
Introduction
Breast augmentation is the most common elective cosmetic surgical procedure, with around 10,000 women undergoing this procedure in Australia each year.1 Complications such as infection and capsular contracture are the most common reasons for revision surgery.1,2 These complications vary depending on many factors with choice of surgical approach being an important one.2–4
We present a case of a breastfeeding mother who developed sudden onset unilateral peri-implant collection containing 800 mL of breast milk, three years following bilateral breast augmentation via a periareolar approach. Written consent was provided for publication of patient data, including deidentified photographs.
Case
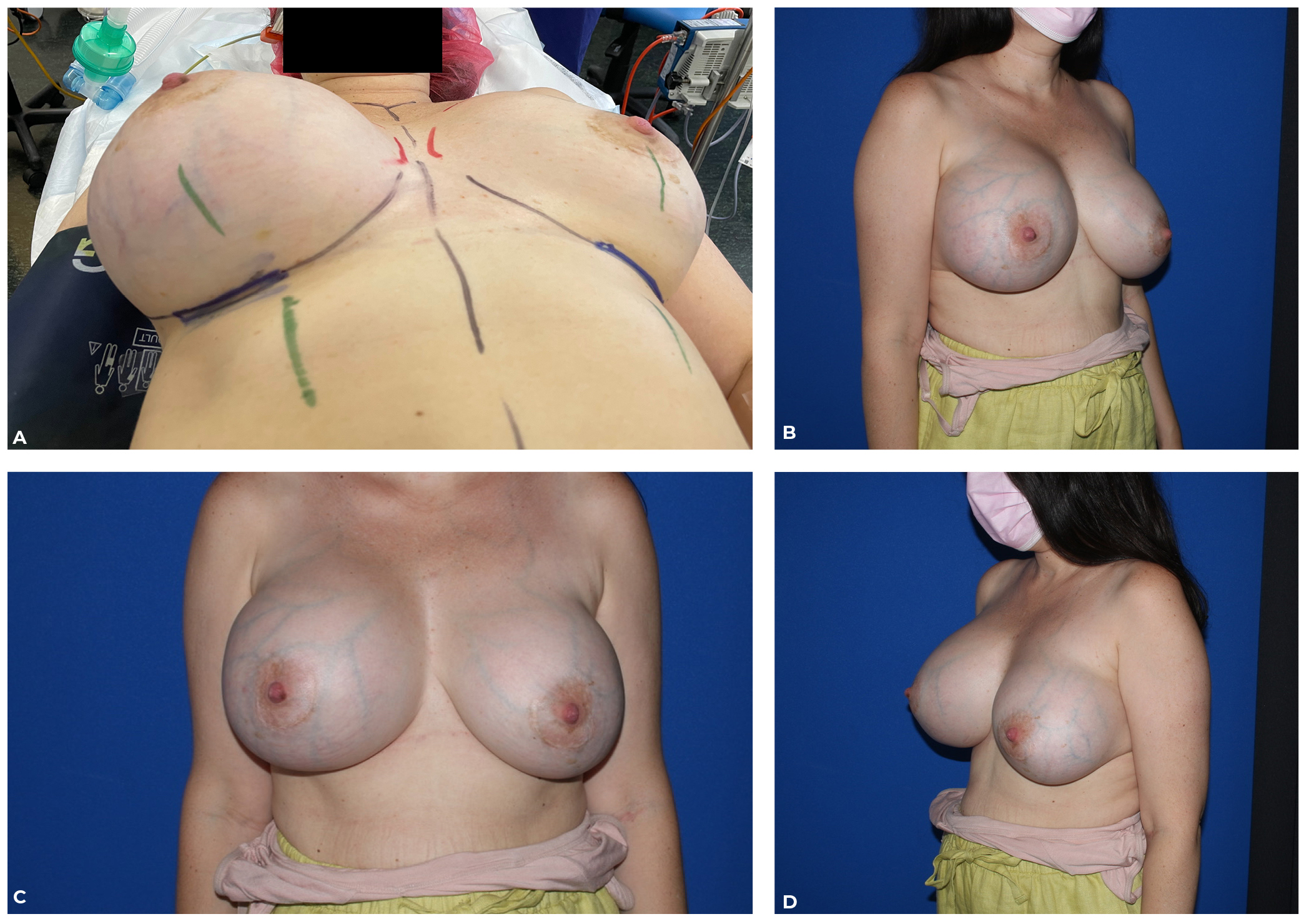
A 34-year-old female underwent bilateral cosmetic breast augmentation three years prior via an inferior periareolar approach. Six months postoperatively she experienced gradual implant descent/malpositioning on the left side. She subsequently gave birth to her first child (five months old at time of re-presentation), had been exclusively breastfeeding and described plentiful breast milk supply. Over a two-week period, she developed a large unilateral breast swelling which became tense and painful (Figure 1). Ultrasound-guided aspiration was arranged and demonstrated peri-implant collection of ‘milky fluid’ with negative microscopy, culture, cytology and flow cytometry to exclude anaplastic large cell