


Introduction
Successful reconstruction of total laryngopharyngectomy (TLP) can be challenging. As the new digestive tract serves to transmit food boluses and enzyme-rich liquids, it must be impervious in its entirety.
Head and neck reconstruction methods have progressed significantly in recent decades. Originally these defects were treated with local flaps,1 pedicled flaps (for example, pectoralis major)2 followed by visceral conduits (eg gastro-omental) and free flaps (for example, jejunal), and most recently fasciocutaneous free flaps.3 At our institution the anterolateral thigh (ALT) free flap is the preferred donor site and has many advantages for head and neck reconstruction.4,5 Importantly, the ALT provides a large skin paddle with a long vascular pedicle and the ability to be raised as a chimeric flap. It is distant from the area of resection so lends itself to a concurrent raise during oncological resection in a two-team approach. Compared with the radial forearm free flap (RFFF), the ALT donor site has superior cosmesis and lower morbidity.5 In comparison with the visceral free flaps, it does not violate the abdominal cavity and risk the morbidities associated with viscus resection.3
Modifications to the harvest and inset of the ALT have sought to address complications such as flap necrosis, dehiscence, fistula and stricture.6–13 Here we present our approach to reconstructions using the double paddle myofasciocutaneous ALT flap as our workhorse for various combinations of pharyngectomy defects. We share our experiences and thoughts on critical factors for success and outline our operative sequencing and nuances.
Patients and methods
This is a retrospective review of 14 consecutive patients undergoing reconstruction of TLP defects using an ALT free flap from January 2017 to November 2019 at St Vincent’s Hospital Sydney, Australia. Data was extracted from a prospective collection database including patient demographics, perioperative information and surgical data. Follow-up data were derived from medical records.
Surgical technique
Preoperative
Preoperative perforator mapping is performed with a handheld Doppler in a standard fashion. Either thigh is used, though the side that permits concurrent raise (that is, a two-team approach) is preferred if suitable perforators allow.
Flap raising
The flap is raised in a routine technique, from the anterior edge in the subfascial plane (Figure 1). If at least two suitable perforators are identified from the descending branch of the lateral circumflex femoral artery (dbLFCA), and these are separated to adequately allow a double paddle design, then the pedicle of the dbLFCA is used. If only a single perforator is identified, then the transverse branch of the lateral circumflex femoral artery (tbLCFA) is taken in addition. In this scenario, the dbLFCA is used for the distal paddle and the tbLFCA is used for the proximal paddle. When taking both the transverse and descending systems, the two are followed to a confluence at the lateral branch of the circumflex femoral artery (LCFA) and vein. This generally requires sacrifice of the branches to the rectus femoris and vastus intermedius, as well as nerves passing between.

The flap is raised without making the posterior incision and without splitting the skin into paddles. Once the resection is completed, the defect is templated using a material drape. The superior circumference of the defect is frequently large and may be over 20 cm long. The template is placed on the thigh and orientated to facilitate a double paddle while allowing direct closure of the donor site. This can be positioned longitudinally, transversely or obliquely over the proximal perforator.
The pharyngeal component of the reconstruction is designed using the proximal paddle and this is generally taken as a fasciocutaneous element (Figure 2). The distal component is used to fill dead space, resurface the neck if required, and to serve as an external monitor of flap perfusion. The flap is harvested as a chimeric myofasciocutaneous flap with a two perforator-perfused skin paddles and a segment of distal vastus lateralis muscle.
_and_.jpg)
The final cutaneous paddle incisions are made and the posterior dissection completed, keeping a 1 cm lip of fascia lata. In the case of a circumferential defect, the proximal paddle is tubed in situ over a 20 cc syringe while the flap remains perfused and attached in the thigh. The proximal skin paddle is tubularised using a single layer of interrupted 3-0 VICRYL® (Ethicon Johnson-Johnson Surgical Technologies, Sterilmed, 5010 Cheshire Parkway, Suite 2, Plymouth, MN 55446, USA) horizontal mattress sutures (Figure 2).
Flap inset
For a circumferential reconstruction, the cranial inset is performed first using a combination of 2-0 and 3-0 VICRYL® sutures. This starts posteriorly then proceeds to the lateral pharyngeal walls and to the base of the tongue anteriorly. It is important that muscle is included in suture bites in addition to mucosa.
