

Introduction
The incidence of complex scalp reconstruction has decreased due to a combination of factors. Improved patient education and increased surveillance have led to earlier detection of disease. To a lesser extent, the increased use of dermal substitutes has also contributed to a reduction in microsurgical scalp reconstruction. In addition, medical therapy in the form of immunotherapy has emerged as an alternative that provides relatively effective and durable disease control where surgery is contraindicated.
A challenging cohort of patients remains, who require complex scalp reconstruction. They include patients with advanced malignancies involving the skull or refractory to other treatment modalities, osteoradionecrosis and failed cranioplasty. In these patients, microsurgical free flap reconstruction is commonly the only reconstructive option.
In this article, we describe a streamlined approach to microsurgical scalp reconstruction including cranioplasty, which has evolved out of experience and our clinical outcomes.
Methods
This is a retrospective study assessing the clinical outcomes over a five-year period of complex scalp reconstruction carried out by the senior author (SC).
Patients who had undergone ‘free flap reconstruction’ and ‘scalp reconstruction’ were identified from a prospectively maintained database. Data on patient demographics, disease aetiology, surgery and postoperative follow-up were gathered.
Surgical technique
Microsurgical free flap reconstruction
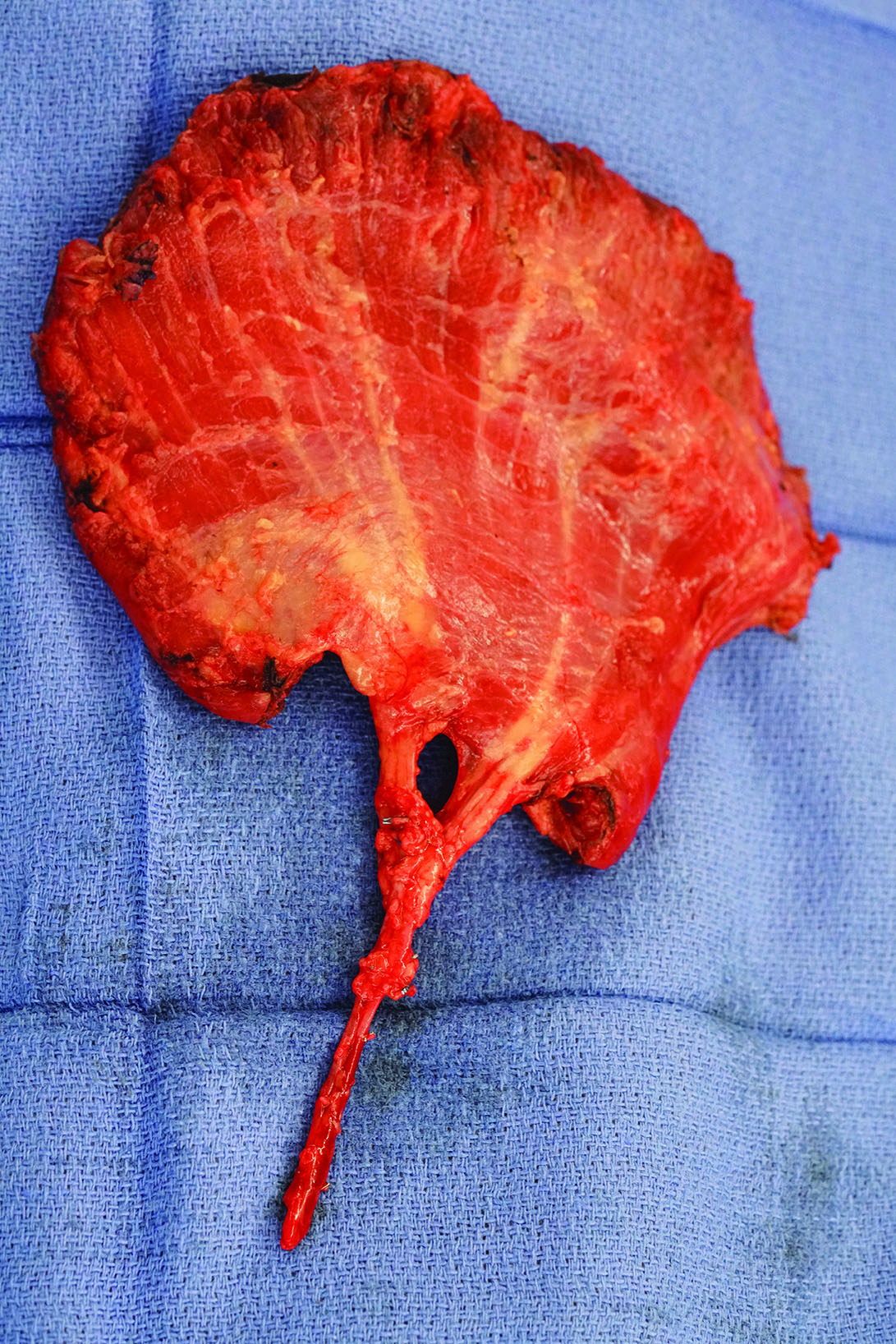
The latissimus dorsi (LD) free flap is our workhorse for scalp reconstruction. The patient is placed in a lateral decubitus position throughout the case. Therefore, the ipsilateral LD free flap is prerequisite if intraoperative re-positioning of the patient is to be avoided. Simultaneous preparation of the superficial temporal (ST) vessels as recipient vessels and LD free flap harvest are carried out by two separate teams. For defects over the scalp vertex, the recipient vessels are prepared 1–3 cm