Introduction
In Australia, breast augmentation surgery is the most popular cosmetic procedure.1 The International Society of Aesthetic Plastic Surgery reported 17,553 breast augmentations in Australia in 2018 which accounts for 17 per cent of total aesthetic surgical procedures.1 With its increasing popularity, it is not surprising Australians are exploring options when it comes to selecting plastic surgery services and, in some instances, are choosing to have their cosmetic breast surgery abroad.
Aesthetic surgery tourism is a financial-driven phenomenon with overseas surgeons offering considerably cheaper services.2,3 This is also fueled by access to information online and the relative affordability of travel.4 On average, a breast augmentation in Australia can cost between AU$10,000 to AU$15,000.5 Factors that go into these costs include surgeon’s fee, anaesthesiologist, choice of implant, recovery time and follow-up appointments. Some overseas websites advertise breast augmentation surgery at costs as low as AU$1800.6
Although information regarding the risks of cosmetic tourism is readily available, an increasing number of Australians continue to choose to travel overseas for aesthetic surgery causing a surge in demand for the management of complications.1 Problems mostly occur after the patients return to their home country as they have not received sufficient follow-up care.7 Regularly reported complications include infection, wound dehiscence, pain/discomfort and aesthetic dissatisfaction.7,8
In 2008, the Journal of Plastic Reconstructive and Aesthetic Surgery published a report from the British National Health Service that highlighted the impact of cosmetic tourism on UK plastic surgeons, addressing the funding necessary to treat complications and the need for evidence based guidelines on their management.3 In Australia, there continues to be a paucity of accurate data to reflect the number of complications from these overseas surgeries which commonly end up being treated in our healthcare system.
The Australian Breast Device Registry (ABDR) is available to all patients in Australia undergoing breast device surgery, including those who had implants inserted aboard. The ABDR has a data collection form for recording a standardised minimum dataset at the time of surgery in Australia.9 The aim of this study is to establish the financial costs from complications of overseas inserted implants being treated at our unit as recorded by the Australian Breast Device Registry (ABDR).
Methods
Ethics and data access were approved by the ABDR. Research approval was obtained from the Royal Brisbane and Women’s Hospital ethics committee [HREC/2019/QRBW/59101]. A retrospective analysis of data recorded from the ABDR was performed. All patients identified on the registry as having overseas inserted breast implants surgically removed at RBWH from October 2014 to October 2019 were included in the study. Aggregate data was provided by secure file transfer. Information was collected regarding the reason for surgery, the procedure description, type of surgical complication and further in-hospital treatment.
The financial cost of hospital admission and outpatient follow-up of patients with complications from overseas breast implants has been calculated by the RBWH data analysis and assurance team using electronic medical records and discharge codes.
Results
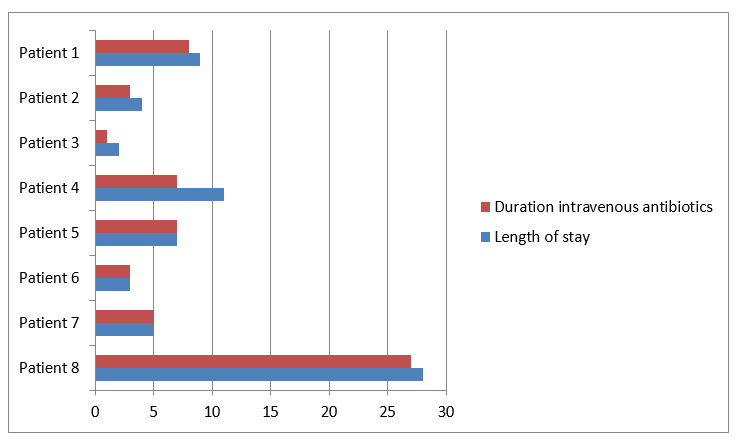
Of the 331 surgical cases of explantations recorded, 149 (45.0%) involved removal of tissue expanders and 182 (55.0%) involved the removal of breast implants (without description as to whether this was due to cosmetic breast augmentation or reconstructive surgery). Eight cases in total (2.4%) were from breast devices inserted overseas. Of these, nearly all were bilateral implant augmentations for cosmetic enhancement (n = 7) though one case was an immediate reconstruction post bilateral mastectomy for cancer treatment with tissue expanders. Most patients had their initial surgery performed in Thailand (n = 6) with only two other cases reported as having their initial surgery in the Philippines and South Africa. All eight patients were below the age of 40 with no significant comorbidities. The majority of patients presented via our emergency department (n = 7), two of whom were in an unstable condition. The clinical presentation varied from localised wound infection/breakdown and skin cellulitis (n = 6), to systemic compromise with sepsis (n = 2). Seven (n = 7) patients required emergency operations which involved removal of the bilateral breast devices, wound washout and closure over surgical drains with two cases requiring skin debridement and negative pressure wound therapy. Two patients required more than one operation which involved further washout and debridement of skin and tissue. One patient required medical intensive care postoperatively for a period of 24 hours for respiratory support in the context of sepsis. All patients required intravenous antibiotic therapy while in hospital and dressing changes. Multi-resistant organisms were cultured in two of the eight cases and were associated with longer inpatient treatment (Table 1). Length of stay ranged from two to 28 days with a median length of stay of 8.6 days (Figure 1). This was primarily guided by the duration of intravenous antibiotic treatment which varied from 24 hours to three weeks. None of the patients were referred to the RBWH’s Hospital in The Home (HITH) program for outpatient administration of intravenous antibiotics. Most patients had multidisciplinary team involvement with infectious disease being the most consulted specialty (n = 5). Other specialties included perioperative medicine, intensive care and the acute pain team. All patients were offered more than one follow-up appointment in the plastic and reconstructive surgery outpatient clinic. An estimate of the total cost of explantation procedures for this period is AU$2,745,500. The complications from overseas inserted breast devices cost our hospital AU$110,963.96. The most cost associated with a single patient was AU$32,794.31 with an average of AU$13,870.5 per patient (Table 2).

