
Introduction
Complex extensor tendon injuries of the fingers can be associated with a slow and unpredictable recovery.1,2 The extensor mechanism consists of a flat, delicate and complex tendon system. It has a broad gliding interface with its overlying subcutaneous areolar tissue and the underlying metacarpal or phalangeal periosteum. Interruption of this gliding plane results in reduced range of movement, joint contracture, pain and functional loss in the affected digit.2–4
While reconstruction of individual anatomical components is feasible, re-establishing these areolar gliding planes for tendon excursion remains a surgical challenge. In acute injuries, either staged reconstruction or the use of a non- vascularised tendon graft can be considered. In delayed operations, extensor tenolysis may be used to resolve adhesions interrupting tendon excursion. However, due to poor tendon vascularity, a scarred tissue bed or underlying fractures, adhesion formation often prevails.2,3,5
We postulate the use of a vascularised composite flap of extensor retinaculum and the overlying skin to reconstruct complex dorsal digital injuries. This composite tissue flap would provide vascularised tendon graft, the overlying skin and a potential intervening gliding plane, thus enhancing tendon excursion. The present study aims to demonstrate the microvascular supply to this composite flap in a cadaveric model.
Methods
Twenty upper limbs, disarticulated at the mid-arm level, from 10 fresh frozen cadavers were obtained through the University of Tasmania’s body bequest program. The study was approved by the Tasmanian human research ethics committee (HREC H0015063). All specimens were free from scars, previous surgery or trauma of the forearm, wrist and hands. Two upper limbs from one fresh frozen cadaver were used in a pilot study to establish the study’s protocol. Once established, the anatomical study comprising the remaining 18 upper limbs from the other nine cadavers was conducted.
A proximal volar forearm incision was made at the midline of the cubital fossa, and the brachial artery was identified first. The ulnar artery was then further exposed by reflecting the flexor digitorum superficialis. The common interosseous artery was traced from the ulnar artery at the level of the radial tuberosity superficial to the flexor digitorum profundus. The short common interosseous artery was then followed deeper to its two terminal arteries, the anterior interosseous artery (AIA) and the posterior interosseous artery (PIA), at the interosseous membrane. The AIA (n = 9) or PIA (n = 9) was selectively cannulated at its origin using an 18-gauge cannula.
The ulnar artery was ligated just proximal to Guyon’s canal through a volar wrist stab incision. The radial artery was ligated just proximal to the anatomical snuff box through a stab incision between the flexor carpi radialis and the abductor pollicis longus tendons. The ulnar and radial arteries were ligated at the wrist to prevent retrograde flow, thus minimising artefact and isolating perfusion to either the AIA or the PIA.
The specimens’ vasculature was prepared as described by Ross and colleagues.6 The specimens were injected serially with warmed normal saline (37 °C) and subsequently with coloured ink. Any vascular leaks were identified and sealed, with either silk sutures or monopolar diathermy.
A dorso-ulnar wrist skin flap, approximately 3 × 4 cm in size, overlying the extensor retinaculum was marked distal to the ulna head. The flap was raised with the proximal portion of the extensor retinaculum. This composite flap consisting of skin and the extensor retinaculum was based on perforators between the fourth and fifth extensor tendon compartments. Care was taken not to separate the skin from the retinaculum. A longitudinal dorsal forearm incision about 3–5 cm in length was made, extending from the proximal border of the flap. In dissecting the PIA pedicle specimens, the intermuscular septum between the extensor digiti minimi (EDM) and the extensor carpi ulnaris (ECU) was opened to locate the PIA. In dissecting the AIA pedicle specimens, the interosseous membrane (IOM) was incised to identify the AIA. All flap dissections were performed under 2.5× surgical loupe magnification.