The tube is designed and orientated so that the vertical seam sits laterally on the contralateral side to the microanastomosis. This is later overlaid by vastus lateralis muscle from the distal paddle. The microanastomosis is then performed using a venous coupler where possible, and 8-0 Nylon for the arterial anastomosis.
In partial pharyngectomy defects, the intact strip of pharynx is not excised. Native pharynx mucosa naturally dilates, which reduces the risk of neopharynx stenosis. Secondly, an intact strip prevents ‘T-Junctions’, which carry a higher risk of necrosis and therefore leakage. The inset to this defect begins by suturing first along one lateral longitudinal side, then the cranial end working from one side to the other, then the second lateral longitudinal side. Microanastomosis is performed after cranial flap inset.
The caudal inset to the oesophagus is performed after the microsurgery is completed, again using 3-0 VICRYL® vertical mattress sutures. A nasogastric tube is passed prior to the caudal anastomosis to facilitate feeding as well as minimise synechiae and consequent stenosis. A soft silicon Montgomery® Salivary Bypass Tube (Teleflex Medical Europe Ltd, IDA Business and Technology Park, Dublin Road, Athlone, County Westmeath, Ireland) was used in one case only.
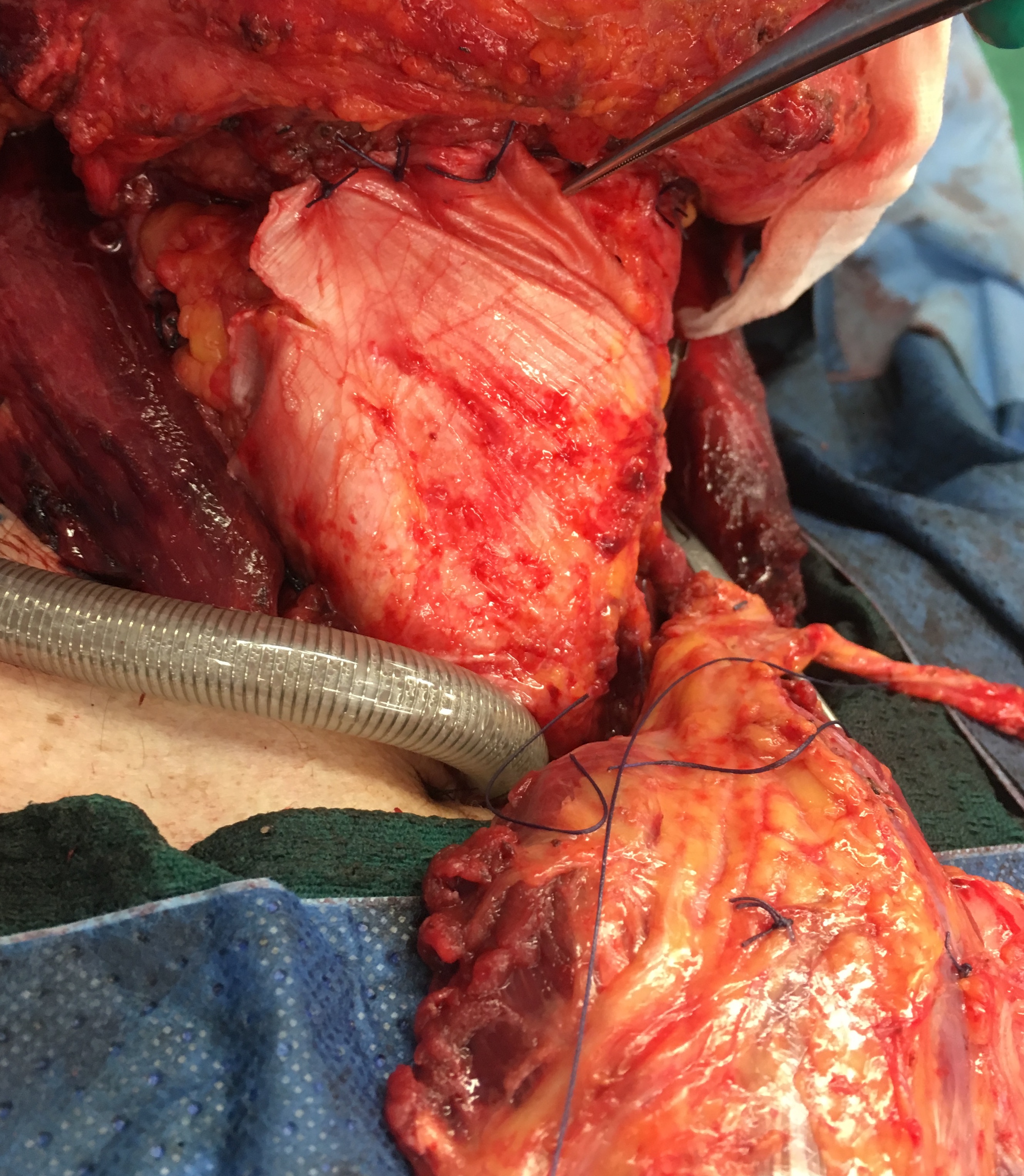
The fascia lata is suspended around the hyoid bone if present, or to the base of tongue muscles using heavy VICRYL® sutures. This is performed to reduce tension and traction on the skin-mucosal repair with tongue movement postoperatively. This fascial suspension aims to have a stress-shielding effect to protect the visceral reconstruction (Figure 3). At the caudal end, a tongue of fascia lata is sutured into a recess between the trachea and oesophagus producing an interface to prevent tracheoesophageal fistula.

The vastus lateralis muscle included with the distal skin paddle is suspended cranially from the suprahyoid muscles and laterally to the sternomastoid to fill the dead space and cover the vertical seam of the neopharynx. The corresponding skin paddle may also be utilised for neck resurfacing if required. If neck resurfacing is not required, the skin paddle is inset as an external monitor in the lateral neck. This paddle can eventually be excised if, after muscle atrophy and possible adjuvant radiotherapy, excessive bulk remains.
