




Introduction
Autologous fat grafting (AFG) has become an increasingly used surgical technique in Australia and around the world. It is a popular surgical option for use in an array of reconstructive, aesthetic and other therapeutic applications.
The recent introduction, in November 2021, of Medical Benefits Schedule (MBS) item numbers in the national health insurance scheme (Medicare) for use in AFG to breast, burns scars and craniofacial defects has refocused attention on fat grafting as an important surgical technique.1 Currently, protocols for best practice are based largely on clinical experience, ad hoc anecdotal evidence or protocols created by commercial entities as a point of differentiation from their competitors.
Despite the variety of broad clinical indications for the use of fat grafting, and an even broader range of clinical techniques described for optimizing fat grafting,2,3 the practice of clinical fat grafting in Australia has not been characterised. To date, little data has been collected or published on fat grafting in Australia and, therefore, regulators and funding bodies are ill-equipped to assess the scope of practice of surgeons and other practitioners who offer fat grafting to patients. Similarly, it is difficult to establish best practice guidelines or recommendations without first understanding the landscape of the practice within our jurisdiction. Importantly, there has been no attempt so far to characterise the practice among plastic surgeons, who are major proponents of fat grafting. One key aspect of understanding best practice, fat graft success rates and volume retention long term is in the process of providing informed consent that is critical to enable patients to make informed decisions regarding their health expectations and outcomes. It is also imperative to better understand the application of the practice now that funding bodies have accepted the liability of paying for fat grafting procedures in certain patient cohorts.
We conducted the most comprehensive clinical survey to date to assess the scope of clinical practice among plastic surgeons in Australia using a validated survey tool.
This article provides a snapshot of fat grafting practice in Australia today and paves the way for further elucidation of AFG in other professional groups. Previously, the only attempt made to characterise the practice of fat grafting was a single question within the ABDR. Part one of this paper presents this previously unpublished data from the ABDR. Part two presents the findings from our clinical survey. We hope that this report will provide the foundations for a more comprehensive study and enable Australian peak funding bodies and regulators to understand the ways in which the practice may be both safeguarded for patient welfare and enhanced when scientific evidence for practices that may improve efficacy come to light.
Methods
Part one
Part one aimed to determine the incidence of fat grafting in breast device insertion surgery from a single question included in the Australian Breast Device Registry (ABDR). The ABDR routinely records details of all surgeries involving breast device insertion, including implants, tissue expanders, acellular dermal matrices or mesh products. The ABDR data collection form records fat grafting used in breast implant surgery under ‘elements of operation’. This part of the form is completed for all operations involving breast implants or tissue expanders recording AFG used at the time of implant insertion, removal or replacement. Data from 2012 to 2020 were sourced from the ABDR. The primary outcomes were the incidence of fat grafting in reconstructive and aesthetic breast device insertion surgeries and incidence of fat grafting in breast device insertion surgeries in previously irradiated breast tissue. The secondary outcomes were operation type for all breast device insertion procedures recorded with fat grafting and volume of fat injected.
