dental measures, local flap reconstruction or periosteal free flap reconstruction. Specific dental measures included antibiotics, hygiene rinses and/or local debridement. Subjects managed with non-periosteal free flap reconstruction such as free fibula flap were excluded. Patients were found by searching the hospital database of discharged patients with diagnosis codes ‘inflammatory conditions of the jaw,’ ‘other secondary osteonecrosis’ and ‘agents affecting calcification adverse effects of treatment use’. Medical record review was then performed. The primary outcome of interest was ‘clinical recovery’ defined as symptomless and closed wound after six months (yes/no). The secondary outcome of interest was ‘radiological evidence of disease control’ defined as (1) improved: increased bone with defined sclerotic margins, (2) mixed: interval bone loss at site of previous debridement but well-defined sclerotic margins or (3) worsened: bone loss with ill-defined bone lucency. A single senior radiologist blinded to treatment modality performed the analysis of pre- and post-treatment imaging. Patient satisfaction six months post-treatment was collected with a standardised telephone survey. Results were analysed descriptively.
The vascularised periosteal RFFF is a technique yet to be described for management of MRONJ. The technique followed at our institution is as follows:
Preoperative planning is essential. We would normally harvest from the non-dominant forearm. Allen’s test was performed to verify ulnar vascularisation of palmar arch. Reverse Allen’s test was also performed to make sure the radial artery was patent. The fascio-cutaneous paddle was defined, centred on the radial vascular pedicle; however, the final paddle was not finalised until after initial exploratory incision to ensure the septal perforators were centred within the flap. This is especially important for this small flap with few perforators. A superficial draining vein was included in the flap. Cutaneous branches of the superficial radial nerve were preserved. The brachioradialis muscle tendon was retracted then radial periosteum incised with length corresponding to the slice of mandibular bone section to be resurfaced. The periosteum was gently elevated to avoid it dissociating from the radial vascular pedicle. The ulnar surface of the flap was secondarily dissected up to the tendon of flexor carpi ulnaris which was retracted to allow exposure of the lower end of the radius. The entire periosteum was released until the opposite detachment zone was reached. The distal end of the radial vascular pedicle was dissected, then ligated. The best draining veins were selected, conventionally one superficial and one vena commitans. The composite flap periosteum was inset first followed by the skin paddle and finally the anastomosis.
Results