Suction drains are placed in the sub-sternomastoid channels bilaterally. The skin is closed in layers and covered in 1 per cent chloramphenicol ointment.
Postoperative
Patients are admitted to ICU for invasive ventilation overnight. Transfer to a tracheostomy ward is encouraged if safe from postoperative day one. Routine flap observations are performed hourly for the first 48 hours then decreased incrementality. Mobilisation from day one is permitted. Modified barium swallow (MBS) testing is performed at approximately day 14 and if successful an oral diet commences.
Results
General
Between 2017 and 2019, 14 patients underwent reconstruction using the described chimeric ALT free flap to TLP defects at St Vincent’s Hospital Sydney (Table 1). All patients were discussed at a multidisciplinary team meeting prior to surgery. All flaps were based on the LFCA system.
Patients averaged 61.1 years of age. There were two females (14%) and 12 males (86%). Ex- or current smokers made up 85.7 per cent of patients with an average of 32 pack years.
Primary resections constituted 13/14 (93%) of procedures, with one case (7%) for recurrence. Two cases (14%) were salvage procedures following chemoradiotherapy.
Previous radiotherapy had occurred in four cases (28.6%). Postoperative radiotherapy was administered to 9/14 (64.3%). One patient underwent palliative radiotherapy only after spinal metastases occurred.
The donor site was closed primarily in all 14 patients.
Inpatient outcomes
All 14 (100%) flaps survived. There were no returns to theatre for microvascular complications.
Initial MBS was performed in 10/14 (71.4%) of patients. One patient was unable to tolerate the procedure and three patients were assessed clinically.
Leakage occurred in one patient 1/14 (7.1%) and was diagnosed by performing the MBS on day 22.
Table 1 summarises all cases, however, the following cases warrant further evaluation:
Case 6: Pharyngocutaneous fistula
Initial MBS on postoperative day eight was negative; however, the patient went on to develop neck swelling and swinging fevers. A repeat MBS performed on day 22 demonstrated a fistula. After the administration of intravenous antibiotics and drainage of a collection associated with the fistula, a follow-up MBS on day 26 was negative. The patient subsequently progressed well and was discharged on an oral diet. They then experienced stomal dehiscence requiring a two-stage supraclavicular flap reconstruction as an outpatient and at an 18- month follow-up remained complication-free.