Part two
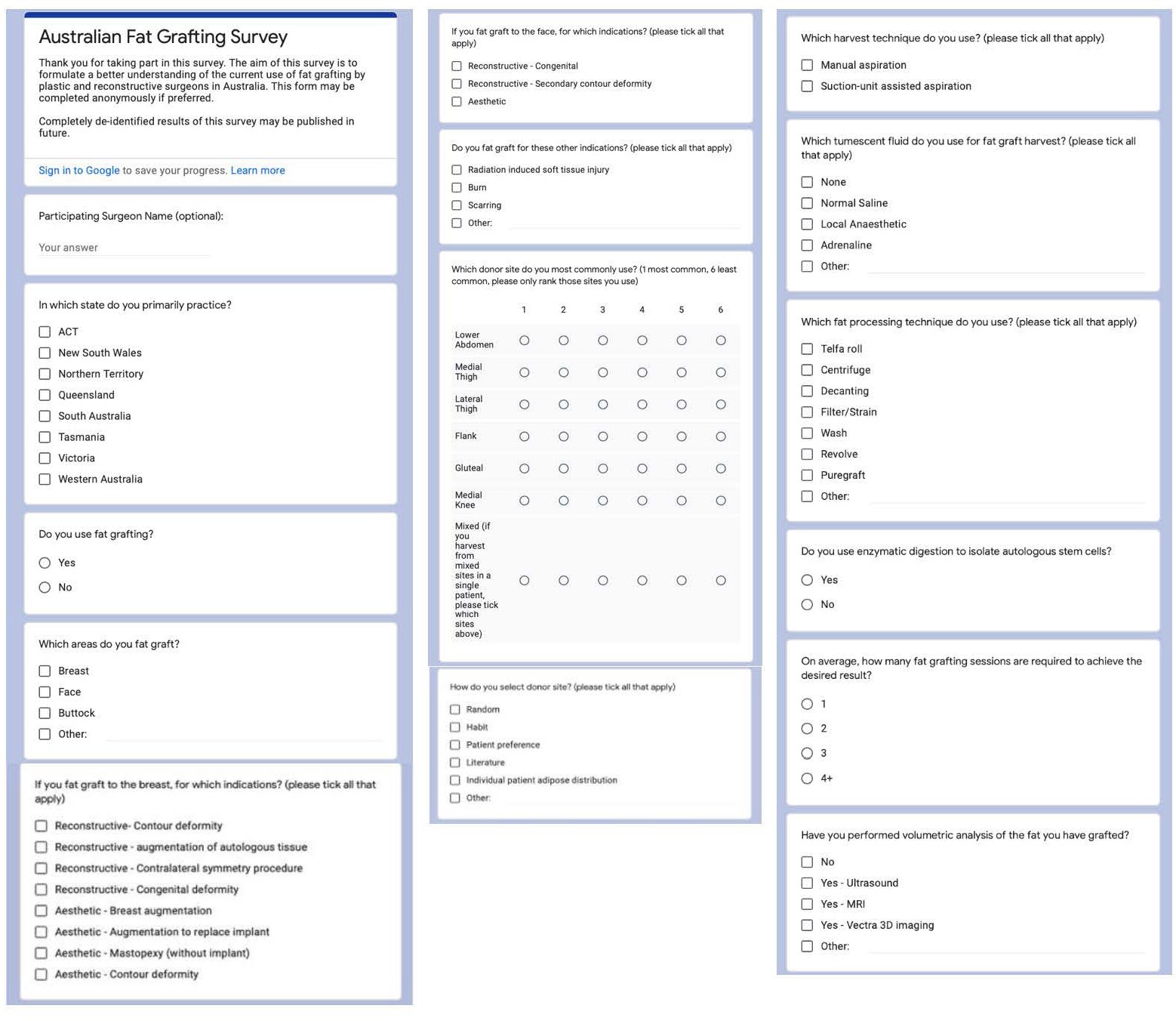
The survey-based study aimed to characterise current fat grafting practice among Australian plastic and reconstructive surgeons. We designed a 14-point questionnaire asking Australian plastic and reconstructive surgeons about their use of fat grafting, area grafted, indications for grafting, donor site selection, harvest technique, processing technique, use of enzymatic digestion, number of sessions required and postoperative volumetric analysis (Figure 1). The study was conducted between July and December 2021. Surveys were distributed via email to 403 active members of ASPS.

This study was approved by the Alfred Health Ethics and Research Governance Committee (HERGC 282/21).