Discussion
Our results show the costs of surgical removal of overseas inserted implants represent approximately four per cent of the RBWH’s budget for breast explantations for this period. Although this figure may seem trivial, we anticipate this percentage will increase in the following years.
While the absolute numbers of people travelling abroad for cosmetic surgery are lacking, we can comment on an increasing number of patients with complications presenting to our department within the past three years (7 out of 8 cases within 2017– 2019 period). This is also supported by a recent survey by the Australian Society of Plastic Surgeons (ASPS) which reports a staggering 38 per cent rise in the number of Australian patients requiring corrective treatment due to complications from overseas plastic surgery.10
In 2008, Jeevan and colleagues3 highlighted the impact that cosmetic tourism has had on the British National Health Service addressing the need for funding to treat complications and national guidelines for their management. More recently, in Australia, Livingston and colleagues11 revealed the burden from overseas cosmetic procedures at the Gold Coast University Hospital to be over AU$150,000 in a one-year period with complications from breast augmentation surgery being the most common. Their findings support the need for increased public health strategies with the aim of prevention of morbidity and mortality of patients engaging in cosmetic tourism.
In our study, we found wound infection as a predominant complication after implant-based breast surgery abroad, followed by wound breakdown and pain/discomfort. This is in keeping with the results of previous studies conducted in Great Britain and United States.7,12 Additionally, a recent study from the United States presented a series of mycobacterial infections after cosmetic surgery in developing countries.13 The authors concluded that due to the low incidence of mycobacterial infections in first world countries there is often a delay in the diagnosis and management of these infections. In our study, one of our eight cases had a mycobacteria infection. This patient had the longest inpatient stay with a delay in the microorganism diagnosis and antibiotic sensitivities likely contributors.
Interestingly, none of the patients were referred to the HITH program for the delivery of antibiotics in the community. This was possibly due to the complexity of their surgical wound care which required daily review by a member of the plastic surgery team in order to assess antibiotic response and guide ongoing treatment. Future management of these patients could aim at reducing the duration of their inpatient care by optimising their wound care management in order to facilitate outpatient treatment.
Limitations
Although this is the first study to analyse overseas breast implant surgery complications using ABDR data, our study is limited by several factors. The ABDR data collection form failed to accurately capture data in 20 per cent of the cases as some datasets were incomplete at the time of surgery. For this reason, we are unable to comment on the type of implant removed and the presence of implant complications such as rupture. There is the potential human error factor where it is possible that some surgical cases of removal of overseas placed implants were not collected in the ABDR data form, or were not correctly transcribed into the ABDR database. The database only incorporates patients who had surgical removal of breast implants, therefore does not include non-surgical admissions from overseas placed implants. Consequently, the relative number and cost of complications from overseas placed implants may be underestimated. Likewise, numbers from neighbouring hospitals treating complications secondary to cosmetic tourism have not been included in our study.
Future research could aim at comparing our findings to the complication rates of domestically inserted cosmetic implants.
Conclusion
Through the ABDR we were able to capture the cases of patients who underwent implant removal surgery from overseas inserted devices at the RBWH to date. The RBWH’s data was used to analyse the cost to the hospital from complications of overseas breast implant procedures. The financial costs of cosmetic tourism to the RBWH over a five-year period is estimated at AU$110,963.96, which represents four per cent of the total hospital spending on breast device explantations. Surgical complications from overseas inserted implants cost a small percentage of the RBWH’s budget for breast procedures, however, with the increasing popularity of cosmetic tourism, this figure could increase in the following years.
These findings, we believe, could be used to create informed public health campaigns about medical tourism and provide evidence-based facts on the risks and implications of pursuing breast enhancing procedures outside Australia. We aim to use this information to provide feedback to the RBWH regarding the actual cost of these patients so that decisions can be made as to whether these patients should be required to reimburse part of the cost of their treatment given their decision to have the surgery overseas resulted in a burden to local services. These findings could also be used in public health campaigns to educate individuals to make better choices and reduce the financial burden to public hospitals in Queensland.
Acknowledgements
We gratefully acknowledge the contributions from the Australia Breast Device Registry in the development of this study.
Disclosure
The authors have no financial or commercial conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.
Revised: 2021 January 15 AEST