lymphoma. Ultrasound examination reported a complex collection of peri-implant fluid and intracapsular rupture and recommended MRI. MRI reported an extensive peri-implant fluid collection on the right and intact implants bilaterally.
_preoperative_right_breast_swelling_(b__c___d)_previous_periareolar_incisions.jpg)
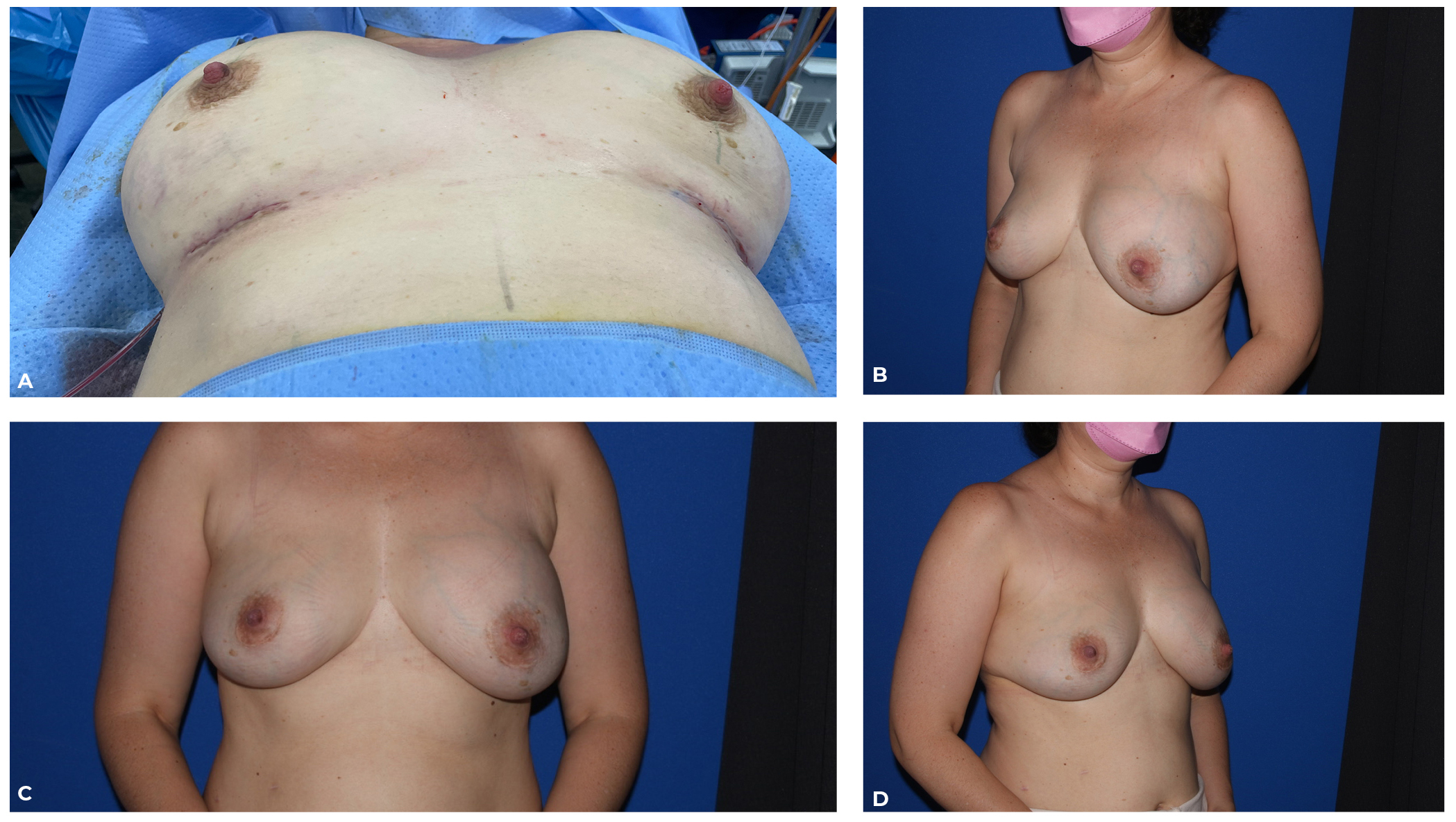
The patient consented to a bilateral explantation and capsulectomy as she did not want to keep either implant in-situ. Upon entry through the capsule, it was evident that the seroma was composed of breast milk as there was copious milk solids within a collection of milky fluid (Figure 2). The breast milk and solids were drained to completion, the breast milk solids were debridedfrom the capsule, explantation was completed and the cavity meticulously washed. A palpably thin segment of the otherwise well-established capsule, bordering the deep breast tissue (underlying the periareolar incision), was deemed to be a potential site of fistula between the capsule and breast parenchyma, so was plicated with 4-0 braided absorbable suture (Vicryl, Ethicon, New Jersey, USA) (Figure 2). Bilateral 280 mL microtextured, round Eurosilicone (GC Aesthetics France SAS, Dublin, Ireland) were removed and were intact bilaterally, with minimal gel bleed on the left (Figure 3). Given there was no absolute indication for capsulectomies, and to reduce the persistence of a breast parenchymal fistula from further