After flap dissection, each specimen was injected with a barium sulfate-gelatin radio-opaque medium as described by Saint-Cyr and colleagues.7 Specimens underwent time-rendered digital subtraction angiography (DSA) during contrast injection. Additional cone-beam computed tomography angiography (CTA) post contrast injection was obtained (Siemens Artis Zee, Siemens, Germany). Multi-planar reconstruction (MPR) and 3D reconstruction in volume-rendering technique (VRT) were used to visualise the patterns of microvascular perfusion of the extensor retinaculum and overlying integument. Image post-processing was performed using OsiriX 4.0 (Pixmeo, Switzerland) and Siemens syngo (Siemens, Germany). All vessel dimension measurements were undertaken on cone-beam CTA images. The perforator diameter was measured at its origin from the pedicle vessel. The perforator diameter was measured on axial and coronal slices to ascertain its cross-sectional dimension.
Results
Of the nine fresh frozen cadavers, four were female and five were male. Their mean age at death was 80 ± 10 years (SD). None had documented peripheral vascular disease, however, seven had cardiovascular disease.
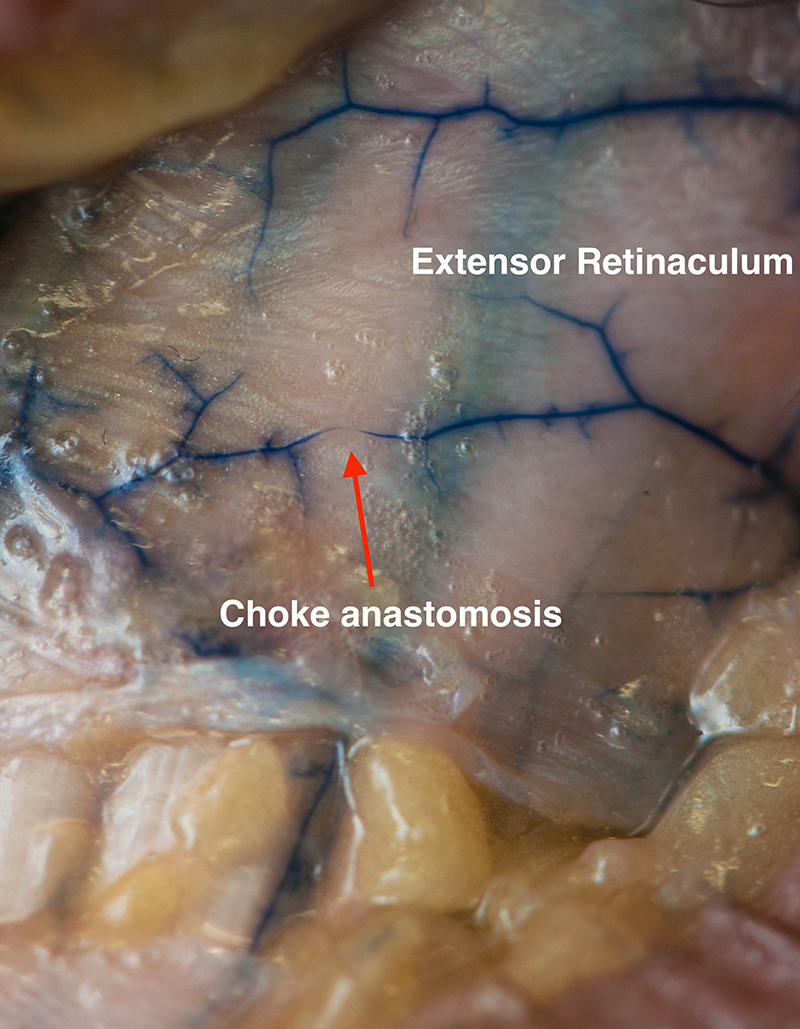
Both AIA and PIA contributed to a dense network of vessels to the extensor retinaculum (Figure 1). Terminal branches of both vessels also penetrated the extensor retinaculum and provided cutaneous perforators.
