Introduction
Carpal tunnel syndrome (CTS) is the most common entrapment neuropathy.1 Although CTS is often idiopathic, a variety of aetiologies have been described that are responsible for median nerve compression within the carpal tunnel, the most common being tenosynovitis of the flexor tendons.2 High division of the median nerve, known as bifid median nerve (BMN), has a incidence of two per cent to 26 per cent and can be associated with CTS.3–6 BMN is often found with persistent median artery (PMA) thrombosis.4,7,8 Persistent median artery has a weakly reported prevalence of between 0.6 per cent to 30 per cent and is also known to be a rare but independent cause for median nerve compression at the wrist.9–13 Discussions on the diagnosis and management of BMN and PMA thrombosis associated CTS are limited in the literature. This review presents two cases of CTS with associated PMA thrombosis and BMN and offers a discussion on diagnostic and management options.
Cases
Case 1
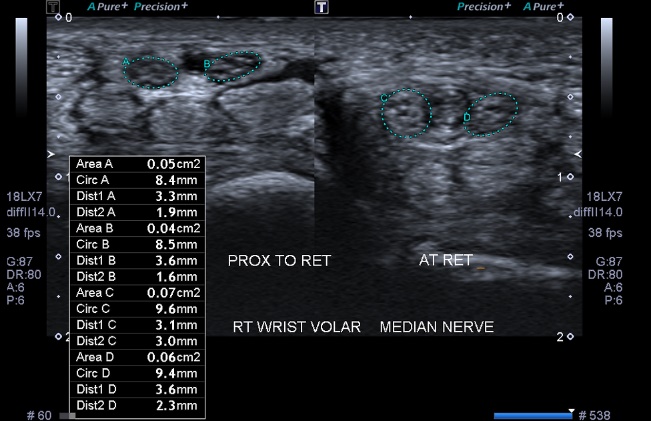
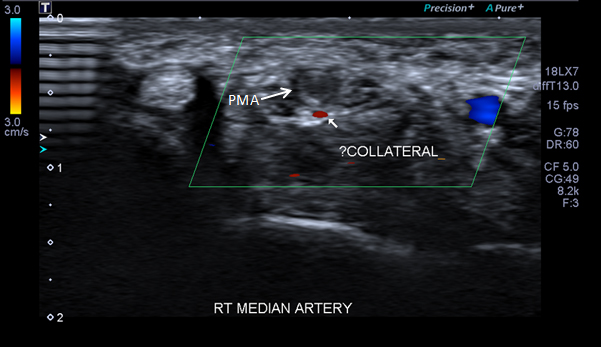
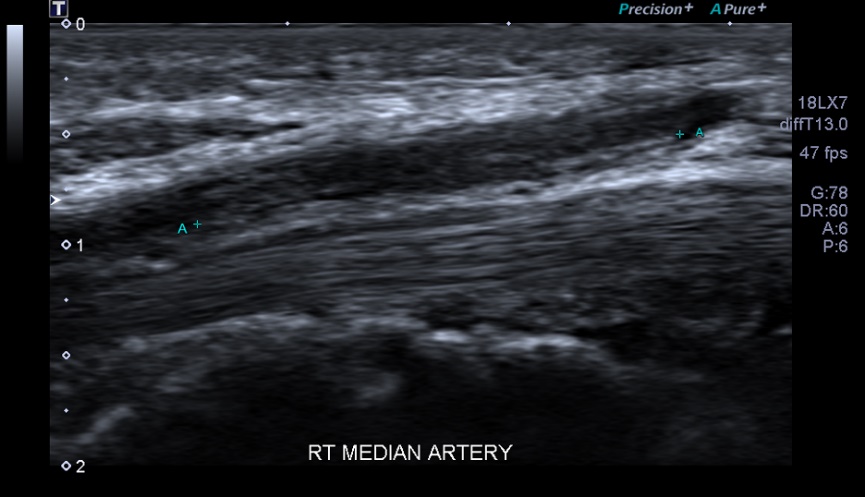
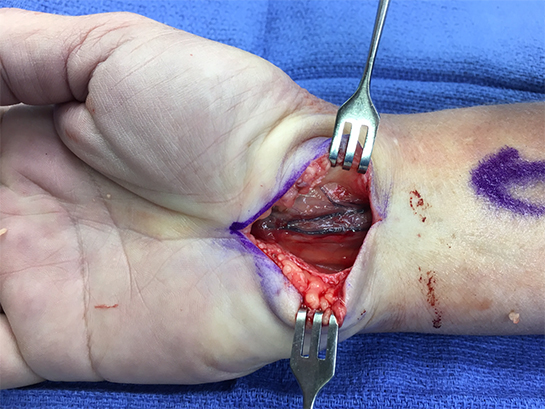
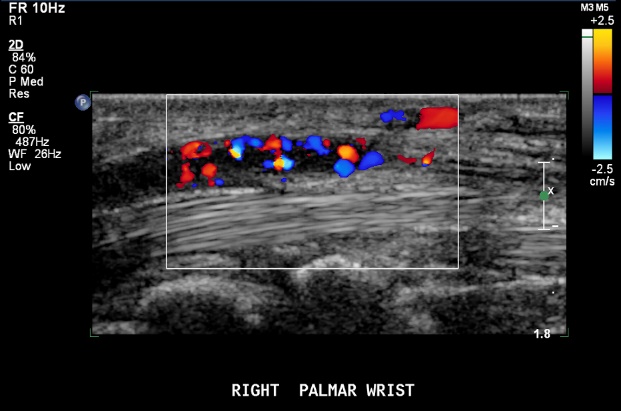
A 29-year-old female with a past medical history of rheumatic heart disease presented with shooting pains in her right wrist and hand. Two weeks prior she had sustained a crush injury to her right wrist. Prior to her injury she had no symptoms in her wrist or hand. On examination she had reduced sensation in the median nerve distribution and had positive Phalen’s and Tinel’s tests. High resolution ultrasonography and Doppler demonstrated a BMN with PMA thrombosis (Figure 1). A segment of thrombus extending over a distance of 22 mm was noted at the wrist involving the PMA. The thrombosed segment was noted to be causing a mild mass effect on the adjacent bifid nerve bundles without change in nerve calibre. The distal artery demonstrated