
Introduction
An escharotomy is a time-critical/emergency limb or even life-saving procedure following a severe large burn. Deep or full thickness circumferential burns require prompt escharotomy. If left untreated these burns can lead to ischaemic tissue damage and eventually irreversible necrosis in the extremities, or respiratory depression, in the context of fluid resuscitation for a severe large burn. Due to the rapid progression of compromise, an escharotomy may need to be performed by health professionals with little or no previous experience when patients are being treated outside of a burn centre, and where immediate transfer is not possible. Even within a burn centre, this procedure may have to be performed by health professionals who have not performed it for months/years. Both situations occurred throughout New Zealand in December 2019 following the White Island (Whakaari) volcanic eruption. While online resources are included as part of the National Burn Service website, on review, the illustrations detailing incision placement were found to lack clarity (Figure 1). Performing accurate escharotomy incisions allows for maximal benefit with minimal scarring as well as protecting vital structures such as nerves and blood vessels.

The original description of escharotomy was provided in 1607 by Fabry of Hilden.1 The modern model of escharotomy incision placements was championed much later by Pruitt in 1968, and has remained relatively unchanged.2 Throughout the years, different authors have adjusted and modified the placement of incisions; however, these resources still lack clarity or detailed illustrations of accurate and safe incision placement.3–5 In addition, there is controversy around hand/digital escharotomy; although previous publications have favoured the use of digital escharotomies, demonstrating higher rates of finger salvage when compared to control.6,7 The evolution of management of severe burns has developed a new concept for escharotomy, which places it within a wider group of decompressive therapies, including fasciotomy, nerve releases, orbital decompression and laparotomies.4 There is an important emphasis on the ‘process’ of burn escharotomy involving a continuum of assessment and reassessment of distal circulation or respiration following the completion of the procedure.3,4 Nonetheless, when faced with a burn patient requiring escharotomy, there may be a considerable level of resources and support required by the health practitioner, especially when they are out of practice or it is being performed in a remote location.
Driven by the national events that unfolded following the Whakaari volcanic eruption, we aimed to update the national escharotomy guidelines, providing clear and user-friendly illustrations. These new guidelines were then put through local evaluation to establish the effectiveness of the newly developed resource materials.
Methods
Updating escharotomy guidelines
We began by assessing the available English literature for recommended escharotomy incision placement. This information, alongside expert opinion from the Australian and New Zealand Burn Association (ANZBA), was used to guide decision making on the appropriate placement of escharotomy incisions for our new guidelines. A medical illustrator was consulted and volunteered to produce new illustrations depicting escharotomy incisions, with emphasis on detailing the precise incision placement on different body parts.
Surveys
We completed two surveys involving the plastic surgery registrar cohort at Middlemore Hospital, across two six-month registrar terms. The first survey aimed to establish baseline knowledge within a cohort of doctors who would be expected to perform such a procedure. This required the participants to draw escharotomy incisions without consulting any guidelines. A second survey aimed to evaluate the usefulness of the new guidelines with participant feedback. In the second survey, the participants were asked to draw escharotomy incisions on blank human illustrations with the use of the new guidelines.
Demographic information sought from the participating registrars included postgraduate level, training status SET vs non-SET (SET: surgical education and training) and completion of the Emergency Management of Severe Burns (EMSB) course. Data were analysed using Microsoft Excel™ (Microsoft Excel 2016, Microsoft, North Sydney, New South Wales, 2060, Australia) and GraphPad (Version 7.05, Prism Software, Irvine, California, USA) to determine statistical significance (t-test). Ethical approval was sought and granted through the Auckland Health Research Ethics Committee [AHREC Ref: AH22018]. Surgical education training plastic surgery registrars are doctors who have been selected for training to become vocationally-registered plastic surgeons by the Royal Australasian College of Surgeons (RACS). Non-SET plastic surgery registrars are not in the training program.
Results
Eighteen plastic surgery registrars were surveyed with a median of seven years of postgraduate training. Of these, forty-five per cent were SET trainees. Following the first survey, without consulting any guidelines, 72 per cent, 54 per cent and 82 per cent of participants correctly demonstrated placement of upper limb, anterior torso and lower limb incisions respectively. The follow-up survey had a response rate of 94 per cent. This second survey showed that 85 per cent of participants correctly demonstrated the placement of upper limb incisions. One hundred per cent and 90 per cent of participants accurately demonstrated placement of anterior torso/neck and lower limb incisions respectively (Table 1).