Anterior interosseous artery
The AIA consistently supplied the integument of the distal dorsal forearm and wrist. On exposure of the extensor retinaculum, a dense network of vessels spanning the entire width of the extensor retinaculum was present.
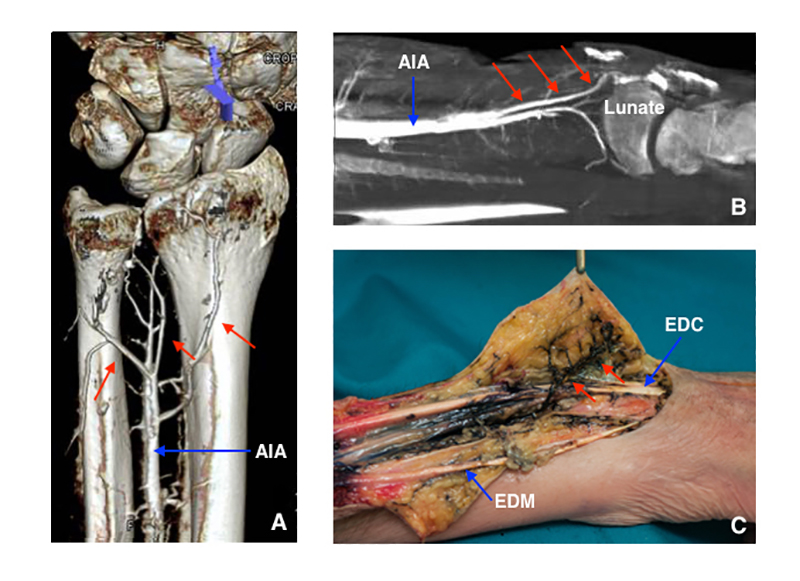
The AIA penetrated the IOM approximately 5 cm proximal to the ulnar styloid process, then coursed distally along the dorsomedial surface of the radius and terminated in the dorsal carpal arch (Figure 2). Large septocutaneous perforators from the AIA were consistently seen arising between the fourth and fifth extensor tendon compartments. One to two septocutaneous perforators were found, supplying the extensor retinaculum and overlying skin (Table 1). The mean diameter of these perforators was 0.4 ± 0.1 mm (SD; Table 2). Additional perforators were also invariably present between the second and third and the third and fourth extensor tendon compartments.
_3d_vrt_reconstruction_after_cone-beam_ct_acquisition_in_ap_view_of_an_aia_specimen_showin.jpg)
Posterior interosseous artery
The PIA supplied a well-circumscribed area of integument over the proximal dorsal forearm. It travelled along the dorsal aspect of the interosseous membrane between the EDM and ECU. It terminated in anastomoses with the dorsal carpal arch.
Exposure of the extensor retinaculum revealed that the PIA supplied the ulnar-sided perforators only (Figure 3). Dominant septocutaneous perforators were seen arising between the fourth and fifth extensor tendon compartments. Inconsistent perforators were seen between the fifth and sixth extensor tendon compartments. Again, there were one to two perforators penetrating the extensor retinaculum, supplying the overlying skin (Table 1). The mean diameter of these perforators was 0.3 ± 0.1 mm (SD; Table 2).
_at_the_fourth_and_fifth_extensor_tendon_c.jpg)
A composite flap incorporating a portion of the extensor retinaculum and the overlying skin was subsequently raised, based on perforator vessels located between the fourth and fifth extensor tendon compartments from both AIA and PIA (see supplementary video).
Discussion
The extensor mechanism of the digits is a broad, flat structure that is reliant on the low-friction gliding planes between the tendon itself and its adjacent areolar tissues.2,4,8 Functional outcomes following extensor tendon repairs rely on maintenance of these low-friction gliding surfaces to facilitate early and adequate tendon excursion.4,8 We postulate that the extensor retinaculum cutaneous composite flap is a technique for reconstructing the extensor tendon after complex injuries. The histology of the extensor retinaculum consists of an inner gliding layer with hyaluronic acid–secreting cells that allows tendon excursion.9 Non-vascularised extensor retinaculum graft has been described in the reconstruction of extensor tendon defects.10 As a composite unit, the extensor retinaculum cutaneous composite flap may provide a natural tendon–skin low-friction interface that is required for tendon excursion.
