Introduction
Factor V Leiden is a hereditary condition resulting in a mutation of the genetic composition of factor V, a clotting factor that forms part of the intrinsic clotting cascade. The mutation results in resistance against the normal degradation of factor V by activated protein C, leading to abnormally increased clotting. The risk of developing abnormal blood clots in heterozygous factor V Leiden patients is three to eight times the risk in the general population, while the risk for homogeneous patients can be as high as one in 12, or an 80-fold relative risk.1,2 Of the inherited thrombophilias, factor V Leiden is the most common: 5 per cent of Caucasians are affected, although incidence rates in other races are much lower than this.1 Inherited in an autosomal dominant manner, the incidence of those homozygous for the condition is estimated at less than 0.25 per cent, while the incidence of those heterozygous for the condition is 3–7 per cent.3 The prevalence in Caucasian Australians is even higher, with a newborn screening study finding 9.5 per cent of the population to be heterozygous.4
Microvascular free-flap reconstruction allows for the reconstruction of complex defects not amenable to repair by other reconstructive options.5,6 Free-tissue transfer involves the reconstitution of blood supply to the transferred tissue via microanastomosis of the artery and/or vein. The most significant morbidity in this process is flap failure due to thrombosis at the anastomotic site, both venous and arterial. Prevention of thrombotic complications typically involves careful vessel dissection and handling, meticulous surgical technique and well-described adjuncts such as heparin, aspirin and dextran.7,8 However, the literature supporting the use of these agents is varied and inconclusive.7 Perhaps more important is the preoperative planning and postoperative management of the patient receiving the reconstruction. Known risk factors for total or partial flap loss include smoking, diabetes, peripheral vascular disease, delayed reconstruction, older age and a technically difficult anastomosis.7–10 Although the risks, and management of many of these risks, are well documented in the literature, there is surprisingly little evidence on free-flap surgery outcomes in patients with factor V Leiden, despite factor V Leiden occurring in 1 in 20–25 Australians.11
Methods
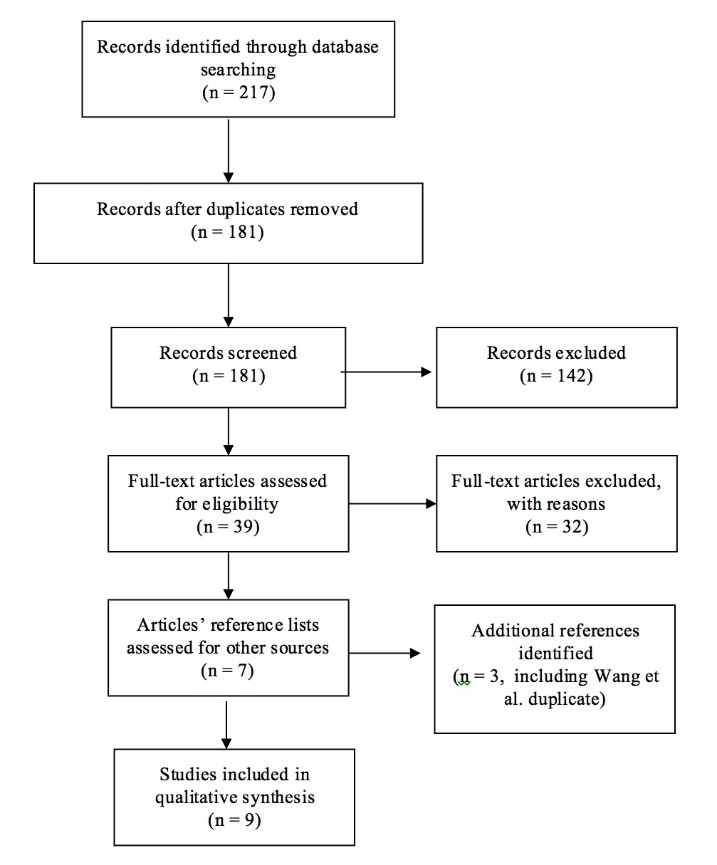
This article presents a qualitative analysis of the current literature regarding free-flap outcomes in patients with factor V Leiden. MEDLINE®, PubMed, EMBASE and Cochrane were searched from their dates of inception to March 2017. The PRISMA attrition flow diagram is shown in Figure 1. We searched ‘(free tissue flaps OR reconstructive surgical procedures OR surgical flaps OR microsurgery) AND (thrombophilia OR factor V)’. This yielded 217 results, including 36 duplicates. The two lead authors screened the titles and abstracts of these 217 articles and excluded studies that did not focus on free-flap surgery, did not differentiate between different types of hereditary thrombophilia, such that patients with factor V Leiden could be isolated out, or were not in English. Studies related to digit transplantation were excluded. Thirty-nine full-text studies were then assessed for eligibility, resulting in seven studies that met the inclusion criteria.

Through examining the reference lists of these seven studies, three additional studies that met the inclusion criteria were identified. It was noted that Wang and colleagues wrote two case series in 2012 and both included a patient with factor V Leiden.12,13 Only the case series with the greater number of patients with factor V Leiden was included in this review, since we did not want to count the same patient twice. Nine case studies or series (level IV evidence) were included in this review.
