Introduction
Breast cancer (BC) is the most commonly diagnosed cancer among women, with approximately 3000 women diagnosed in New Zealand (NZ) every year.1,2 While the rates of BC diagnoses are increasing,3 survival rates have also improved, with an approximate five-year survival rate of 90 per cent following treatment.4 Surgery, which can include partial or full removal of the breast, is the mainstay of treatment for BC.5 Post-mastectomy reconstruction is an integral part of the treatment process as it helps to improve the physical, physiological and social aspects of everyday life of women impacted by BC.6 Therefore, it is now firmly established as part of BC care in well-recognised guidelines in NZ.7
Currently, reconstructive options post-mastectomy are implant or flap-based.8 Donor site morbidity and the time to recovery make flap-based reconstruction an unattractive option. It is a technically demanding procedure and is not deemed safe for patients with comorbidities such as obesity and diabetes.9 This develops a level of inequity in access to reconstruction options between different populations in NZ, such as Māori and Pasifika, which are reported to have increased levels of these comorbidities.10 Implant-based reconstruction is associated with longer term complications, including the development of capsular contractures, which can lead to poor aesthetic outcomes, pain and the requirement for multiple procedures.11,12 Recently, anaplastic large cell lymphoma and breast implant-associated illness have become increasingly topical in the literature, creating anxiety for women around implant-based reconstruction.13
The role of autologous fat grafting (AFG) in breast reconstruction is largely limited to the improvement of implant-based reconstructions, especially following adjuvant radiotherapy, but also as an adjunct to improve contour defects related to flap-based reconstruction. Controversy around implants and the opportunity cost for flap reconstruction makes the ability to achieve whole- breast reconstruction using fat more desirable.
Autologous fat grafting involves harvesting fat using liposuction from a donor site and reinjecting the graft into the chest wall.14 There is low donor site morbidity, rapid recovery and evidence that it alleviates pain and fibrosis associated with radiation.15 The one drawback of AFG is the unpredictability and wide variability in graft survival, with retention rates reported between 30 and 70 per cent of the original grafted volume.14 In order to obtain the desired results, multiple surgeries must be undertaken, necessitating a motivated surgeon, and patient. Additionally, these multiple surgeries use resources that in a public hospital setting are already scarce. Thus far, most studies have compared harvesting methods and processing techniques for AFG retention; however, in order to improve graft retention rates, standardised methods for the measurement of grafts must be developed first.
This pilot study aimed to assess AFG retention via MRI in a pilot cohort of women undergoing AFG in a single centre in NZ.
Materials and methods
Recruitment
Twenty patients requiring mastectomy as part of their surgical treatment were prospectively enrolled in a wider study. Of these, six patients who were suitable for immediate breast reconstruction (IBR) with implant were selected to take part in this pilot study. The six women underwent MRI pre- and post-AFG. The AFG was performed at second-stage surgery, at a minimum of three months post-IBR with implant in order to allow a capsule to develop and a layer in which grafting could occur. An MRI was performed pre-graft, prior to the first session of AFG, and three months post-graft. Patients were eligible if they were undergoing breast surgery at a single centre in NZ. Patient demographic and clinicopathologic information was collected from hospital records for all 20 patients. This study had ethical approval from the Health and Disabilities Ethics Committee, NZ (19/CEN/23) and all participants provided written informed consent.
Operative technique
All procedures were performed by a single surgeon. Antibiotic prophylaxis (cefazolin) was routinely administered prior to induction of general anaesthesia. Donor site areas were marked in the preoperative bay, and were dictated by donor site availability. The pre-marked areas were infiltrated with a solution of 1mg adrenaline in 1L normal saline through 2 mm stab incisions. Fat aspiration was performed using a ‘fat trap’ as described previously by the Paris Breast Center, France.16 This entailed a 4 mm Byron teardrop cannula with a curettage tip connected to a sterile drain bottle, which itself was connected to a liposuction machine.
After completion of aspiration, the bottle was left to decant for 10 minutes, allowing separation of a bottom liquid layer. The bottom layer was discarded and the remaining lipoaspirate was used for injection. Several incisions were made over the reconstruction and the lipoaspirate was injected globally in a multi-plane fashion: subdermal, extracapsular and into pectoralis major with care not to bolus fat in any particular area.
