
Introduction
Intra-tendinous infiltration with tophaceous gout leading to spontaneous rupture in the hand is rare,1,2 with the flexor sheath thought to provide some protection from infiltrative disease.1,3 This differs from other areas of the body where rupture is comparatively common. Prior trauma may predispose specific digits to inflammatory deposition of urate crystals in a hyperuricaemic patient.1 Gouty involvement of the hand may present as arthritis, carpal tunnel syndrome, tophaceous masses, synovitis and suppurative tenosynovitis but very rarely as closed ruptures.4,5 We report on only the second case described within the literature of spontaneous rupture of flexor tendons within the hand, and detail an approach to the assessment, investigation and management of these cases with a comprehensive literature review.
Case
A 51-year-old right-hand-dominant man with an elevated body mass index (BMI) presented two days after experiencing a sudden ‘pop’ [sic] in his left middle finger while opening a drawer. The patient noticed immediate swelling of the finger and loss of flexion. His only medical history of note was hypertension with no prior trauma in the region, rheumatoid or osteoarthritis. Physical examination demonstrated loss of distal interphalangeal joint (DIPJ) flexion and limited proximal interphalangeal joint (PIPJ) flexion. The digit was neurovascularly intact with normal extension and intrinsic function. X-ray examination was unremarkable with no foreign bodies or degenerative change. Ultrasonography reported a closed rupture of the flexor digitorum profundus (FDP) tendon in the region of the A3 pulley with an estimated gap of 22 mm.
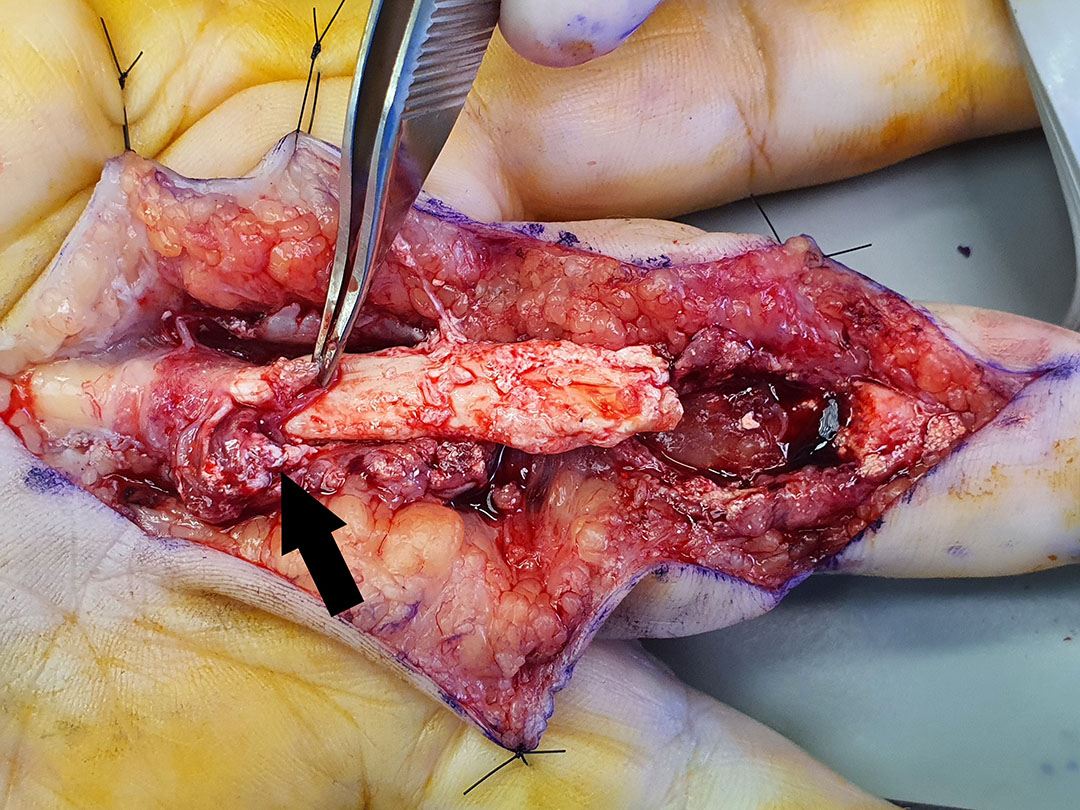
Surgical exploration showed extensive tophaceous and liquefactive gouty deposits within the soft tissue surrounding calcified and avascular FDP and FDS tendons from the A1 through to the A4 pulley, inclusive (Figure 1). Delineation demonstrated complete rupture of the FDP tendon with calcification of the FDS at the chiasm, total rupture of the radial slip, and subtotal rupture of the ulnar slip (Figure 2). The avascular and necrotic tendon was excised and sent with the liquefactive material for histopathology, microscopy and culture. Following debridement, washout, and carpal tunnel release, a 4 mm silicone rod was placed in situ through to the proximal wrist for staged reconstruction of the FDP. The patient was started on colchicine 500 mg twice daily in consultation with rheumatology colleagues.