Case 7: Reconstructive site haematoma requiring evacuation
Rapid neck swelling clinically diagnosed as a haematoma was detected on postoperative day one. Intraoperatively, the microanastomosis was noted to be uninvolved and ooze from the muscular component of the flap was determined as the cause. The admission was subsequently unremarkable.
Case 8: Neck wounds
Two small neck wounds failed to heal postoperatively. The monitoring paddle was mobilised to resurface this area.
Case 9: Postoperative emesis
Day one postoperatively, the patient began vomiting per oral (through the tubed flap) although no leak occurred.
Case 10: Base of tongue dehiscence
A minor dehiscence and collection was noted on routine postoperative examinations as an inpatient. The patient was treated with intravenous antibiotics and non-operative management. The dehiscence healed and the patient was discharged on oral intake at postoperative day 22.
Donor site complications occurred in 2/14 (14.3%) of inpatients. These included one seroma requiring aspiration and one donor site that required a split skin graft and dressing using V.A.C® GRANUFOAM™ Dressing (3M KCI, 3M Center, St Paul, MN, 55144-1000, USA).
Outpatient outcomes
Patients were followed up for an average of 13 months (range 1–28). Outpatient dilations post-surgery occurred in 7/14 (50%) of cases.
Additional related outpatient operations occurred in one patient who underwent a two-stage supraclavicular flap for stoma wound dehiscence, as mentioned above.
One patient was lost to follow-up.
Discussion
Total laryngopharyngectomy reconstruction is a high-risk procedure and presents a challenging reconstructive problem. Being increasingly utilised as a salvage procedure, TLP patients have a compromised local healing environment associated with complications of chemoradiation, including contractured, sclerotic tissue planes and fragile blood vessels in addition to systemic sequelae of malignancy such as nutritional deficits which hinder healing and recovery. These issues heighten the complexity of the reconstruction.
Various flap modifications have been described, each aiming to reduce complications,6–13 including soft tissue coverage of great vessels to reduce carotid artery blowout, reduced stricture formation and dysphagia,6,8 not to mention improved flap monitoring.14
Preventing dehiscence and fistula
We have designed several modifications to reduce fistula formation. Firstly, reinforcing the suture line by incorporating a layer of vastus lateralis prevents food, oral flora, enzyme-rich saliva and gastric juices from leaking into the neck. This models the approach described by Moradi and colleagues where prophylactic pectoralis muscle covers jejunal free flap (JFF) for TLP.15 Others incorporating vastus lateralis in the reconstruction report some improvement in fistula rates: Kao and colleagues found fistula rates to be lower when muscle was included (25% versus 36.8%),16 and although this was not statistically significant (p = 0.5), the authors propose the reduced dead space may reduce fluid collection and fistula formation.12 In 2014, Ooi and colleagues reported fistulas occurring in 3/13 (23.1%) patients who had TLP with a chimeric ALT free flap including the muscle. Cases in this study were salvage procedures post-radiotherapy, which has been found to significantly increase rates of fistula formation.11
Kao and colleagues and Oh and colleagues propose similar logic by using an additional fascial layer or by performing a double layer suture line.12,14 However, our unit does not perform a circumferential fascial layer for concern that it may restrict normal postoperative oedema, which may compromise flap viability.
Secondly, we aim to reduce tension along the anastomosis by suspending the flap on the hyoid or muscles of the base of the tongue as a ‘stress shield’. The reduction in tension in this fashion aims to reduce dehiscence at the proximal and distal anastomoses. Oh and colleagues’ techniques for reducing tension include a graded seating approach; however, we prefer our technique as it allows us to mobilise our patients from day one postoperatively.14
Thirdly, we preserve the lingual arteries. Native arterial supply to the base of the tongue and hypopharynx maximises perfusion to a zone susceptible to dehiscence and therefore fistula formation.
Lastly, positioning of the vertical seam opposite to the microanastomosis is planned as a final barrier to prevent flap complications. With this position, any fistula related to the vertical seam is directed away from microanastomosis. Theoretically, this will facilitate safer percutaneous or operative intervention as well as decrease the likelihood of a leak into other hazardous and inaccessible spaces such as the mediastinum.
