
Introduction
NovoSorb® (PolyNovo Biomaterials Pty Ltd, 2/320 Lorimer Street, Port Melbourne, Victoria, 3207, Australia) biodegradable temporising matrix (BTM) is a synthetic dermal substitute that has provided an alternate approach to dermal loss and reconstruction to the classical reconstructive ladder. Biodegradable temporising matrix is designed to be used in a two-stage process in conjunction with skin grafting and provides an intermediate step where the wound bed is improved prior to definitive grafting.1 To date, there are few cases that have documented secondary intention healing over BTM and these have involved small areas in physiologically well individuals. This case represents the largest area of healing via secondary intention over BTM we are aware of in the literature, which resulted from continued deferment of the secondary grafting procedures due to the patient’s fluctuating acute medical status.
Case
A 66-year-old woman was referred to the Launceston General Hospital (Tasmania, Australia) plastic surgery unit in March 2020 with extensive skin necrosis of her bilateral upper limbs and left lower leg secondary to an undifferentiated vasculitic process, estimated at 8 per cent of her total body surface area (TBSA). Her medical history of note included Sjogren’s syndrome and supraventricular tachycardia managed with apixaban. The patient was under the joint care of the rheumatology and dermatology teams and was commenced on high dose corticosteroids and methotrexate.
After a period of medical stability, the patient underwent serial debridement of the remaining eschar down to fat totalling approximately 4.5 per cent TBSA. Given the depth and size of the defects and still unclear aetiology, BTM was applied to temporise the wound and was dressed with Acticoat® and Hypafix® (Smith and Nephew, 85 Waterloo Road, North Ryde, NSW, 2113, Australia). Split skin grafting was scheduled five weeks post-BTM application, but a further flare up of cutaneous necrosis and anaemia of unknown origin necessitated deferment. In the subsequent months, the patient had several hospital admissions with recurrent medical decompensations and community-acquired pneumonias thought to be related to her immunosuppression and still unclear diagnosis. As the BTM showed signs of stable integration and resistance to infection, skin grafting continued to be postponed.

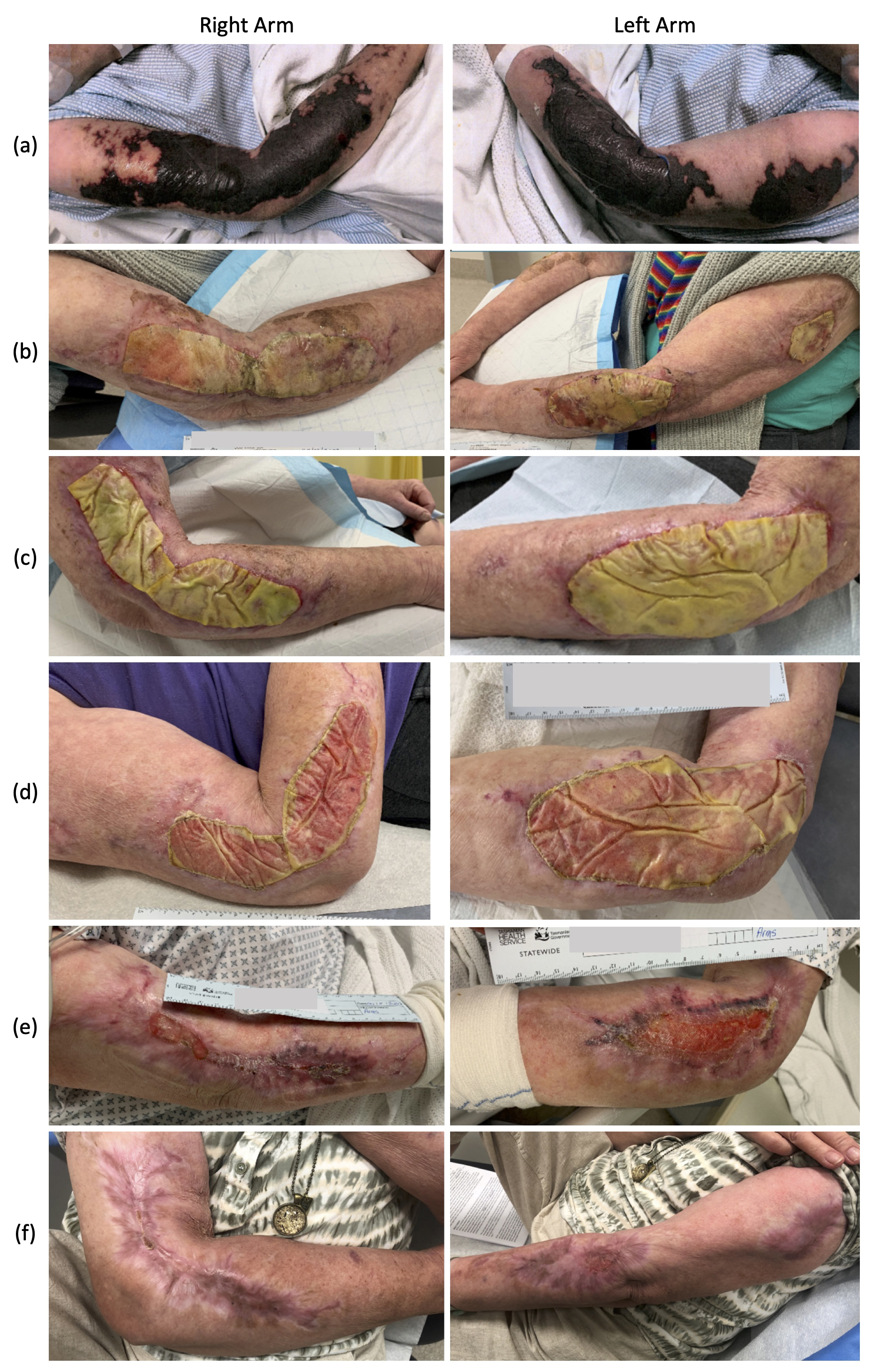
During this time the patient had frequent wound reviews in the plastics clinic and was managed with chlorhexidine wash and Mepilex® lite foam dressing (Mölnlycke Health Care Pty Ltd, Level 4, 12 Narabang Way, Belrose, NSW, 2085, Australia). Due to high exudate secondary to infection, this was initially a daily dressing plan performed by community nursing but was reduced to twice weekly after BTM integration. At three months post-BTM application, the bilateral upper limb wounds showed significant secondary healing and wound contraction with partial auto-delamination of the BTM sealing membrane. The remaining membrane was delaminated in clinic and wounds were dressed with foam dressing until completion. At six months post-BTM application, bilateral upper limbs were completely healed by secondary healing (Figure 1). The lower leg wound required surgical debridement of infected BTM and was managed with negative pressure wound therapy (NPWT) followed by simple dressings and resulted in a chronic wound. Of interest, the patient has retrospectively been diagnosed with calciphylaxis, a rare and poorly understood disorder resulting in vascular calcification and microthrombi leading to skin and soft tissue necrosis.