Volumetric assessment
Assessments were performed at baseline and three months post-AFG using the 15-channel breast coil in conjunction with a Siemens’ MAGNETOM Skyra 3T MRI scanner (Siemens Healthcineers AG Erlangen, Germany). Pre- and post-contrast images were obtained as part of a diagnostic scan, which included the administration of weight-related gadolinium (Dotarem, Guerbet Australia Pty Ltd, Lane Cove West, 2066, New South Wales, Australia). Three-dimensional T1 volumetric gradient echo sequences were performed to increase measurement reliability, as 2D sequences would have resulted in slice gaps.
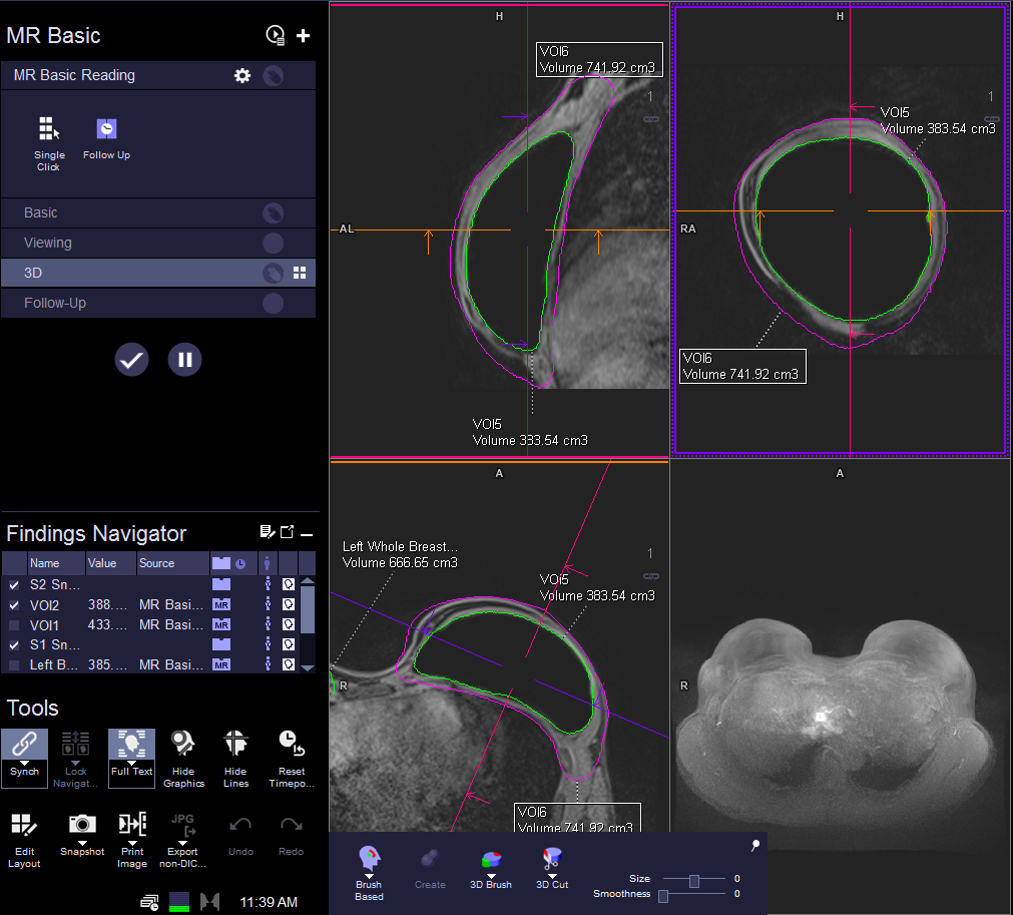
The breast area was outlined for sections at intervals, which included the skin and breast footprint, based on consistent anatomical landmarks such as the sternum, manubriosternum, nipple and inframammary fold. All volumetric analysis was interpreted by an experienced radiologist with a breast fellowship and double determination was performed with the charge MRI medial imaging technologist. The MRI volumetric analysis was performed using Siemens’ syngo.via software (Siemens Healthcineers AG Erlangen, Germany) post-processing package, which is part of the syngo.MR 3D lesion segmentation tool (Figure 1). The pre- and post-surgery MRI images were loaded into this platform and the areas of the breast and implant were calculated in three planes over multiple slices. With breast and implant areas defined on each slice, the software then calculated the breast and implant volumes for each MRI, allowing comparison of pre- and post-surgery volumes excluding the implant.