Flap monitoring
The rationale for a technique that facilitates skin paddle monitoring is that buried flaps are more at risk of flap loss than those that are non-buried.17,18 Many methods have been investigated for the monitoring of buried free flaps, including implantable Doppler, thermography, fluorescence imaging and microdialysis; however, each has drawbacks such as high costs, the requirement for specific technical expertise and results being susceptible to subjective interpretation.19–22
We find that the simplicity of a skin paddle with clinical observation and handheld Doppler checks provides the most reliable method of assessing perfusion in a ward-based setting with an acceptable cost outlay. Recently, Oh and colleagues reported a chimerised flap that also provides skin paddle monitoring.14 Depending on the size of the skin paddle left for monitoring, it may be excised under local anaesthetic or kept for use in neck resurfacing (Figure 4).

Neck resurfacing
Five patients had neck surfacing included in the primary reconstruction. Most of these patients had prior radiotherapy (3/5, 60%), which had led to contractured and attenuated anterior neck skin that was resected at the time of tumour extirpation. Therefore, when neck skin was compromised, a chimeric flap skin paddle was inset among healthier skin. In one case, chimeric muscle was inset and a split skin graft applied. There have been previous reports of chimeric flap components being utilised for neck resurfacing23,24 as well as modifications based on de-epithelisation and skin paddle folding.8,14 We prefer the chimeric approach, which by design has no communication between the neopharynx and outer skin.
Chimeric flap design also offers greater freedom in neck resurfacing. This became evident when one patient experienced wound dehiscence during their admission, which was repaired with mobilisation and re-inset of this external skin paddle.
Stricture
Throughout the literature, stricture is among the most common complication of TLP. Strictures requiring outpatient endoscopic dilations occurred in 7/14 (50.0%) of patients. These results are inferior to the proportion reported in a 2019 review, which reported an average stricture rate of 59/316 (18.7%), although the definition of ‘stricture’ was not clearly outlined (for example, clinical, radiological, endoscopic) and the average follow-up period was not reported.16 However, in a 2015 study by Tan and colleagues, endoscopically diagnosed stricture occurred at a rate of 8/21 (38.1%), while others have reported rates as low as 0.0 per cent in small series.13,24,25 Our higher rate of stricture may be related to the method of detection, via endoscopy, as opposed to less sensitive methods such as MBS. It is also possible that a high rate of postoperative radiation (64.3%) of the neopharynx contributed. While in Koh and colleagues’ 2019 review, the JFF reported lower rates of stricture, at 10.9 per cent.16
Donor site morbidity
In our study, complications were uncommon and minor despite very large skin paddles being harvested. Patient body habitus was frequently wasted and thus thin thighs with excess skin favoured primary closure; however, it should be noted that in obese patients, the tubed ALT may not be a feasible option. In these circumstances, RFFF is our second preference followed by JFF. While JFF has low rates of stricture, donor site morbidity and potential complications cannot be completely disregarded. In the largest study of JFF to date, Perez-Smith and colleagues report complications of ileus, bowel obstruction, hernia, intraperitoneal bleeds, intussusception and wound dehiscence reaching 4.35 per cent.26
We have not observed mobility issues despite reports of potential compromise of the rectus femoris circulation with division of the dominant branch to this muscle. However, we aim to preserve any distal vessels to this muscle for this reason. Similarly, although initially concerned at the inevitable loss of quadriceps strength resulting from sacrificing both nerves to vastus intermedius and vastus lateralis, we have observed no major impedance in mobilising or knee stability in our patient cohort.
Conclusion
The ALT flap is a workhorse reconstructive flap option for total laryngopharyngectomy defect reconstruction. The modifications performed by our unit involve harvesting an off-centred fascia lata suspension as a ‘stress shield’, a strip of vastus lateralis to reinforce the vertical seam, and a chimeric skin paddle for monitoring and/or neck resurfacing. We have now demonstrated with 14 consecutive cases that this method provides a reliable reconstruction which is resilient to the described difficulties of this reconstruction.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship and/or publication of this article.
Revised: 2021 August 8 AEST