Results
Part one: Epidemiological data from the Australian Breast Device Registry
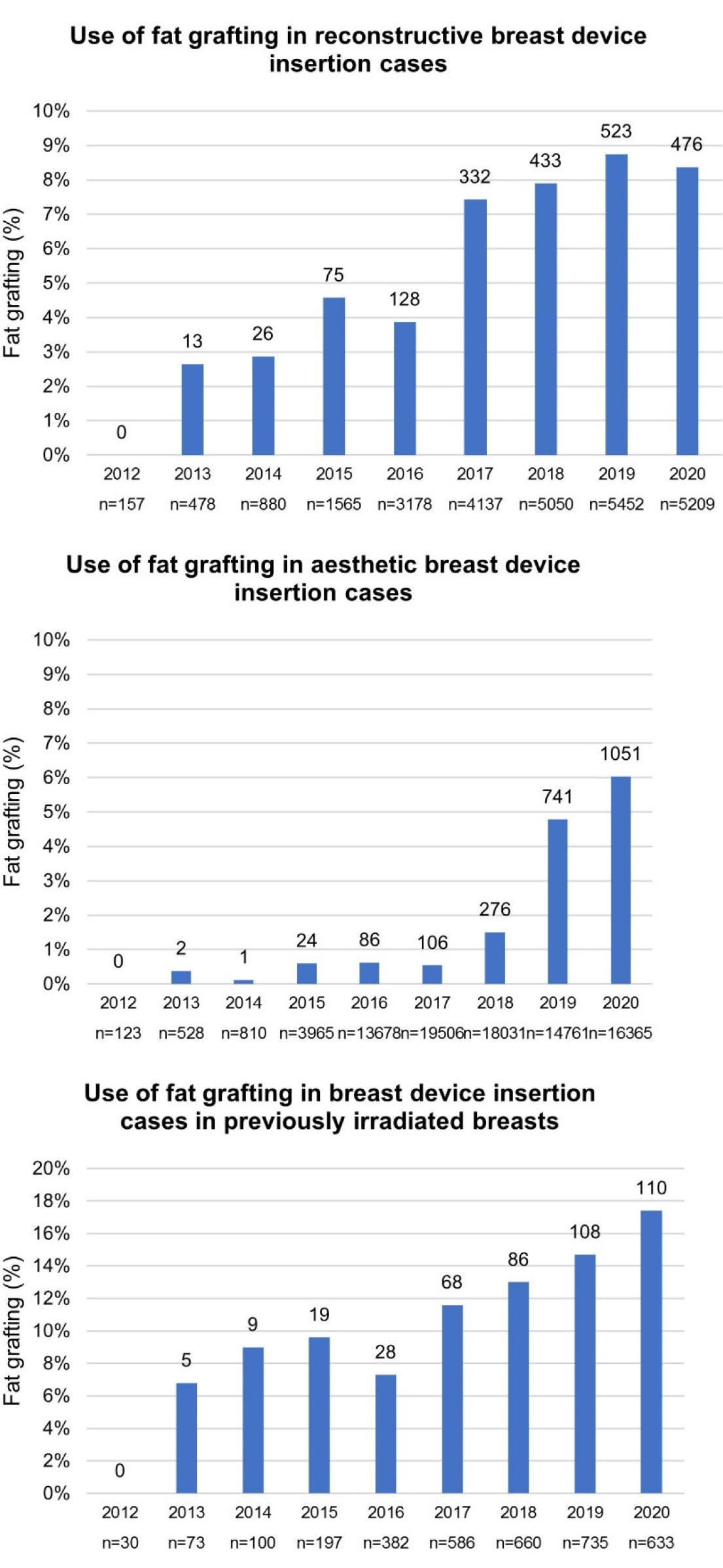
The ABDR form records the presence of concomitant fat grafting at the time of device insertion (yes or no) as well as the volume of fat injected. This is currently the only formal method in place for collection of autologous fat grafting data. The proportion of device insertion procedures with fat grafting increased from 0 per cent in 2012 to 8.4 per cent and 6.0 per cent in 2020 for reconstructive and aesthetic procedures respectively (Figure 2, a and b). Fat grafting at the time of breast device insertion in previously irradiated breast tissue has also increased from 0 per cent to 17.4 per cent in the same seven-year period (Figure 2c). The mean recorded volume of fat injected in breast device insertions was 61.5mLs for reconstructive procedures and 31.4mLs for aesthetic procedures.