There was an observable improvement in overall incision placement accuracy, and this was greater in the non-SET vs SET registrar subgroup: 54 per cent vs 32 per cent (p = 0.206) respectively. General participant feedback on the new guidelines was positive; on average the indication of usefulness for the guidelines from ‘not useful’ (1) to ‘very useful’ (10) was 9/10. All participants felt they could safely perform an emergency escharotomy using these guidelines. The most difficult area for incision placement was reported by participants to be the hands, fingers and thumbs (descending order).
Discussion
Good outcomes following a burn injury depend greatly on the initial resuscitative care provided to patients, and this includes escharotomies performed promptly.6 Performing an escharotomy can be a daunting task in the hands of a practitioner who is inexperienced or who has had little practice. Therefore, to ensure the best possible timely outcomes we must provide accessible and user-friendly resources. We have met our aim to improve the current standard of escharotomy resources, which have been locally evaluated to determine if they are fit for purpose.
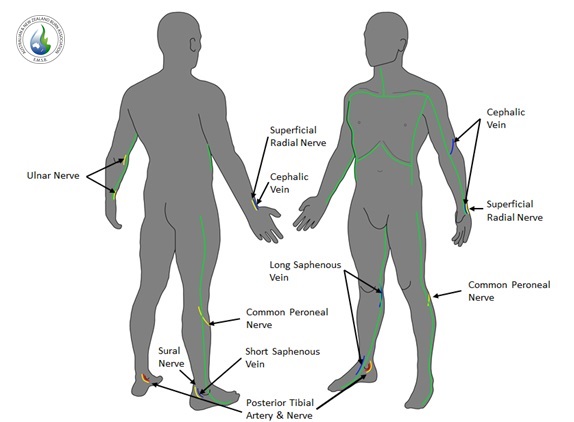
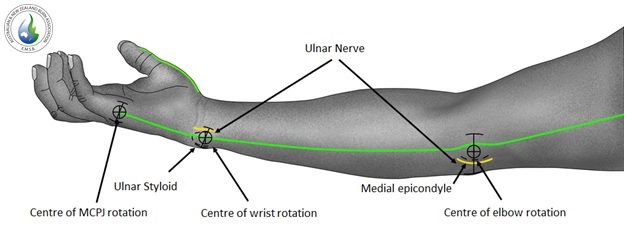
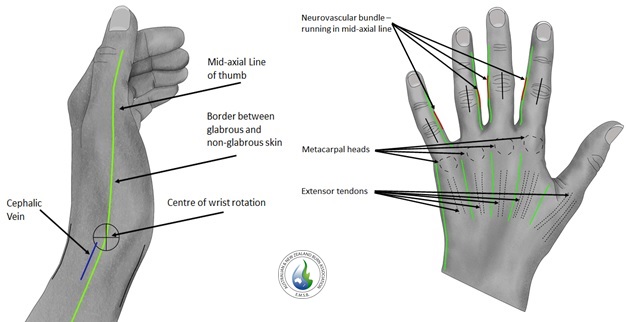
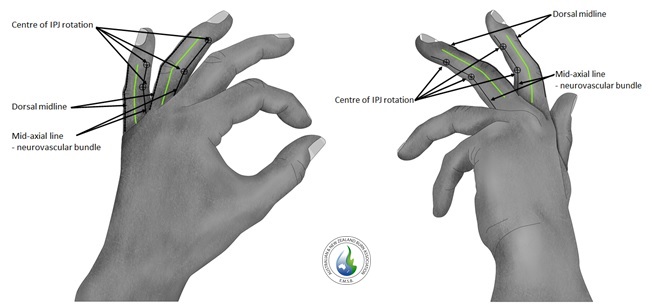
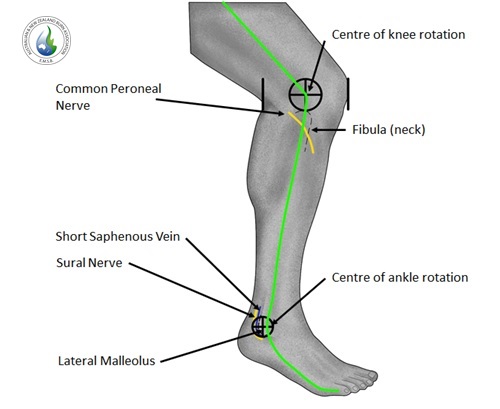
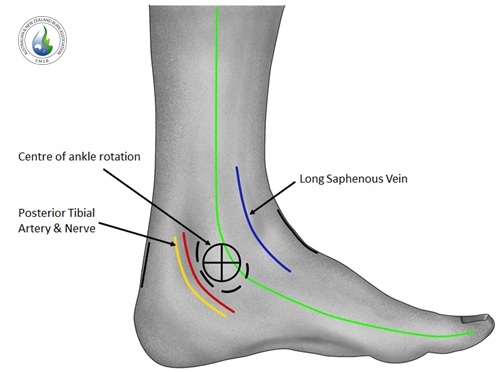
The consensus on exact incision placement has varied over time and throughout the literature, especially with certain body areas such as the neck and hand/digits. To distil the incision placements within our new illustrations (Figures 2–7), we undertook a literature review and consultation with Australasian burn surgeons, alongside the EMSB education committee. Areas of interest included the hand, digits and neck. In our illustration (Figure 2), the placement of a midline incision of the neck during escharotomy aims to protect the vital lateral neurovascular structures from injury or desiccation. In addition, a central location may also facilitate future tracheostomy placement if prolonged intubation is warranted in the intensive care setting. Moreover, the dorsal hand incisions have been placed in line with each of the web spaces, thus protecting extensor tendons from exposure or desiccation. The location of the dorsal hand escharotomy incisions still provides access for fasciotomies through the same wound. Digital escharotomies should be considered on a case-by-case basis, performed through a single incision in the mid-axial line. Care must be exercised not to injure the nearby neurovascular bundle. In our illustration, each finger receives a single incision on the non-working border (Figure 5).
._illustration_by_dr_cath_francis.jpg)