A total of 10 patients were included in this series: six were female and four were male. The mean age of patients at the time of first treatment for MRONJ was 67 years (range 54–82 years). The most common class of drug was the bisphosphonates (8/10), followed by denosumab (1/10) and the mTor inhibitor everolimus (1/10). Indication for these medications included multiple myeloma (5/10), osteoporosis (4/10) and renal transplant (1/10). Seven patients were classified with stage 2 MRONJ and three patients were classified with stage 3. Initial symptoms on first consultation included pain (5/10), non-healing tooth extraction site (3/10), fistula (1/10) and mobile teeth (1/10). One patient was asymptomatic. Patient demographics and their outcomes according to treatment are summarised in Table 1 and Table 2.
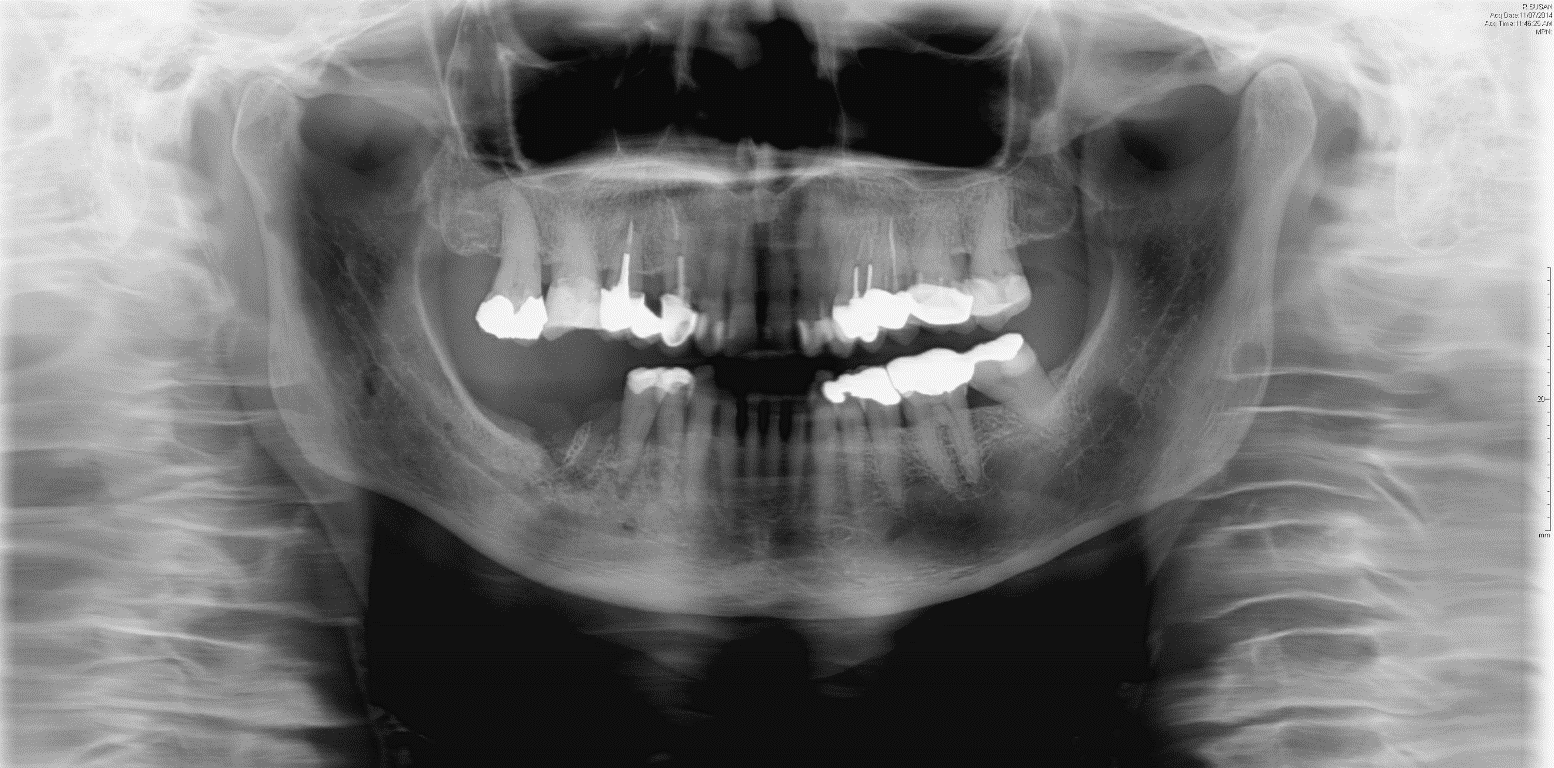
Four patients were managed with dental measures alone involving local debridement. Nasolabial flap reconstruction was selected for three patients. Vascularised periosteal (RFFF) reconstruction was selected for three patients. Patients were generally selected for local nasolabial flap reconstruction if the area of exposed bone was small and located in the maxilla or patients were deemed high risk for more complex longer surgeries due to comorbidities. Patients were selected for free periosteal forearm flap reconstruction if the area of necrotic bone was large, located in the mandible and if there was significant bone loss posing high risk for pathological fracture if disease were to progress (Figure 1). There were no postoperative complications recorded for the nasolabial flap or the RFFF patients.

All six patients selected for flap reconstruction demonstrated asymptomatic wound healing at six months post-reconstruction (Figure 2). In contrast, only one of four patients managed with dental measures were healed and symptom free at six months. The other three patients had ongoing pain, discharge or residual soft tissue defect.

Radiologically, three of the four patients managed with dental measures showed a mixed picture of increased bone loss at the site of previous debridement but with well-defined sclerotic margins at six months follow-up. The other of these four patients had two foci of MRONJ in the maxilla and mandible. The maxilla showed worsening bone erosion while the mandible showed sclerosis. Of the three patients selected for nasolabial flap, one demonstrated a mixed picture of interval bone loss but with well-defined sclerotic margins, one demonstrated an improved picture with increased bone and sclerotic margins and one patient did not undergo postoperative imaging. Due to symptom-free recovery, this patient did not consent to follow-up imaging. All three patients selected for RFFF demonstrated an improved radiological picture with increased bone deposition and well-defined sclerotic margins (Figures 3, 4, and 5).



Only one of four conservatively managed dental patients reported patient satisfaction at six months post treatment while all patients managed with flap reconstruction reported that they were satisfied.