reconstituted flow. After discussion of treatment options, the patient underwent an open carpal tunnel release. The thrombosed, enlarged median artery was identified intraoperatively adjacent to, and overlying, the median nerve, causing compression within the carpal tunnel. The flexor retinaculum was released and the thrombosed segment of the artery was left intact (Figure 2). The patient was reviewed in the outpatient hand clinic one week later and reported relief of her symptoms. At follow-up 12 weeks post-surgery she reported having pillar pain and weakness when using her hand. Her pain and dysaesthesia was relieved through anti-inflammatories. The patient received no anticoagulation throughout their treatment.


Case 2
A 59-year-old female presented with a six-week history of progressively worsening pain and paraesthesia over the radial aspect of her right hand. She had sustained no injuries prior to the onset of her symptoms. Her past medical history comprised of idiopathic cardiomyopathy, hypertension, hyperlipidemia and heavy smoking. High-resolution Doppler ultrasound demonstrated a BMN and partly thrombosed persistent median artery at the level of the lunate that had concentric thickening involving all three layers of the arterial wall. There was a hypoechoic thrombus with some Doppler flow around the periphery which could reflect early recanalisation (Figure 3). A BMN and PMA was also visualised in the left wrist without thrombosis. The patient underwent an open carpal tunnel release. The thrombosed PMA and BMN were left intact (Figures 4 and 5). The patient was reviewed two weeks postoperatively and had almost complete resolution of her original symptoms, however, she had developed shooting pain in her little finger. She underwent nerve conduction studies, which were unremarkable. Her pain resolved with no additional treatment or anti-inflammatories at subsequent outpatient reviews.