Histopathology demonstrated deposits of basophilic acellular material surrounded by a giant cell and histiocytic response. Large deposits of urate crystals were noted on confocal microscopy and tissue culture was aseptic. The patient subsequently volunteered that he had experienced mild and infrequent attacks of gout in the past but never in the hand region.
Following three months of medical therapy coupled with hand physiotherapy, the patient underwent palmaris longus tendon grafting in an optimised and supple digit. At the first review post-reconstruction, the DIPJ was noted to be in 10 degrees of fixed flexion, while the PIPJ and metacarpophalangeal joints (MCPJ) were stable with a full range of movement. Some scar hypersensitivity was noted, and intensive desensitisation training was included with hand therapy in subsequent weeks. The patient returned at six weeks post reconstruction with a full range of movement—including in the DIPJ—and resolution of the scar hypersensitivity. Formal total active movement (TAM) measurements were not undertaken as routine. The patient has since resumed all normal duties at work, including pulling himself up into the cab of heavy industrial vehicles.
Discussion
Closed flexor tendon ruptures most commonly occur due to traumatic avulsion, followed by attrition.6 Potential causes of attrition include rheumatoid and osteoarthritis, carpal bone pathology, anatomical fulcrums, and prior plate fixation.6 Insidious and chronic synovial infection of the hand, most commonly by mycobacteria, can also result in closed tendon rupture.7 Other unusual aetiologies include infiltrative and proliferative synovial conditions such as systemic lupus erythematosus, sarcoidosis, amyloidosis, and crystal deposition as seen in our patient. Prior steroid injection or fluoroquinolone antibiotic use are potential contributory factors but iatrogenic cases are uncommon.6
A search of the literature using the PubMed® database for ‘gout’ and ‘tendon rupture’ revealed only one similar case of flexor tendon rupture in the hand.3 Of the remaining five reported cases of tendon ruptures secondary to gouty infiltration in the upper limb, one occurred in a distal biceps tendon,8 and the rest in extensor tendons.5,9–11 This distribution pattern may support predisposition by prior trauma and inflammation.1
To determine the epidemiology of pathological alterations in human tendons, Józsa and colleagues retrospectively analysed the histopathology of 1966 tendons collected over the course of 18 years.2 Of these, 1024 were biopsy or ‘pathological’ samples, and 942 were autopsy or ‘control’ specimens. Out of an eventual 1258 pathological tendons (944 biopsy and 314 autopsy samples), gout was found in only six specimens (0.3%). Of the 494 spontaneous ruptures accounting for biopsy specimens, none were due to gout. In decreasing order of frequency, hypoxic-degenerative tendinopathy, tendolipomatosis, mucoid degeneration and calcific tendinitis accounted for the ruptures.2 A subsequent prospective case-controlled study of spontaneously-ruptured tendons by the same group yielded similar results, with only one of 891 ruptured tendons affected by gout.12
The investigation and treatment of closed tendon ruptures needs to consider potential aetiology, particularly in an undifferentiated presentation. Where a diagnosis is unestablished, intraoperative specimens should be sent separately in saline, formalin, and as a fresh specimen; this will facilitate polarised light microscopy, diagnostic staining and microbiological culture respectively. Atypical mycobacterial and fungal cultures should also be requested.6
Conclusion
Gout in the hand is a rare but important cause of spontaneous tendon rupture. The surgical management of gout within the hand was summarised by Moore and Weiland as the excision of tophaceous deposits to (1) alleviate pain, (2) control infection and drainage, (3) decompress nerve(s), (4) reduce total body urates, and (5) to improve the ability of the patient to wear rings and gloves.5 We suggest that the excision of tophaceous deposits to ‘facilitate functional improvement or reconstruction’ constitutes an important sixth indication, as demonstrated in the literature as well as our own case.
In our patient, carpal tunnel decompression relieved localised swelling and facilitated the insertion of the silicone rod. Debridement of the necrotic, infiltrated tendon and synovium coupled with prompt, ongoing medical therapy decreased the locoregional urate burden and associated inflammation. Together with medical and hand therapy, this facilitated the successful staged reconstruction of function in a supple digit free of associated pathology with no residual flexor deficit.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Disclosure
The authors have no financial or commercial conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.
Revised: 2021 July 28 AEST