._illustration_by_dr_cath_francis.jpg)
._illustration_by_dr_cath_francis.jpg)
._illustration_by_dr_cath_francis.jpg)
._illustration_by_dr_cath_francis.jpg)
._illustration_by_dr_cath_francis.jpg)
Plastic surgery registrars were chosen because of their pre-existing knowledge and expected familiarity with escharotomies. These registrars are typically the first point of contact for advice from other services outside of the burn centres regarding burn management, including escharotomies. They would also be expected to perform the emergency procedure ‘after hours’ as they are onsite 24/7. The registrars are expected to know the correct placement of escharotomies as part of their role. Nevertheless, this survey evaluation has demonstrated that these new guidelines improved participant performance with regards to correct incision placement, with the most impact on junior doctors (non-SET compared to SET registrars). Although this result did not reach statistical significance due to the underpowered nature of the study (and the baseline level of expertise expected), it nevertheless highlights the benefit of these resources, particularly for the less experienced.
Participant feedback has indicated ongoing areas of difficulty to be the hands, fingers and thumbs. These areas historically lacked consensus within the literature and highlight the need for ongoing work to improve instructions for escharotomy incisions in these areas. Our emphasis with these illustrations has been to use anatomical landmarks, such as the joint axis of rotation, to guide the users in incision placement (Figures 3–7). The guidelines helped improve performance specifically in junior doctors, demonstrating the applicability of these resources to those less familiar with the procedure. Although feedback received on the new guideline illustrations was positive overall, there were requests for video demonstrations to further clarify the procedure; this is an area of future development.
Conclusion
Our updated National Burn Service escharotomy resources have been locally evaluated and determined to be easy to use. By incorporating detailed illustrations, we provide highly accurate escharotomy incision placement guidelines. Difficult areas of the body will require attention in future revisions of this resource. These updated illustrations are an important step in allowing an escharotomy to be safely performed by those who need to perform it but are unfamiliar with the procedure.
Acknowledgement
Images reproduced with permission from Australian and New Zealand Burn Association are taken from the manual, Emergency Management of Severe Burns, 19th ed. Queensland, Australia: ANZBA, 2021.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship and/or publication of this article.
Revised: July 23, 2022 AEST