_reconstructiv.png)
For reconstructive breast surgery, the majority of procedures reporting the use of fat grafting were for implant replacement procedures (42.8%) followed by tissue expander to implant exchange procedures (38.3%). For aesthetic breast surgery, most procedures with fat grafting consisted of first implant insertions (71.2%) and a smaller proportion consisted of implant replacements (22.3%) (Table 1).
Part two: Fat grafting survey for Australian plastic and reconstructive surgeons
Demographics of respondents
The overall response rate was 21 per cent (84 responses). This response rate carries a 10 percent margin of error with a 95 per cent confidence interval. Eighty-eight per cent of participants reported ‘yes’ to the use of fat grafting while 12 per cent reported ‘no’. Surgeons from all states and territories were represented: ACT (1.2%), NSW (21.4%), NT (1.2%), QLD (10.7%), SA (4.8%), TAS (2.3%), VIC (53.6%) and WA (4.8%). Victorian representation in the survey was higher than its 30 per cent representation of ASPS members.
Indications for autologous fat grafting
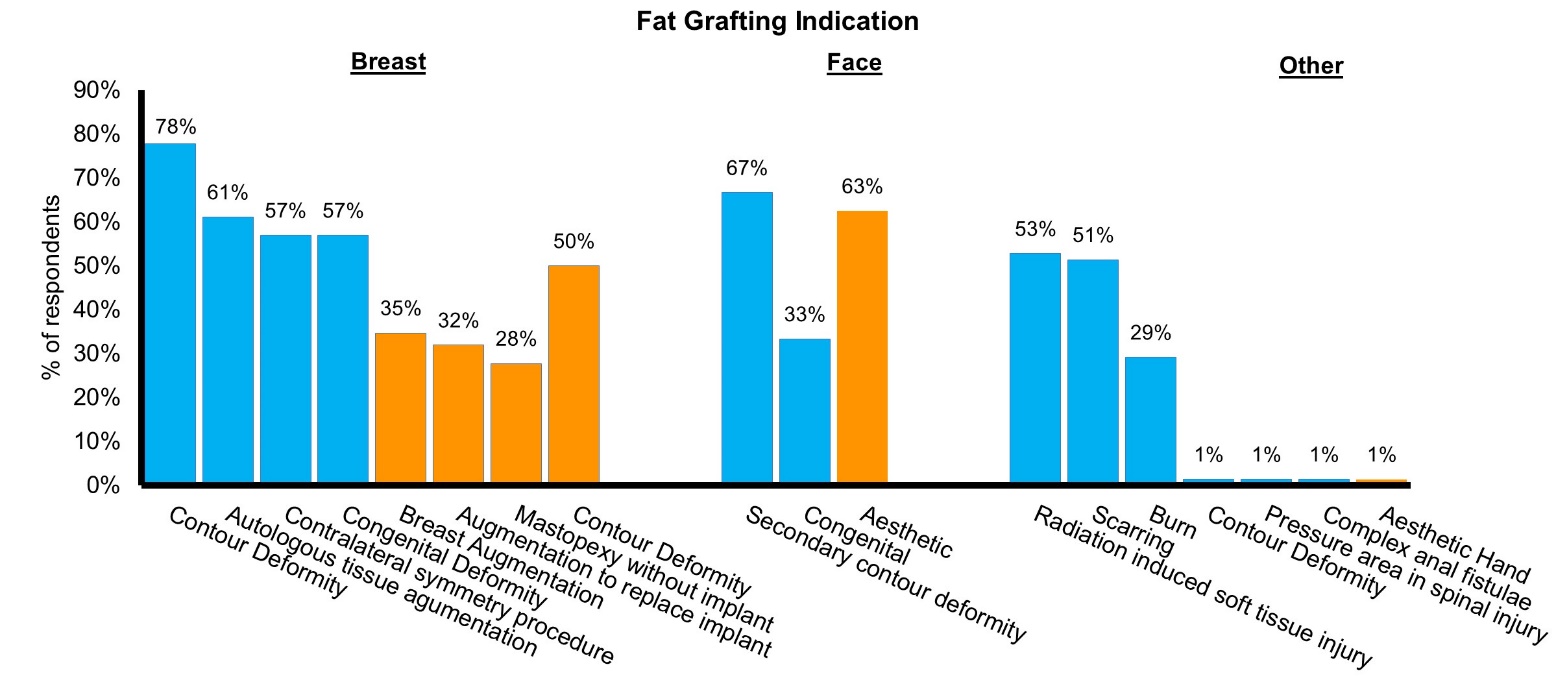
Autologous fat grafting use was reported for 18 indications (Figure 3). All but four of these indications were used by more than 25 per cent of respondents, indicating that AFG is commonly used across a wide range of reconstructive and aesthetic clinical applications.