Results
Despite factor V Leiden being a relatively common and well-studied condition, literature on whether or not it affects outcomes in free-flap surgery is scant and limited to level IV evidence (case studies and reviews). Only nine studies, involving 22 patients in total, were found. These studies are outlined in Table 1. For many of the included cases, data on patients with factor V Leiden were extrapolated from studies on patients with thrombophilias in general.12,14,15 All patients had at least one free-flap operation, while two patients (Davison, Kessler and Al-Attar,14 Olsson and Hoijer16) had two simultaneous free-flap operations. This resulted in 22 patients with 24 free flaps in total. Nine flap failures were reported due to thrombotic complications. One free flap in the uncomplicated group suffered intraoperative thrombosis but was able to be salvaged. The same patient subsequently suffered a delayed deep vein thrombosis complication two months postoperation.16
Of the 22 patients, three had factor V Leiden where it was not specified whether or not they were homozygous or heterozygous,^12,17 12^ were heterozygous with unspecified mutations,16,17 two were heterozygous with the G1691A mutation,15,19 one was heterozygous with the R506Q mutation,20 one was a compound heterozygote (G169A and A4070G) with other thrombophilic mutations,20 two were heterozygotes (R506Q) with other thrombophilic mutations14 and one was a heterozygote (mutation not specified) with other thrombophilic mutations.21 Table 2 stratifies the patients and cases by their mutation type and compares mutation type with whether or not the free-flap survived.
Results from the current literature suggest that even heterozygous factor V Leiden patients have a relatively high risk of free-flap failure of 3/15 free flaps (20%). Patients who were heterozygous for factor V Leiden and had other coexistent thrombophilias had an even higher failure rate of 5/6 free flaps (83.3%). Importantly, these values do not control for the different types of anti-thrombotic treatments used across the various studies. A deliberate decision was made not to generate summary statistics such as odds ratios and relative risks because the sample size was too small and the quality of evidence too low.
Discussion
Limitations of the literature
The studies summarised in tables 1 and 2 suggest a trend towards patients with factor V Leiden, even those who are heterozygous, having an increased risk of free-flap thrombosis. Indeed, five out of the nine studies in this review included one or more patients with factor V Leiden who experienced free-flap failure secondary to a thrombotic complication. These results should be contrasted with the results of Arnljots, Söderström and Svensson’s large-scale case series,17 which found the rate of flap failure for patients with a thrombophilia (1/12 or 8%) to be comparable to the rate for patients without a thrombophilia (11/88 or 12.5%). The authors concluded that most flap failures were due to surgical factors, such as pedicle kinking and compression, rather than patient-specific factors.17 This aligns with current evidence suggesting that the commonest cause of free-flap failure is technical error.22
The most obvious explanation for this is that case studies are inevitably subject to publication bias. For patients with factor V Leiden who have successful free-flap surgery, their surgeons and even the patients themselves may never become aware of their thrombophilic status. In order to test this hypothesis, larger-scale case-control studies should be undertaken, especially since Arnljots, Söderström and Svensson’s18 study was done more than 20 years ago. The issue of publication bias is not unique to factor V Leiden studies, since the available literature on other inherited thrombophilias is also dominated by case studies.23–32
Since both factor V Leiden and patients who undergo free-flap reconstructions are relatively rare, a cohort or cross-sectional study would need to have an unfeasibly large number of patients in order to generate conclusions with meaningful statistical power. The optimal study type to answer the question of whether patients with factor V Leiden have worse free-flap outcomes would be a retrospective case-control study.33 A database of patients with factor V Leiden (heterozygous and homozygous) who had undergone free-flap surgeries would need to be gathered from an institution that performs a high volume of such operations. Each patient would then be matched to a patient in the control group who had similar baseline characteristics in terms of age, gender, medical comorbidities, smoking status and type of operation.
Another caveat is that certain elements of Arnljots, Söderström and Svensson’s18 study may not be applicable today. In the years since the inception of free-flap surgery in the 1970s, success rates of microsurgery have increased significantly.6 Given that their flap failure rate in patients without thrombophilias was 12.5 per cent, which is higher than the estimates given in recent much larger scale studies,5,34–37 it is probable that with the improvement in microsurgical techniques and instrumentation, the findings of this study have been surpassed. Current data suggest that expert surgical technique and proper patient selection may be the best ways to prevent microvascular thrombosis.7,38–40 One hypothesis is that, with increases in technology leading to a reduction in operator-dependent microsurgical complications, the relative influence of patient comorbidities, including thrombophilias, has become more significant than the relative influence of surgical factors on free-flap outcomes.
Clinical implications: a role for preoperative screening strategies
Free-tissue transfer is the most complex technique in the reconstructive surgeon’s armamentarium. As such, failure may result in a patient being left with no reconstructive options other than another free flap.5,6 Flap loss results in stress for both the patient and the surgeon, with a long list of subsequent complications including exposure of essential structures and hardware, leaks or fistulas and the need for multiple repeat operations. Thus, failed free flaps represent a significant cost not just for the patient, but also for the healthcare system.5,41,42 In Australia, the cost of flap salvage has been estimated at A$3045 and the cost of replacing a flap with a new free flap has been estimated at A$5075.21.