Results
Cohort characteristics
Demographic and clinicopathological characteristics of all 20 women were collected from patient records as part of a wider study. A detailed outline of demographic and clinicopathological characteristics of the cohort is set out in Table 1. All patients in the MRI sub-group (n = 6) underwent implant-based reconstruction and had AFG over implant as part of their second-stage reconstruction.
Volumetric analysis
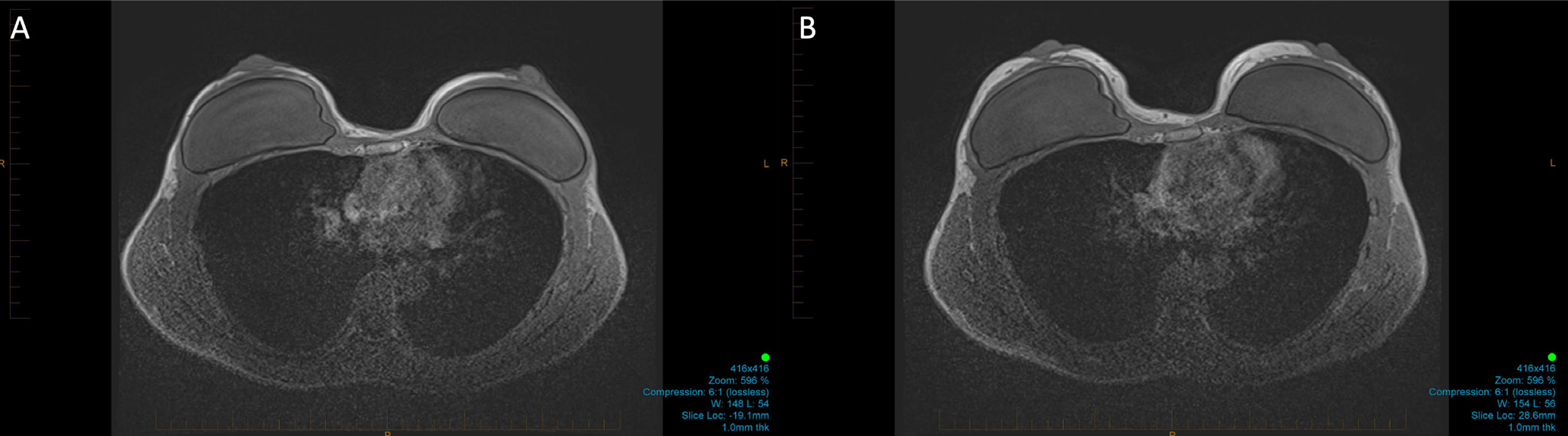
Volumetric analysis was performed on seven breasts from six patients. The volume of fat injected ranged from 150 to 200 cm3. All patients had a net gain in volume of tissue at three months post-procedure with a mean of 123.6 ± 56.07 cm3. The percentage retention by volume ranged from 30.0 to 104.7 per cent with a mean of 73.72 ± 28.97 per cent (Table 2). Interestingly, the patient who had AFG in both breasts had substantially different retention rates at 104.7 per cent and 56.0 per cent in the right and left breast respectively. Figure 2 shows representative MRI images of pre- and post-AFG. Additionally, there was no association between fat graft retention and treatment characteristics, specifically requirement for chemotherapy, radiotherapy or hormonal manipulation.