disruption of the breast parenchyma (particularly in the currently breastfeeding mother), capsulectomy was not performed. If implants were to be replaced in future, we would then ensure the patient had completed their family and ceased breastfeeding, and we would discuss the risks and benefits of capsulectomy at time of implant insertion.
_evacuation_of_breast_milk_intracapsular_collection_(b)_samples_sent_for_analysis__and_(c).jpg)
Following surgery, the patient’s symptoms resolved; there was 80 mL of haemoserous drainage to four days postoperatively and no milk was found in the drain output. She was encouraged to express for comfort from the affected right breast but was able to continue breastfeeding her child. At two weeks and four weeks postoperatively, she developed mild mastitis on the affected side, which was successfully treated with oral antibiotics and mechanical methods.
Biochemical analysis of the intracapsular fluid demonstrated 2.2mmol/L glucose, 43 g/L total protein, 29 g/L albumin, 2149 U/L lactate dehydrogenase, 1.4mmol/L trigylcerides and 1.4mmol/L cholesterol. Lactose and lactoferrin testing were unavailable.
Bacterial culture, acid-fast bacteria culture, fungal culture, cytology, flow cytometry and histopathology of the intracapsular fluid and milk solids were negative. Although culture was negative, it does not mean the collection was entirely sterile, given the known colonisation of breast milk with normal flora.