__aesthetic_(orange)._percentage_of_respon.jpeg)
Autologous fat recipient and donor sites
Fat was grafted to all anatomical regions, with breast (86%) and face (73%) representing by far the most common recipient sites (Figure 4). Donor site selection was largely heterogeneous (Figure 5). There was a minor predilection for lower abdomen, with 51 per cent reporting it as their most used donor site. Lower abdomen (19%), lateral thigh (20%), flank (24%) and medial thigh (28%) were similarly ranked as most used secondary donor site. Twenty-four per cent ranked gluteal as their least used donor site.

_to_6_(least_common)_by.jpeg)
Method of donor site selection
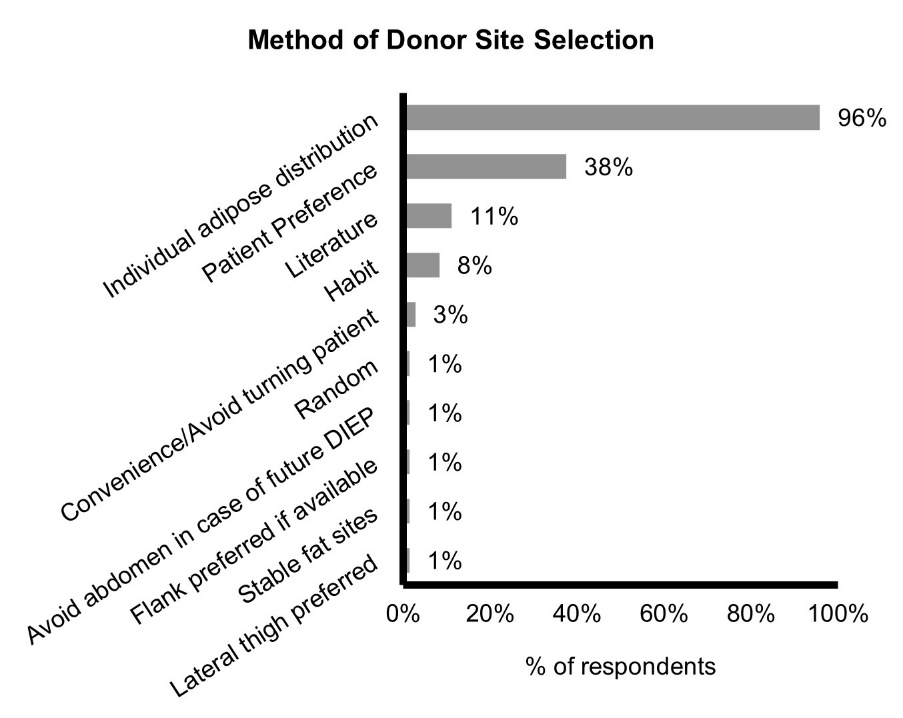
The method of donor site selection was more standardised. Ninety-six per cent used individual patient adipose distribution and 38 per cent used patient preference (Figure 6). Several other less common methods were recorded. Notably, only 11 per cent referred to literature.

