Introduction
Breast augmentation is one of the most frequently performed surgeries by specialist plastic surgeons in Australia.1 Refinements in operative breast augmentation techniques have continued to evolve over time. Implant migration remains a concern, especially when using smooth implants. The breast implant can either displace laterally towards the mid-axillary line or inferiorly through the inframammary fold, resulting in a loss of cleavage, upper pole fullness, ‘bottoming out’ and in some cases, a ‘mega pocket’. Specifically, this technique aims to prevent telemastia, defined as an abnormally wide separation between the breasts.2
We propose an intraoperative technique unique to primary breast augmentation that ensures the breast implant is secured by means of a composite autologous myofascial (CMF) sling involving the pectoralis major muscle. This aims to prevent inferno-lateral displacement of the breast implant which renders a poor aesthetic result secondary to loss of ‘cleavage’ and the resultant formation of a mega pocket. The authors have integrated this technique into their practice since August 2020, with case numbers now in excess of 500. The authors use the technique to mitigate implant displacement in both breast augmentation and augmentation mastopexy cases.
Operative technique
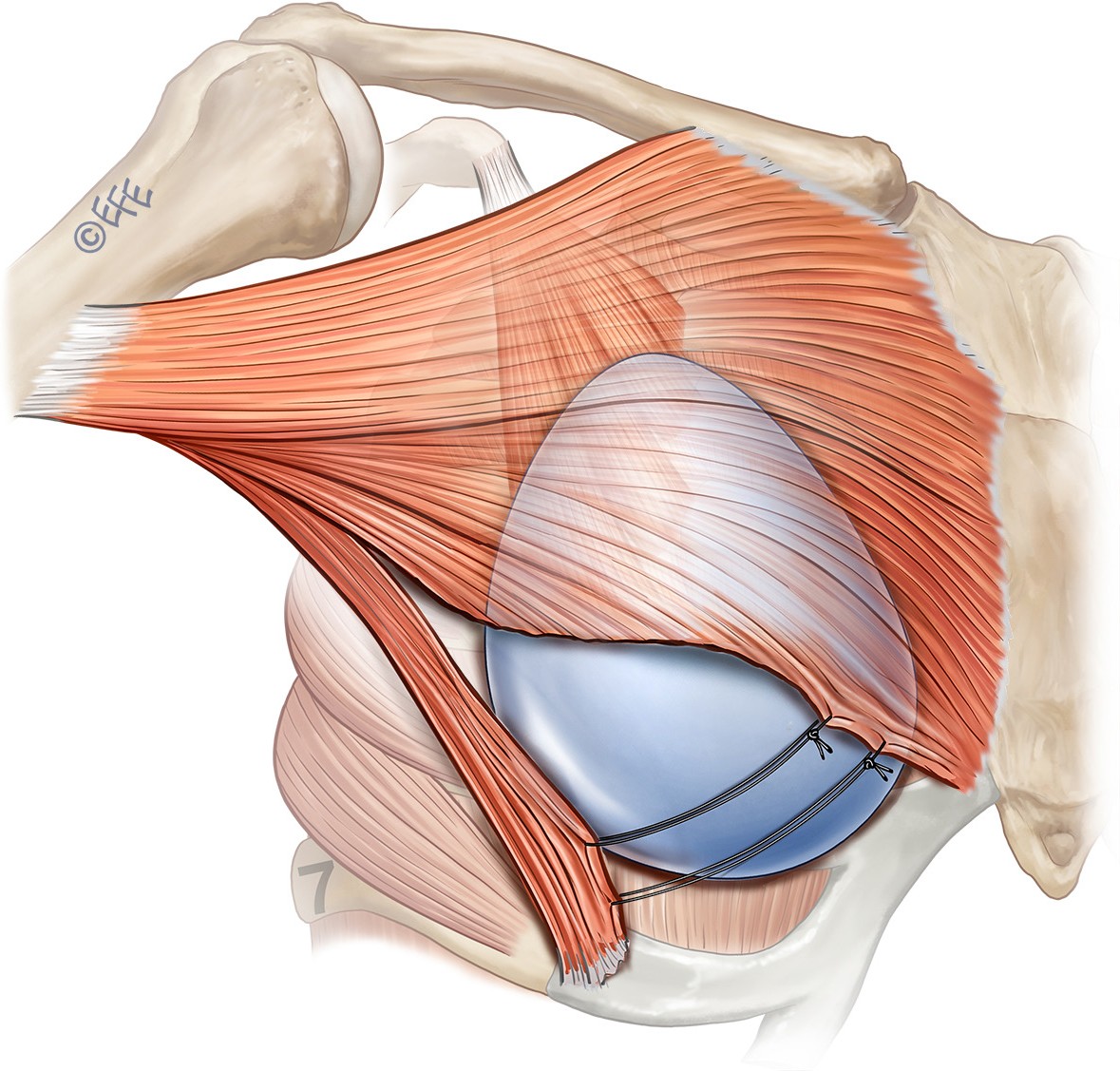
An inframammary incision facilitates dissection through the superficial fascial system (SFS), down to the pectoralis major fascia at the 6 o’clock position, to expose the inferolateral pectoralis major fibres. A submuscular pocket is elevated in the loose areolar plane between pectoralis major and minor to facilitate dual plane coverage of the impending breast implant. The most inferolateral muscular fibres (approximately 1.5–2 cm in transverse diameter) of pectoralis major are dissected and elevated as a myofascial flap. This may also incorporate the uppermost fibres of serratus anterior, particularly in cases where the pectoralis major is deficient caudally. A myofascial sling is then constructed with either a transverse cable tie or horizontal mattress suture, using a tapered 2/0 polydioxanone (PDS) suture, which is inserted through the myofascial substance of the pectoralis/serratus flap. The breast implant is inserted aseptically into the submuscular plane (Figure 1). The myofascial sling is then secured and tied medially onto the perichondrium of the rib at the inframammary