Discussion
Following an extensive literature review (PubMed from inception to June 2022, including the terms ‘breast implant’, ‘seroma’, ‘breast milk’, ‘collection’ and ‘lactocoele’), and to the best of our knowledge, breast milk intracapsular collection has not been previously described as a complication of breast augmentation. This rare case represents a previously unreported, but evidently important, complication of breast augmentation. An intracapsular collection of breast milk is distinct from a lactocoele, which can occur after any breast surgery as an immediate or short-term complication and may be in continuity with a newly placed implant. A simple lactocoele located within glandular tissue could be drained (via image-guided or open surgical techniques) without entering the peri-implant spaceas opposed to an intracapsular collection, and thus management is different. Although clinically distinct, they are likely driven by shared mechanisms.
The mechanism of postoperative lactocoele or even galactorhoea (abnormal expression of breast milk) is thought to be increased prolactin levels due to stimulation of intercostal nerve branches during surgery.5 Lactocoeles can also be spontaneous in pregnancy, in breastfeeding mothers or those taking contraceptives, with a proposed mechanism of ductal obstruction driven by increased prolactin.6 In this case, ductal obstruction via surgical disruption of the periareolar breast parenchyma, exacerbated by active lactation, is thought in this case to have forced breast milk into the established implant capsule. Disruption of the breast parenchyma similarly continues from the nipple, along the path of insertion and onto the peri-implant space. A thin anterior capsule may have represented a potential fistula tract, corresponding with the path of implant insertion three years prior. An inframammary approach avoids disruption of the parenchyma and thus likely reduces the potential for fistula formation.
Various surgical approaches are available for breast augmentation, including inframammary, periareolar and transaxillary, with each offering a unique risk and benefit profile.2,4 Inframammary incisions have historically been and remain the most common choice given consistent anatomy and easy dissection to the surgical plane, which then provides adequate exposure of the pocket. This contrasts concerns regarding higher rates of capsular contracture, decreased nipple sensation, wound infection and reoperation rates with periareolar and transaxillary approaches.3,4 Certainly, an augmentation mastopexy involves implant insertion and simultaneous manipulation of breast tissue and would carry similar risks for lactocoele and breast milk intracapsular collection.
Multiple studies have demonstrated the rates of capsular contracture to be significantly lower with inframammary incisions compared to periareolar incisions.4 There is a strong evidence base to support a bacterial biofilm seeded at time of implantation as the primary causative factor in capsular contracture.7,8 The 14-point plan is a group of perioperative strategies aimed at reducing device infection and capsular contracture.7 Point II suggests the avoidance of the periareolar approach as the dissection passes through breast tissue. Similarly, point III suggests the use of nipple shields as the endogenous breast flora is known to inhabit both the breast tissue and nipple areolar complex during surgery.9
Early research reported high rates of altered nipple sensation with a periareolar approach10; however, this has not been studied with prospective randomised trials. The rates of implant malpositioning and reoperations are higher in periareolar incisions.4
This case report and literature review are a timely reminder for all surgeons who perform breast augmentation to consider the risks imparted by their operative decisions. Surgeons must ensure their patients are informed of the risk profile unique to the operative approach offered to them, especially if this differs from the most common inframammary approach. This is particularly true in women who are yet to complete their families.
Conclusion
Breast milk intracapsular collection is a rare but potential complication of breast augmentation. Traversing the breast parenchyma when placing implants through a periareolar incision may lead to a potential fistula tract. Augmentation mastopexy may theoretically carry this same risk. Surgeons should be aware of this potential complication in women who are yet to complete their family.
Patient consent
Written consent was provided for publication of patient data including deidentified photographs.
Conflict of interest
Dr Deva is a research coordinator for Johnson & Johnson (New Brunswick, NJ), Allergan (Irvine, CA) and KCI (3M) (St Paul, MN). The other authors have no conflict of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship and publication of this article.
Revised: 2022 August 17 AEST