Harvest technique
Seventy-four per cent reported use of manual aspiration while 60 per cent reported use of suction unit-assisted aspiration. These percentages indicate that many surgeons use both types of aspiration. The composition of the tumescent fluid used prior to harvest was also variable (Figure 7). The most common ingredients included adrenaline (84%), local anaesthetic (68%) and normal saline (61%). A number of other ingredients were used less frequently. Only 1 per cent (1 respondent) reported use of enzymatic digestion to isolate autologous stem cells.

AFG processing and postoperative course
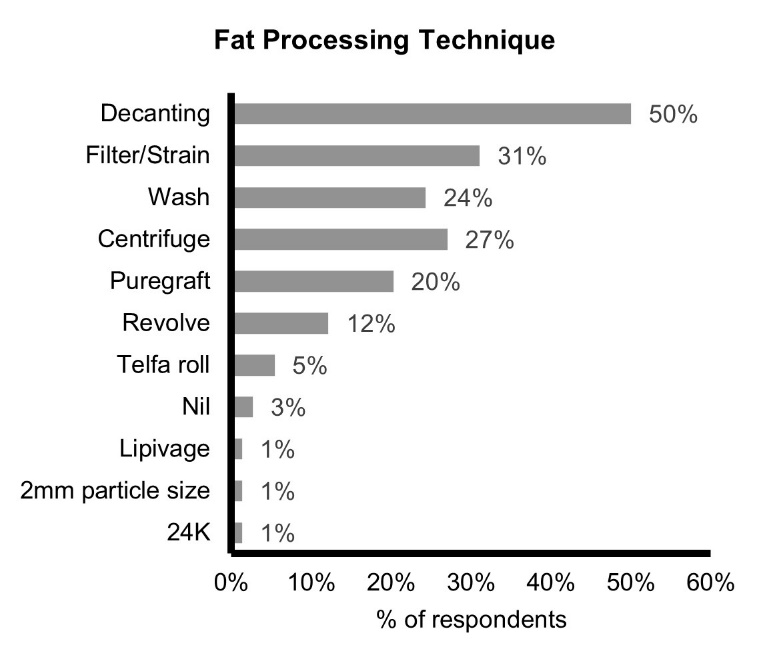
The techniques used for fat processing were also highly variable. The most common processing techniques included decanting (50%), filtering or straining (31%), washing (24%), centrifugation (27%) and proprietary methods including Puregraft (Solana Beach, California 92075, USA) (20%) and Revolve (Allergan Australia Pty Ltd, North Sydney, New South Wales, 2060, Australia) (12%) (Figure 8). Seventy-five per cent recorded that more than one session of grafting was required to achieve the desired result (Figure 9). The need for multiple sessions may reflect variable graft survival,4–6 or intentional serial, smaller volume injection to optimise survival.7 The variability in number of graft sessions required may alternatively reflect that varying numbers of sessions are used for different indications. Eighty per cent of respondents did not use any post-grafting volumetric analysis (Figure 10). Methods that have been trialled include Vectra 3D imaging (Canfiled Scientific, Parsippany, New Jersey, 07054, USA) MRI, ultrasound, CUI (Mentor, Irvine, California, USA) breast measurement device and standardised photography.



Discussion
Our results, which were compiled from a combination of a single question incorporated into the ABDR and a more comprehensive set of questions that comprised the first dedicated survey of fat grafting in Australian plastic surgery, demonstrated that the use of fat grafting is rapidly increasing in Australia. Nevertheless, clinical practice of fat grafting remains poorly standardised with respect to donor site selection, harvest technique, processing technique, number of sessions required and volumetric follow-up.
Heterogeneity in fat graft practice is consistent with findings from previous literature reviews we and others have completed.2,3 There is a lack of consensus regarding the most effective technique. This variability in technique likely contributes to the variable graft survival rates reported in the literature as 40–70 per cent.4–7 The nature of fat grafting consisting of multiple steps from fat harvest to fat injection likely further contributes to this variable graft survival.