superior to the helical rim to decrease the length of free flap vascular pedicle necessary (Figure 1). Where the ST vein is not an appropriate recipient, a cephalic vein turn-up is preferred over a segmental inter-positional vein graft. The LD free flap is routinely harvested distal to the pedicle bifurcation, which requires intramuscular dissection of the vascular pedicle (Figure 2). This increases free flap pedicle length without the need to undertake tedious dissection in the axilla, as well as ensuring a better calibre match with the distal ST vessels. We have been able to regularly increase our pedicle length by 4 cm with this technique. This technique also allows us to exclude the bulkiest proximal triangular part of LD from the free flap for improved contouring. In patients where an LD free flap is used for coverage of the cranioplasty implant, a temporising skin paddle is required. In this situation, a thoracodorsal artery perforator (TDAP)–LD chimeric free flap is favoured. A segmental LD free flap is harvested if only a small flap is required.
_t.jpg)
_muscle_free_flap_is_dissected_intramuscular.jpg)
Cranioplasty
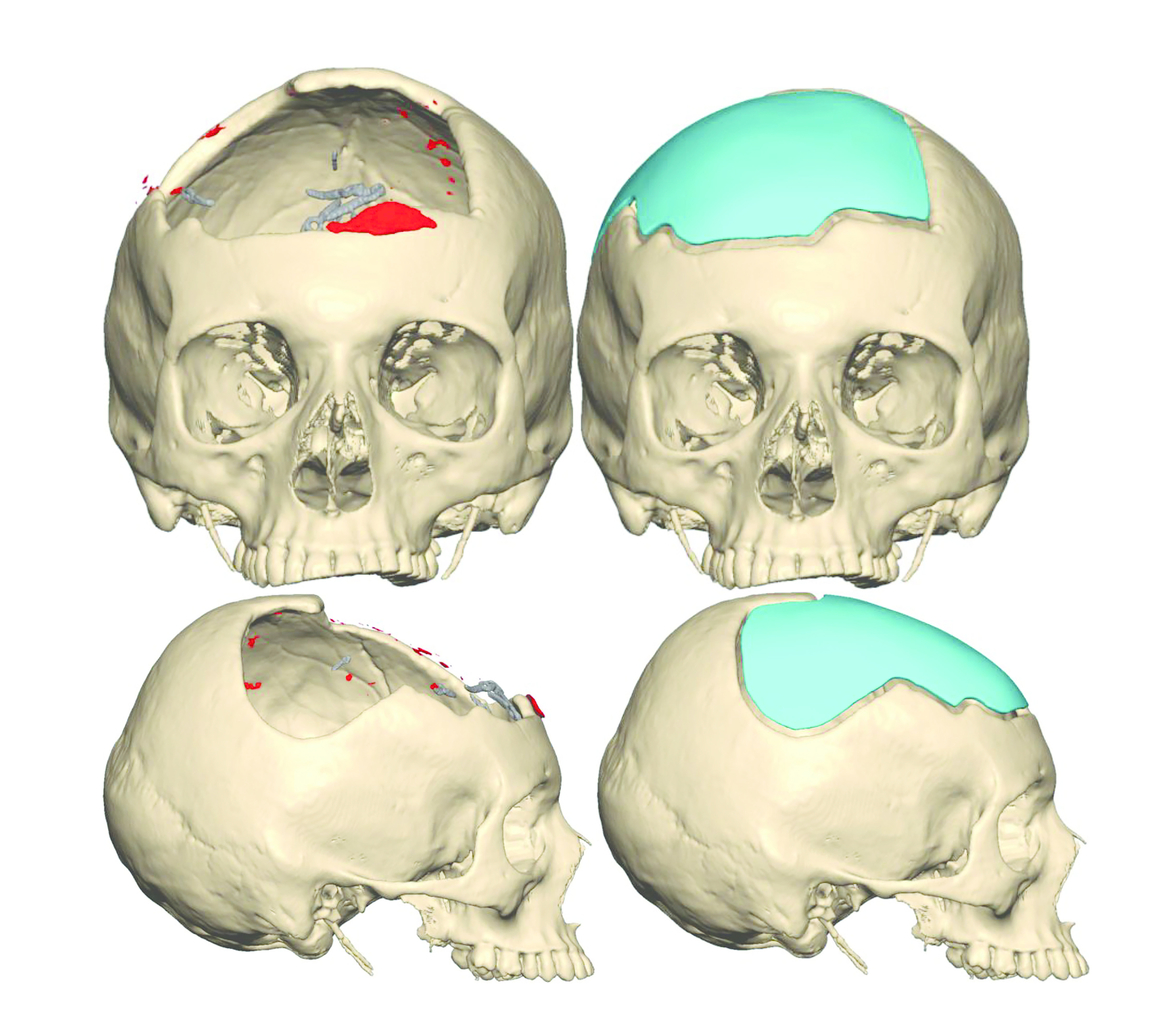
Preoperative virtual surgical planning (VSP) is carried out to customise the cranioplasty implant if the cranial defect is complex. The implant is fashioned so that it is offset by 3 mm (Figure 3). This allows the native scalp skin to be reapproximated without tension at a later stage following eventual atrophy of the underlying LD muscle, and the temporising intervening free flap skin paddle excised (Figure 4a and Figure 4b). Polyetheretherketone (PEEK) was the cranioplasty implant material of choice where VSP was carried out, and polymethylmethacrylate (PMMA) where cranioplasty was fashioned de novo intraoperatively.


Surgical sequencing
To reduce the duration of cranioplasty implant exposure, the microsurgical free flap reconstruction precedes the neurosurgical component of craniectomy/cranioplasty. The former is completed, and the vascularised free flap moved to the periphery of the surgical field and protected, during the latter. Following insertion of the cranioplasty implant, the free flap is inset immediately in a ‘vest-over-pants’ manner.1