fold (IMF), or the costochondral border of the sixth costal cartilage, or to the caudal edge of the sternal origin of the pectoralis major muscle serving as a biomechanical hammock to suspend the implant, thus preventing inferno-lateral displacement of the implant, and the resultant telemastia. If the vector of the CMF sling is unfavourable for cable sutures medially, then we create a sling by suturing vertically to the undersurface of the breast parenchyma. It is the preference of the senior author to avoid securing the cable ties to the cephalic aspect of the medial pectoralis major fibres, given the potential animation deformity that may result.

Conclusion
Advocacy of submuscular breast implant and expander placement has been extensively described, primarily with regard to preventing exposure of these devices in the context of adjuvant radiotherapy for breast cancer.3,4 In contrast, our technique exclusively applies to both primary breast augmentation and augmentation mastopexy cases. This functionally serves to prevent implant lower pole (ILP) migration inferolaterally in order to improve long-term aesthetic outcomes. There is potential to reinforce such inferolateral implant support by means of a synthetic mesh overlaying the cable ties, although this would also increase the theoretical risk of infection. Our proposed method remains as first described pertaining to primary breast augmentation and augmentation mastopexy by virtue of a cable-tied myofascial sling in a total of over 500 cases performed by the senior authors. Long-term follow up of our case series has the potential to define potentially superior aesthetic outcomes consequent to incorporating this technique. This technique is particularly suitable for those patients whose chest wall anatomy predisposes them to implant migration and telemastia. However, the authors advocate for its use in all cases to achieve superior long-lasting aesthetic outcomes, in particular the longevity of upper pole fullness and medial cleavage lines. The incidence of revision surgery for implant migration has reduced dramatically since incorporating this technique.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship and/or publication of this article.
SUPPLEMENTARY ONLINE MATERIAL
Videos accompanying this guide can be found on the AJOPS YouTube channel:
https://youtube.com/shorts/I-E8yR-IHV8
https://youtube.com/shorts/ROs01l-A3aw
https://youtube.com/shorts/hHYN5AbDvuw