Discussion
Biodegradable temporising matrix is a synthetic dermal substitute that has been described for use in the treatment of full thickness skin defects encountered in burns, necrotising skin and soft tissue infections and trauma.1–5 It is designed to be used in a two-stage reconstructive process. The first stage involves application of the BTM to a debrided full thickness dermal wound. Fibroblasts and neovasculature then migrate into the synthetic matrix creating a neodermis suitable for grafting. After integration of the BTM, the second stage of reconstruction involves delaminating the sealing membrane and application of a split skin graft onto the underlying neodermis.5–7 Case series on burns patients and those with complex trauma have reported excellent outcomes with reliable integration, resistance to infection and good scar outcomes.1,4,8
This case represents a deviation from the recommended management of BTM. The first stage of reconstruction was successful; however, the second stage of grafting was unable to be completed due to the patient’s unstable medical status. A literature review revealed just three other cases of secondary healing over BTM and these were in small isolated areas.9,10
Our patient healed via epithelisation over the BTM with associated contracture of the wounds without deformity or banding. Initially the scars matured with a mixed scar pattern exhibiting both areas of hypo- and hyperpigmentation; however, throughout healing the scars remained supple and maintained good contour with the surrounding tissue. At 26 weeks post-BTM application, the upper limb wounds had largely healed. Elbow range of motion was preserved and the patient reported no itch or neuropathic pain associated with the scars. Improved scar cosmesis and itch scores have been previously noted in case reports on burns patients following BTM application and grafting compared to grafting alone.6 Overall the patient was satisfied with the cosmetic and functional scar outcomes, and at the 12-month follow-up scars were soft and pliable and variations in pigmentation had reduced (Figure 2).

Biodegradable temporising matrix’s resistance to infection is well documented.1 As demonstrated by Wagstaff and colleagues in the first human case series on BTM, and Solanki and colleagues in a recent series of 25 complex wounds,4 20–40 per cent of BTM cases exhibited clinical signs of infection, but just one case resulted in failure of BTM integration.5,8 Our case presents similar results. Three weeks post application, the BTM exhibited signs of clinical infection including a yellow-grey colour, significant exudate and wound swabs positive for Staphylococcus aureus and Enterococcus. The patient was managed with appropriate oral antibiotics and daily dressings in the community where the exudate under the sealing membrane was expressed and the wound cleansed with a chlorhexadine soak prior to application of a Mepilex® foam dressing. Our unit has had success with this management plan for simple seromas under the BTM and so chose to trial this management on infected BTM. While the lower limb BTM was unable to be salvaged, the upper limb BTM continued to integrate despite the patient’s physiological and pharmacological immunosuppression demonstrating notable resistance to infection.
On reflection, the decision to use BTM was likely the right choice for this patient despite being unable to complete the second stage of reconstruction. At the time of debridement and reconstruction, the patient had been medically stable and was thought to be progressing well in remission from the primary insult and so functional and cosmetic factors were considered when deciding on reconstructive options. Biodegradable temporising matrix was chosen due to the size, depth and varied location of the defects. Negative pressure wound therapy was not used initially due to the number of limbs involved, which would have significantly affected the patient’s mobility and ongoing reconditioning, however it was used on the lower leg after BTM failure. Primary skin grafting into the defects was considered, however was opted against due to concerns over donor site morbidity and the impressive cosmetic outcomes following BTM reconstruction being seen in the unit. Given the retrospective diagnosis of calciphylaxis, it is still unclear if the decision to avoid immediate skin grafting was correct. There is no consensus in the appropriate management of calciphylaxis wounds with some groups advocating against grafting due to the risk of donor site morbidity. The literature contains several case reports and series documenting the challenging nature of these wounds, which often require multiple trips to theatre, debridements and have variable graft success with one retrospective study of seven patients reporting individual graft takes of 30–90 per cent.11,12 Furthermore, in our patient’s case, reconstructive flap options were limited due to the size and location of the defects and concerns regarding reliability of vascular pedicles given the unclear diagnosis.
Conclusion
This case reports the largest area of secondary healing over BTM we are aware of in the literature. Given the patient’s overall instability and retrospective diagnosis of calciphylaxis, the outcome of soft pliable scars without skin grafting within six months is a positive outcome. Biodegradable temporising matrix provided adequate temporising coverage largely resistant to infection despite the patient’s immunosuppression and facilitated ongoing healing despite poor physiological reserve.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.
Revised: August 16, 2021, September 14, 2021 AEST