_mri_pre-_and_(b)_post-afg._bilateral_immediate_implant_reconstruction_baseline_scan_(a)_a.png)
Discussion
This study demonstrates that measuring AFG retention over an implant is feasible. We performed systematic MRI pre- and post-graft over breast implants in six patients, with a measured graft survival ranging from 30 to 100 per cent and a median retention volume of 54.2 per cent. This demonstrates the variable success of AFG in women undergoing implant-based IBR at a single centre in NZ, although our percentage retention is in line with reports in the literature. To our knowledge, this is the first local study to measure retention rates of grafts placed over implants via MRI.
Following MRI analysis, all patients had a net gain in volume post-procedure; however, the percentage of retention ranged substantially. This aligns with current literature, which reports 30–70 per cent graft retention, and reinforces caveats around the use of AFG for whole-breast reconstruction.14 At present, it is really only possible to routinely graft fat into the pectoralis major at the time of mastectomy as fat cannot be grafted in the mastectomy cavity itself. A graft needs scaffolding with vascular supply in order to survive. We grafted 150–200 cm3 of fat over the implant in all women, with an average volume of 168.33 cm3. Using a median graft survival of 54 per cent, three sessions of AFG would be required, three to six months apart, to achieve whole-breast reconstruction to an A-cup breast size. For those patients who desire whole-breast reconstruction using AFG, this is an important demonstration of what is achievable over time; an A-cup breast reconstruction over three to four operations spread out over 12 to 18 months. Due to the limits of AFG, it is routinely used in second-stage reconstruction to improve the outcome of implant-based reconstruction. Autologous fat grafting is a relatively simple procedure with low risk, and substantive quality of life gains due to the demonstrable reversal of radiotherapy-related fibrosis and pain.17 Several units now include routine fat grafting as part of the treatment schedule for implant-based reconstruction where radiotherapy has been required.18
The ability to more accurately predict fat graft survival and the factors that may influence this is important to create more realistic expectations for women, and also to lower the threshold to achieving more predictable whole-breast reconstruction in a timely manner. In this cohort, we did not find a difference in graft survival by patient or treatment characteristics, namely the requirement for chemotherapy, radiotherapy or endocrine manipulation. However, this cohort is very small, and larger studies should take into account patient, disease and treatment characteristics which may contribute to graft success.
Multiple studies have examined the role of harvest technique and infiltrant solution in graft survival.19 In regard to the technique used in this study, the group from whom the technique originated have previously reported their prospective randomised trial which found no significant difference between decanting and centrifugation in chest wall thickness after post-mastectomy AFG.20 It appears overall, that technique, preparation solution and donor site do not contribute significantly to the variability for graft survival. To our knowledge, no studies have looked at the interaction between donor and recipient site at a molecular level with a focus on the milieu that drives the alleviation of fibrosis and scarring after treatment.
However, a consistent gold-standard measurement technique is required in order to allow for reproducible research into AFG retention, as well as being able to measure retention rates in the clinic. One of the major setbacks for such AFG studies is the lack of consensus on the accurate measurement of retention. A number of studies have successfully used MRI to measure small bolus injections of fat into superficial areas of the body, such as the back of the arm or over a flat surface.20,21 Previous studies have reported difficulty measuring fat graft retention over implants due to changes in contour over multiple points. We used a technique as suggested by Glovinski and colleagues and found that it is feasible to accurately measure graft retention over implant using MRI.22 One potential setback with the use of MRI for AFG measurement is the cost and practicality of the tool. In NZ, MRI is not currently a routine part of the patient care pathway. The introduction of routine MRI following AFG could therefor lead to an increase in the costs and need for specialists, something for which the health system is not currently equipped.
Regardless of whether it is feasible to introduce this into the clinical care pathway, the use of MRI as a measurement tool for graft retention is promising and important for future studies investigating AFG retention. The use of MRI can aid research aimed at developing techniques for consistent, viable graft survival, at which point the need for retention measurement as part of clinical care could become obsolete.
Conclusion
This study demonstrates the feasibility of measuring AFG retention over implant using MRI, as well as confirming variable tissue retention rates. This is an important step towards improving overall graft survival in women undergoing breast reconstruction and all patients who require restoration of form and function after cancer treatment.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
This research was funded by the Breast Cancer Foundation of New Zealand.
Revised: August 13, 2022 AEST