To our knowledge, there are no retrospective or prospective human studies comparing fat graft survival with use of different tumescent fluid components, different donor sites or different harvest techniques. In terms of fat graft processing, a retrospective review of a single surgeon’s experience of AFG with implant-based breast reconstruction in over 1000 patients comparing decantation to a proprietary closed wash and filtration method found a significantly higher rate of fat necrosis in the decantation group versus the Puregraft group (3.2% versus 1.0%, p = 0.01).8
The number of adipose derived stem cells (ASCs) in the graft also appears to contribute to fat graft survival. In 2013, Kolle and colleagues conducted a non-randomised placebo-controlled trial to investigate the effects of adding autologous, cultured ASCs to grafted fat and found a 65 per cent increase in volume retention by MRI volumetric assessment (p < 0.0001).9 The same group trialled this technique for large-volume lipo transfer in primary cosmetic breast augmentation and measured an 80.2 per cent mean retention rate in the ASC-enriched group compared to 45.1 per cent in the control group (p = 0.0022).10 Graft supplementation with platelet-rich plasma has shown a 30 per cent improvement in volumetric retention as measured by Gentile and colleagues, who performed team-based clinical evaluations of breast contour post-lipotransfer.11
The current process of gaining consent from patients for fat grafting is based on lower quality evidence from clinical case series, single-surgeon experiences and literature that reports highly variable outcomes based on the multitude of techniques used in the fat grafting process and for various indications. Altogether this suggests that more robust data from comparative clinical trials informing fat graft success rates and long-term retention would improve consent for patients undergoing autologous fat grafting as a primary reconstruction, augmentation or adjunct to other reconstructive options. Objective volumetric assessment devices, such as a protocolised ultrasound assessment, MRI or Vectra 3D imaging, will facilitate strong objective outcome measures of graft survival in future clinical trials.
Limitations
Our study had several limitations. The significant rise in recorded use of fat grafting since 2012 may reflect in part the increase in number of sites participating in the registry and increasing capture rates over time. Missing data is also a consideration, as fat grafting is reported through a tick box option. No tick is assumed to mean no fat grafting but may also reflect missing data, which would result in an underestimation of the prevalence of fat grafting use. The survey data was also limited by its 21 per cent response rate and subsequent 10 per cent margin of error. Victorian plastic surgeons represented 54 per cent of the survey data which was disproportionate to their 30 per cent representation of ASPS members. The survey results may therefore over-represent Victorian fat grafting practice. Finally, plastic surgeons are not the only surgeon group who perform fat grafting in Australia. General surgeons who perform fat grafting in breast surgery were not represented.
Notwithstanding this, the increasing use of this technique means that clinical data measuring the effect of patient demographics and procedural variables on fat grafting outcomes is vital to ensure patient safety, health resource management and to inform best practice guidelines. The information gathered by analysis of the heterogeneity in technique leading to specific outcomes will form a powerful foundation on which to base future regulatory decisions related to fat grafting and fat therapeutics.12 Further, basic laboratory research is underway to characterise the cellular heterogeneity within adipose tissue and between its depots, and may scientifically assist the decision-making processes to which clinicians and patients have access.13
As gene profiles and functional phenotypes of these heterogeneous cell populations are identified through our ongoing work, fat grafting and fat therapeutics may be further optimised. In addition to further basic science research, a registry database would provide the clinical data required to optimise and monitor this technique. A general registry of autologous fat transfer exists in the United States for American, Brazilian and Canadian plastic surgeons. As a historically significant contributor to clinical innovation and research in plastic surgery, it is important to characterise practice in our jurisdiction in order to ensure that both best practice is maintained and Australian plastic surgeons and researchers may optimally contribute to fat grafting practice globally.
Acknowledgements
We thank the Australian Breast Device Registry for providing the registry data included in this manuscript. We thank the Australian plastic and reconstructive surgeons who completed the fat grafting survey.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship and/or publication of this article.
Revised: July 20, 2022 AEST