Given the paucity of high-level evidence on outcomes of free-flap surgeries in patients with factor V Leiden, there is disagreement as to whether surgeons should routinely screen free-flap candidates prior to surgery. Pannucci, Kovach and Cuker38 argue that we do not yet have enough information on the relative risks of microvascular thrombosis and flap failure in patients with hereditary thrombophilias. Indeed, a pathophysiological link between factor V Leiden and microvascular or intra-anastomotic thrombosis has not yet been proven. Most evidence for preoperative risk factors for thrombosis in this patient population relate to macrovascular events, such as venous thromboembolisms.7
The screening algorithm suggested by Pannucci, Kovach and Cuker stratifies patients according to whether or not they need preoperative review by a haematologist.38 They recommend that patients with a personal or family history of thrombosis, with acquired risk factors such as malignancy or with a ‘high-risk’ Caprini score be seen by a haematologist. This differs from the screening algorithm suggested by Friedman and colleagues43 in that a haematologist is consulted prior to ordering the thrombophilic screen. However, the 2005 Caprini risk assessment method,44 which has been validated in plastic surgery patients,45,46 already includes personal and family history of thrombosis (each worth two points), as well as a range of acquired risk factors. Pannucci, Kovach and Cuker do not provide a cut-off Caprini score above which they suggest referral to a haematologist. This could be problematic since most free-flap candidates would have a baseline score greater than or equal to six, qualifying them for haematologist referral (age 60–74 = 2, malignancy [present or previous] = 2 and major surgery [> 45 minutes] = 2).
The importance of routinely screening patients is highlighted in Sezgin’s 2016 study.47 Sezgin conducted a prospective cohort study using his own preoperative algorithm to detect thrombophilic patients: 60 patients who were to undergo free-flap breast surgery were questioned on their prothrombotic risk factors. Patients with suspicious personal or family histories underwent thrombophilia panel testing. Sezgin found that 35 per cent (21/60) of patients had a positive history for prothrombotic tendencies; that is, they answered ‘yes’ to one or more of his screening questions. The questions asked about ‘any previous thromboembolic event concerning the patient or family member, diseases or medications that may cause predisposition to thrombosis, the presence of varicose veins and history of deaths in utero and miscarriages’. Unfortunately, Sezgin does not include the questionnaire itself, so it is unclear how detailed it is. If it included a large number of common acquired risk factors, such as a previous history of cancer or smoking, it is understandable that greater than one-third of his patients were found to have positive histories.47
Even so, Sezgin reported that 9/21 (42.9 %) of these patients (9/60 or 15% of total patients studied) were newly diagnosed with a congenital thrombophilia. He writes: 'Four patients were diagnosed with MTHFR gene mutations accompanied by hyperhomocysteinemia, while two patients had activated protein C resistance (factor V Leiden), two patients had decreased antithrombin III activity and one patient had protein S activity deficiency. None of the patients were aware about their thrombophilic states beforehand.47 DeFazio and colleagues speculate that Sezgin’s unusually high rate of thrombophilic patients might be due to this patient population having disproportionately high rates of comorbidities that cause them to present as candidates for free-flap surgery.15 Thrombophilic patients were deemed not for free-flap surgery and were given pedicle flaps or implants instead.47
Conclusion
Current evidence for outcomes of free-flap reconstruction in patients with factor V Leiden is limited to nine studies of level IV evidence, totalling 22 patients who underwent 24 free-flap operations. Out of these 24 operations, nine free flaps failed due to thrombotic complications; one free flap suffered intraoperative thrombosis but was salvaged. Although the literature suggests a trend for patients with factor V Leiden being at increased risk of free-flap thrombotic complications, the low level of evidence and small sample sizes of the extant studies mean that a definitive conclusion cannot be drawn.
Nevertheless, given the significant economic and psychological costs associated with failed free-flap reconstructions, the use of a simple, non-invasive screening protocol has significant potential. We agree with the recommendation of Pannucci, Kovach and Cuker38 that institutions would benefit from having a preoperative screening protocol that involves taking a thorough history and then referring high-risk patients for haematology review. Beyond this, it is up to the discretion of the surgical department whether they adopt a radical approach of not offering free flaps to any patients with factor V Leiden (including heterozygotes), or whether they simply work with the haematologist to minimise the patient’s risk through a combination of more aggressive chemoprophylaxis, meticulous surgical technique, more frequent postoperative flap monitoring and educating the patient on his/ her increased risk profile.
Such an approach has many merits: it is cost-saving, easy to implement and could foster stronger cross discipline collaboration between plastic surgeons and haematologists. Scope for further research includes whether or not adopting such a protocol would be cost-saving for an institution or lead to fewer free-flap complications. Further study should also be undertaken into the molecular pathways involved in microvascular thrombotic events and whether or not such pathways are altered in patients with factor V Leiden.
Disclosures
The authors have no conflicts of interest to disclose.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Prior publication
This study was presented as a poster at Plastic Surgery: The Meeting, Chicago, 2018.