Discussion
Embryology
The median artery is usually a transitory vessel that develops from the brachial axial artery in early embryonic life.14 It accompanies the median nerve in the forearm and during embryonic development acts as an important vessel of the forearm and hand.14–16 After the eighth week of gestation, the median artery usually regresses and the ulnar and radial arteries then dominate arterial supply of the hand.14 The vestigial median artery remains as the arteria comitans nervi median which accompanies the median nerve in to the forearm.17 It becomes perceived as a ‘persistent median artery’ when it is of a diameter and presence large enough to be noticed either through ultrasound or visual inspection.18 Persistent median artery has been described in two different patterns based on the vascular territory: palmar and antebrachial.19 In the palmar type, the PMA reaches the hand while in the antebrachial type, it terminates before reaching the wrist.19 When extending into the carpal tunnel, PMA may join the superficial volar arch, may supply the radial digits with an absent arch, or may end as a thrombosed vessel.20 In the majority of studies, PMA has been observed to be unilateral and assuming a position ulnar to the median nerve in the distal forearm.20
The median nerve is the only nerve to travel through the carpal tunnel. Anatomical variations of the median nerve are common and well-described in the literature.21 In 1977, Lanz classified median nerve anatomic variations into four groups, group III being the bifid or high division median nerve.8 The two parts of the nerve may be equal in size or a predominance may exist of either the radial or ulnar part.22 This may be clinically relevant in cases in which there is a pathology of the median vessels because the bifid nerve anomaly may be missed if the small ulnar division is surrounded by the abnormal median vessels.7 The most common variants of BMN are accompanied by persistent median vessels with or without involved pathology.7
Persistent median artery, bifid median nerve and carpal tunnel syndrome
Over the last two decades there have been a limited number of recorded clinical reports that describe the aetiopathogenesis, diagnosis and management of CTS secondary to PMA and BMN.1,9,23–25 Persistent median artery is usually asymptomatic, however, it may be responsible for median nerve compression secondary to thrombosis, calcification or an aneurysm of the artery.20,23,26–29 Thrombosis is the most frequently reported cause. Persistent median artery thrombosis may be caused by infection of deep fascial planes, trauma, frequent bicycle riding with the wrist placed in an unusual position, hormonal contraceptive pills and repetitive wrist work such as frequent screwdriver usage.9,26,30–33 The mechanism by which PMA thrombosis produces CTS has been proposed to be either directly through nerve compression or by an ischaemic phenomenon from a poor anastomotic connection between the median, ulnar and radial arteries.23,30,34 Consistent with the cases in this study, PMA thrombosis symptoms usually include acute or sub-acute pain and parathesiae in the median nerve territory of the hand.30
There is no consensus in the literature regarding BMN as an independent risk factor for CTS. In 2008, Bayrak and colleagues proposed that BMN may predispose to median nerve compression and CTS because of a higher cross-sectional area relative to that of a non-bifid median nerve. However, a higher BMN cross-sectional area was only found in the control group and not in the patient group.3 The study did find a significant difference in the relative frequency of BMN in CTS patients versus the control population.3 This is in contrast to the 2011 study by Granata and colleagues who demonstrated, using ultrasonography, that the prevalence of BMN had a similar frequency in the patient group affected by CTS and in symptom free control group.21
Median nerve conduction studies are often considered the gold standard investigation in CTS diagnosis.35 Imaging studies such as ultrasonography and MRI are promoted with the claim they may reveal anatomical variants such as PMA and BMN that are responsible for some atypical CTS presentations. Studies using ultrasonography and MRI imaging for assessing PMA and BMN prevalence and incidence have demonstrated that each modality can delineate these anatomical variants.3,20–22 Both of the patients included in this study had Doppler ultrasonography prior to surgery for diagnosis of PMA thrombosis and BMN. It appears that only some of previous case studies reporting PMA thrombosis in CTS used ultrasonography for diagnosis prior to treatment, and in others the pathology was found at surgical exploration.1,23,25,30,36,37 Kele and colleagues used preoperative ultrasonography in a single case of PMA thrombosis CTS.33 They state that ultrasonography was beneficial for diagnosis of the pathology and influenced the selection of surgical equipment and anaesthesia used.33 It was also argued that preoperative ultrasonography may reduce the risk of iatrogenic trauma. There are no studies that have compared outcomes in PMA thrombosis CTS in patients who have and have not had preoperative imaging.