Results
In total 39 operations were performed in 35 patients. The commonest disease aetiology was advanced cutaneous malignancy—squamous cell carcinoma (n = 22), melanoma (n = 2), basal cell carcinoma and angiosarcoma (n = 1); osteoradionecrosis (n = 8); failed bone flap requiring explantation following a neurosurgical procedure (n = 3); wound breakdown following cerebral bypass (n = 1); and meningioma (n = 1). Nine patients underwent postoperative adjuvant radiotherapy.
A full LD (including muscle-only and musculocutaneous) free flap was harvested in 24 cases, a segmental LD free flap in three, a chimeric TDAP/LD free flap in three, and a chimeric LD/ serratus anterior free flap in one. The other miscellaneous free flaps included radial forearm free flap (n = 5), ulnar artery perforator free flap (n = 2) and anterolateral thigh free flap (n = 1). Full-thickness craniectomy was performed in 14 cases, and cranioplasty was performed in 12 cases (8 PMMA, 3 PEEK and 1 titanium). Two skull defects were not reconstructed due to poor prognosis. Nine patients underwent resection of the dura, including the sagittal sinus in two.
The superficial temporal artery (STA) was the recipient artery of choice in 32 (82%) cases, and the superficial temporal vein (STV) in 29 (74%) cases. The STV was not available as the recipient vessel in three (9%) cases. Other recipient vessels included the facial artery (n = 5), external carotid artery (n = 1), transverse cervical artery (n = 1), (tributaries of) the internal jugular vein (n = 6), external jugular vein (n = 1), postauricular vein and transverse cervical vein (n = 1). Cephalic turn-up was used in two cases, including one free flap venous congestion salvage where an interpositional vein graft had been used. There was a close calibre match between the STA and STV, with a mean vessel calibre of 2.4 mm.
