

Introduction
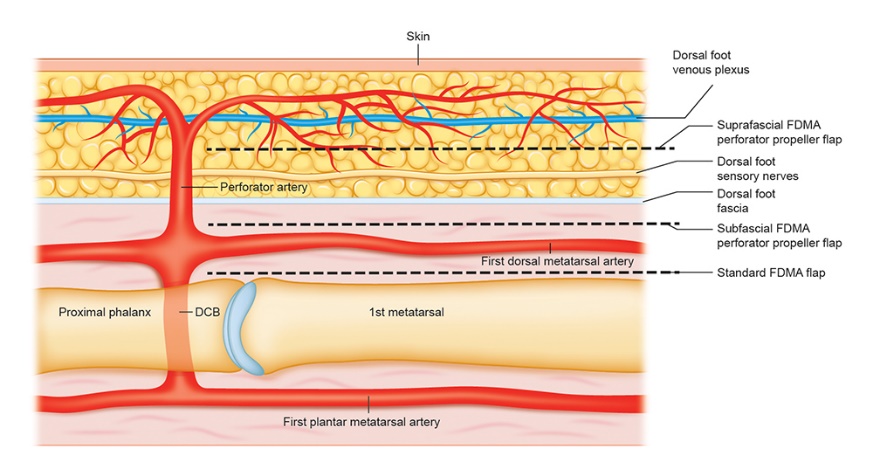
Coverage of distal foot and toe tissue defects is challenging regardless of the cause (for example, trauma, oncological resection, infection or burn injury). Vascularised locoregional flaps based on the dorsalis pedis artery or first dorsal metatarsal artery (FDMA) are often used for pedal tissue coverage. These flaps, however, sacrifice a major artery to the foot and have significant donor site morbidity owing to skin grafting of the secondary defect. We describe a variation of the traditional reverse FDMA flap; a suprafascial propeller flap based on an FDMA perforator (Figure 1) was used for great toe resurfacing after excision of a locally invasive squamous cell carcinoma. We outline potential advantages of this technique.

Case
A 76-year-old Caucasian woman underwent wide local excision of a biopsy-proven squamous cell carcinoma of her right great toe. Excision included the entire nail complex leaving exposed the proximal and distal phalanges, and the intervening interphalangeal joint.
The dorsalis pedis artery and its continuation FDMA, and a distinct suprafascial cutaneous perforator at the junction of the FDMA and distal communicating branch, were mapped and marked out preoperatively using duplex ultrasonography (Figure 2a). After the interphalangeal joint was arthrodesed, a propeller flap (15 mm × 65 mm) based on the perforator, was raised from proximal to distal in a suprafascial plane until the distal communicating branch perforator was encountered (Figures 2b and c). More proximal cutaneous perforators were ligated. The deep and superficial peroneal nerves were preserved as dissection was limited to a suprafascial plane.
_to_be_excised_inferior_to_great_toenail_is_marked__first_dorsa.png)
The flap was transposed 180° clockwise in a standard propeller fashion and inset into the defect. The reach of the flap extended with ease to the tip of the great toe. The majority of the donor site was primarily closed, and a small split skin graft was required at the site of transposition to cover the adipose tissue around the perforator pedicle. The flap and skin graft were well healed at nine months postoperatively (Figure 2d).

Discussion
Distal foot tissue defects can be reconstructed using skin grafting, locoregional flaps and free tissue transfer. Traditionally, locoregional flaps, centred on the dorsalis pedis axis, entail subfascial dissection, leaving a large, concave secondary defect that necessitates skin grafting onto midfoot periosteum and, often, sacrifice of the deep and/or superficial peroneal nerves.
This subfascial approach has been well described with satisfactory outcomes.1–4 Hallock described two successful subfascial FDMA perforator propeller flaps for great toe defects in 2016 in patients who had bone and interphalangeal joints exposed, one case due to infection, the other due to trauma.1 Both patients had good clinical outcomes at the 9–12-month follow-up. Limthongthang and Eamsobhana also used the subfascial FDMA perforator flap for coverage of great toe defects (including bone exposure), dissecting down to dorsalis pedis vessels. Both cases achieved good results at the 12-month follow-up.2
While there have been reports of FDMA propeller flaps for distal foot reconstruction, to our knowledge there have been no reported cases of using a suprafascial design of the FDMA perforator propeller flap.
In this case report, we have applied the perforator flap concept to the traditional reverse FDMA flap and described an axial cutaneous perforator flap for coverage of a distal foot defect. The benefits of this modified propeller flap are several-fold. Suprafascial flap elevation allows transfer of a superthin flap, which is especially useful for resurfacing dorsal digital defects. The suprafascial FDMA propeller flap does not entail sacrifice of the dorsalis pedis artery and preserves important dorsal foot sensory nerves. Lastly, it preserves deep fascia on the foot, and creates a more favourable secondary defect for grafting if the donor site cannot be closed primarily.
The typical anatomy of the FDMA consists of perforators that are found superficially in the distal space between the first and second metatarsal bones1 (Figure 1). The most distal of these cutaneous perforators is reliably present between the heads of the first and second metatarsals, and this is key for a viable vascularised FDMA perforator propeller flap.5 However, it should be noted that the communicating vessel between dorsal and plantar arteries is absent in 15 per cent of patients.6 Vascular anatomical variations should not be a problem with our suprafascial design as it is still possible to use a perforator directly from the FDMA to perfuse a FDMA perforator propeller flap, even in the absence of a distal communicating branch.
Conclusion
Here we have described an alternative option for vascularised coverage of distal foot defects. The suprafascial approach for this FDMA perforator propeller flap allows a safer dissection, a thinner flap to resurface defects with a higher likelihood of flap success and provides a better graftable bed if donor sites are unable to be primarily closed. This approach also demonstrated long-term satisfactory functional and aesthetic outcomes for big toe salvage.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.
Revised: September 16, 2021 AEST