Management
The limited number of case studies that describe PMA thrombosis with CTS show inconsistencies in management. Conservative management with anticoagulation versus surgical management is the first and most significant divergence in treatment. In 2012, Rzepecka-Wejs and colleagues described a case of CTS with Doppler ultrasound proven PMA thrombosis that was managed with unspecified anticoagulant therapy and had nearly complete remission of symptoms over a three month follow up period.38 In 2015, Srivastava and colleagues also described an acute carpal tunnel with ultrasound proven PMA thrombosis that was treated with therapeutic enoxaparin and warfarin and had marked improvement in symptoms after four weeks of anticoagulation.39 Resolution of CTS symptoms and re-canalisation of PMA thrombosis with unspecified therapeutic anticoagulation was also reported in the case report by Salter and colleagues in 2011.23 Akgun and colleagues describe a case of CTS secondary to PMA thrombosis in an eight-week-pregnant woman where no treatment was undertaken by the patient because of the pregnancy, however, over the following weeks, the patient gradually became less symptomatic.1 It should be noted that these reports came from non-surgical specialties which may explain the preference for non-operative management.
In the two cases described here, the flexor retinaculum was released and the thrombosed PMA and BMN were left intact. The patients were not given anticoagulants. As far as we are aware, this is the first report to describe this surgical treatment for CTS secondary to PMA thrombosis. Two case studies describe reports of CTS secondary to PMA thrombosis where the flexor retinaculum was released and additionally the thrombosed vessel excised.25,30 In the 2002 study by Khashaba and colleagues the patient had ongoing numbness in the ring and index fingers for ten months postoperatively and had residual dysaesthesia over the radial aspect of the ring finger.30 Several studies have recommended that resection of the thrombosed PMA should generally be avoided because it involves the potential for vascular compromise in the hand.2,26,39 However, there are no reports in the literature that describe this occurring or that demonstrate a hand with full arterial dependence on the PMA. Arterial studies may be performed preoperatively to evaluate radial, ulnar arteries and PMA’s contribution to the hand’s circulation.
Conclusion
There are very limited studies reporting surgical management of BMN in CTS. Emphasis in reports is placed on preserving the median nerve branches while releasing the flexor retinaculum.7,24
In treating acute, severe carpal tunnel syndrome, we propose an open carpal tunnel release be performed and the nerve be inspected for the presence of an adjacent PMA. A thrombosed PMA can precipitate acute carpal tunnel syndrome with the consequent tissue inflammation causing an increase in carpal tunnel contents and subsequent provocation of pressure neuropathy. Previous experience of pressure neuropathy demonstrates that severity of nerve injury is a complex result of degree of ischaemia, duration of ischaemia and previous background injury together with patient medical factors. In the case of PMA thrombosis within the carpal tunnel, the ischaemic insult to the nerve will be of a dual nature: the injury to the arborisation of the arterial vascularity of the median nerve will be major, while the extrinsic compression from the enveloping walls of the carpal tunnel on the swollen contents will supplement the injury. It is reasonable to release the carpal tunnel as soon as possible and decide under direct vision at that time whether microsurgical resection of the thrombosed section of the artery will benefit the recovering nerve. That assessment will depend upon the overall balance of tissue tensions and that individual arterial pattern.
We have experienced benefit with preoperative Doppler ultrasonography. This included both diagnosis of pathology and the preoperative planning. As a result of ultrasonography findings, endoscopic approaches were not considered, markings were made to include a more proximal incision, both patients were in a state of general anesthesia and a consultant surgeon was present for both operations. Lastly, despite there being no discussions in the literature regarding the rate of recurrence with conservative management, surgical treatment as above can be considered more definitive and therefore potentially associated with a lower rate of recurrence.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Disclosure
The authors have no conflicts of interest to disclose.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Revised: June 25, 2018 AEST