Discussion
There is no consensus regarding the definitive management of MRONJ, especially for advanced stages of the disease (stages II and III); as such, there are no international standardised guidelines. The purpose of this case series was to describe preliminary comparative outcomes for advanced MRONJ managed with conservative dental measures, local nasolabial flap reconstruction or vascularised periosteal RFFF reconstruction. The results of this preliminary series support our hypothesis that complete excision of necrotic bone followed by reconstruction of defect with either local nasolabial flap or periosteal forearm free flap may halt disease progression more effectively than conservative dental measures alone. The results support the secondary hypothesis that vascularised periosteal RFFF, a novel technique for MRONJ management, promotes new bone formation and may prevent progression to pathological fracture.
Surgical resection and vascularised bone reconstruction in MRONJ has been trialled in multiple studies. To date, vascularised free fibula transfer has been the most prevalent approach for advanced disease with pathological fracture.10,11 The use of this technique has been limited by significant concerns over non-union at the fibula-mandible fixation sites, occurring at a rate of 6.5 per cent,12 impaired fracture healing in MRONJ-affected bone13 and recurrence of osteonecrosis at the site of reconstruction.14 The vascularised periosteal RFFF is a technique that has yet to be described for management of MRONJ. This flap was originally proposed as a fascio-periosteal variant for optimal vascularisation of maxillary bone grafts in the trauma setting.15 Roselli and colleagues then described a radial periosteal fascio-cutaneous free flap with frozen autologous mandibular bone for mandibular reconstruction.16 More recently, Bettoni and colleagues described a technique for harvest of a periosteal forearm composite free flap in the treatment of mandibular osteoradionecrotic injury.8 Our approach of using a segment of vascularised periosteum to cover mandibular defects provides a number of key benefits over previously reported surgical approaches for MRONJ. First, the aim of our intervention was to prevent pathological fracture development and thus represents an early intervention when compared with free fibular transfer. Second, evidence of new bone formation has not been reported with other methods of soft tissue coverage for MRONJ; therefore, vascularised periosteal radial forearm flaps illustrate the possibility of disease reversal as a new dimension in treatment. This is theoretically based upon the osteo-inductive and osteogenic activity seen with other vascularised periosteal free flaps (medial femoral condyle and others).17–19 It is believed that the hyper-vascular properties of periosteum provided the MRONJ-affected bone with the necessary vascular support for osteogenesis and disease reversal.20 Finally, our technique is bone-sparing, which leaves further options for later reconstruction as required and negates the risk of internal fixation: introduction of foreign material, possible damage to osteoblasts and non-union associated with free fibular transfer.
The inclusion of local nasolabial, mylohyoid muscle or buccal fat flaps as well-vascularised tissue above decorticated bone has been shown to improve healing rates for MRONJ.7,21,22 In this series, patients were selected for nasolabial flap reconstruction if the area of necrotic bone was smaller and located in the maxilla predominantly or if the patient’s comorbidities favoured a shorter and less risky procedure. One of the three patients in this series treated with nasolabial flap had their underlying pathology in the anterior mandible. This patient’s high level of comorbidity precluded them from consideration for microvascular free flap reconstruction. The reliability of nasolabial flap use for maxillary-based defects shown in this series is similar to previous studies.7
Previous studies have advocated against extensive bone resection and complex reconstructive procedures, arguing the average life expectancy of the advanced MRONJ population and the high complication rate of these procedures makes this an unrealistic option. This argument is countered by the zero per cent complication rate for flap patients in this series.
Limitations
The major limitation of this study is its small patient sample size and subsequent comparative case series study design. Medication-related osteonecrosis of the jaw is a rare and relatively new disease which pose a challenge to patient recruitment. Moreover, vascularised periosteal RFFF reconstruction for MRONJ is a novel treatment and hence the findings presented in this study are preliminary.
Conclusion
We report preliminary evidence that local nasolabial flap and vascularised periosteal radial forearm flap reconstruction for advanced MRONJ is more effective at halting the disease and alleviating morbidity than conservative dental measures alone. We report the first cases of a vascularised periosteal RFFF in MRONJ as well as novel radiological evidence that this technique may reverse disease progression through the formation of new bone and prevention of pathological fracture. Within the limitations of a comparative case series, we believe local flap coverage and RFFF with vascularised periosteum show promise in the treatment of osteolysis in MRONJ and other diseases affecting the maxillofacial skeleton.
Prior publication
This study follows on from an abstract published from the 2020 Royal Australasian College of Surgeons Annual Scientific Congress, which did not proceed due to the COVID-19 pandemic.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Disclosure
The authors have no financial or commercial conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.
Revised: March 8, 2021 AEST