The median follow-up period was 12.9 months (range 0.5–49.2 months). At the time of analysis, there had been cumulatively eight cases of local disease recurrence and three disease-specific deaths. Complications included free flap venous congestion successfully salvaged (n = 1), infected PMMA cranioplasty requiring explantation subdural haematoma requiring craniotomy for evacuation (n = 1) and free flap donor site haematoma (n = 2).
Discussion
In this series of 39 complex scalp reconstructions we describe a range of technical refinements in free flap harvest, vessel selection and cranioplasty technique that are both well established and novel.1,2
Our experience showed the ST vessels to be reliable and safe recipients in the large majority of cases, in line with Hansen and colleagues, Halvorson and colleagues and Chen and colleagues.3–5 However, some key technical aspects of our surgical approach differ significantly from theirs. Chen and colleagues described dissecting the ST vessels proximally into the parotid parenchyma inferior to the tragus to obtain a vessel diameter of at least 2.0–2.5 mm.5 Hansen and colleagues and Halvorson and colleagues also reported routinely using the main trunk of the ST artery and vein, to avoid vessel spasm.3,4 We propose the contrary: dissecting the ST vessels distal to their bifurcation onto the parietal scalp for defects over the scalp vertex to decrease the required free flap vascular pedicle length. We have found the vessel calibre to be between 2 mm and 2.5 mm at this level. In the few cases where the ST vessels had been prepared within the parotid gland in this series, the vessel calibre we encountered was greater, that is 3–3.5 mm, which is similar to that reported by Halvorson and colleagues.4 We have not found the distal ST vessels to be prohibitively spasmodic with routine use of papaverine irrigation. Chen and colleagues advocated hand-sewing the STV due to the extreme thinness of its wall.5 While we concur that the STV is indeed thin-walled, we have been able to perform all cases of venous anastomosis to the STV with a Synovis Microvascular Anastomotic Coupler System (Synovis Micro Companies Alliance Inc, 439 Industrial Lane, Birmingham, United Kingdom AL35211).
The cephalic vein turn-up has proven to be an invaluable alternative for microsurgical head and neck reconstruction.6,7 Although it did not feature extensively in our current series, from our overall experience in head and neck microsurgical reconstruction, the cephalic vein turn-up is a reliable option. When harvested from the level of the elbow it can easily reach the preauricular level. It has the other advantages of being a high-flow, low-pressure system, carrying only one venous anastomosis as opposed to two for a vein graft; easily concealed; and usually outside previous radiotherapy fields. It might be the only option in a vessel-depleted woody neck, and is arguably easier to dissect than the other potential candidate, the internal mammary vein.8–10
The ideal timing of cranioplasty in skull reconstruction is controversial.11–16 A literature review by De Cola and colleagues concluded that a latent period of three to six months following decompressive cranioplasty may significantly improve motor and cognitive recovery.17 Morton and colleagues advocated for timing the cranioplasty for skull reconstruction between 15–30 days, taking into consideration the risks of infection, bone flap resorption and development of seizure in non-oncological patients.18 Whether their findings could be extended to oncological patients is at present unclear. It is certainly impractical to routinely stage reconstruction in patients in whom postoperative adjuvant radiotherapy and/or chemotherapy are commonly indicated. While there are no published data, we propose that the most important parameter in decreasing cranioplasty infection is the duration the synthetic implant is exposed intraoperatively, hence our recommendation that microsurgical free flap reconstruction be completed prior to the neurosurgical component. In our patients, synthetic cranioplasty is usually exposed for less than five to 10 minutes.
Preoperative virtual surgical planning for skull reconstruction has not received the same attention as that for the facial skeleton due to (perceived) lesser complexity, but there are some nuances worth noting for a finessed customised reconstruction.19,20 We offset the PEEK cranioplasty by 3 mm, and have found that degree of offset allows for the native scalp skin to be approximated over the atrophied LD muscle free flap without undue tension and yet maintains the natural convex appearance of the scalp.
Limitations
We acknowledge some of the limitations of this study. The data is as accurate as possible for a retrospective study as it was extracted from a prospectively maintained database. We had originally intended to assess the duration of surgery but omitted that aspect as we contemplated how the permutations of resection and reconstruction differed for each case.
Conclusion
Complex scalp reconstruction incorporating cranioplasty can be reliably and safely streamlined with preoperative VSP, intramuscular dissection of the LD free flap vascular pedicle, distal anastomoses to the ST vessels, and reversed sequencing of microsurgical reconstruction and craniectomy/ cranioplasty.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Disclosure
The authors have no financial or commercial conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.