The present study is the first to propose the anatomical feasibility of a free vascularised extensor retinaculum composite flap based on the AIA or PIA pedicles. In our investigation, septocutaneous perforators from both the AIA and the PIA were consistently seen arising between the fourth and fifth extensor tendon compartments. A composite free flap consisting of the proximal extensor retinaculum and its overlying skin could be raised based on these vessels. The microvascular anatomy of this composite flap appeared predictable and feasible for free-tissue transfer.
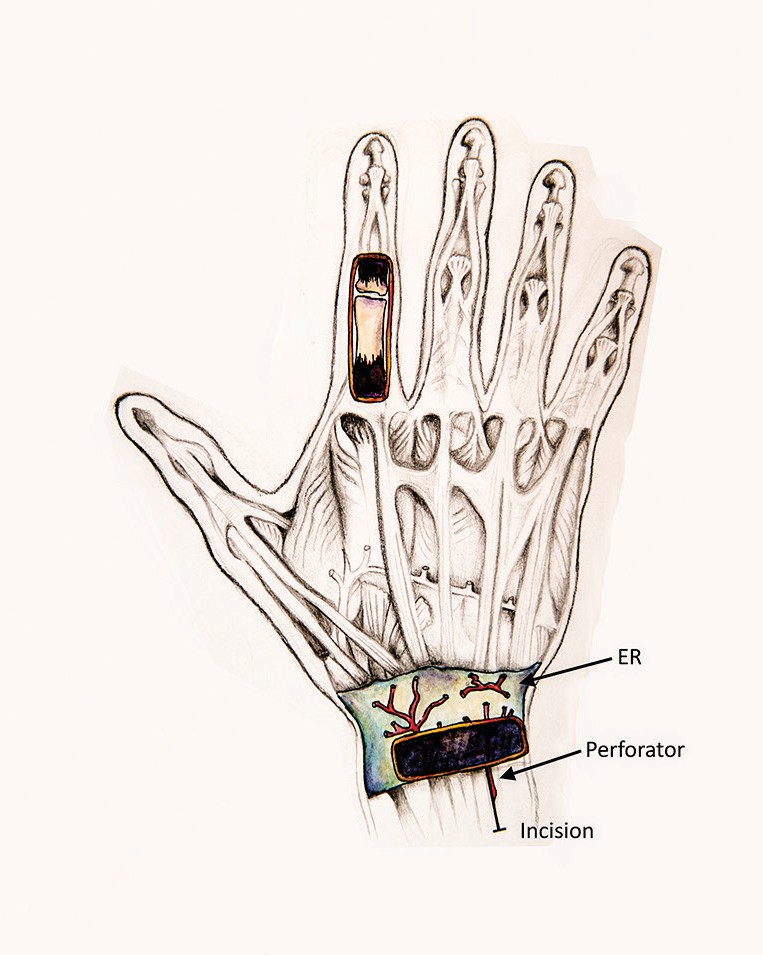
In harvesting this composite flap, the dorsal wrist skin and proximal half of the extensor retinaculum could be elevated in toto, consequently preserving the septum between the fourth and fifth extensor tendon compartments (Figure 4). Proximal extension of the incision allowed the communicating perforator to be traced to either the AIA or the PIA. If in doubt, a microvascular clamp can be applied to the AIA and PIA, sequentially, to identify the dominant arterial supply.

Based on the perfusion of the desired flap design, the selected pedicle vessel is dissected to the required length and divided. The pedicle length attained was approximately 5 cm. The pedicle diameters were sufficient for microvascular anastomosis. We found this dissection technique uncomplicated in cadaveric specimens.
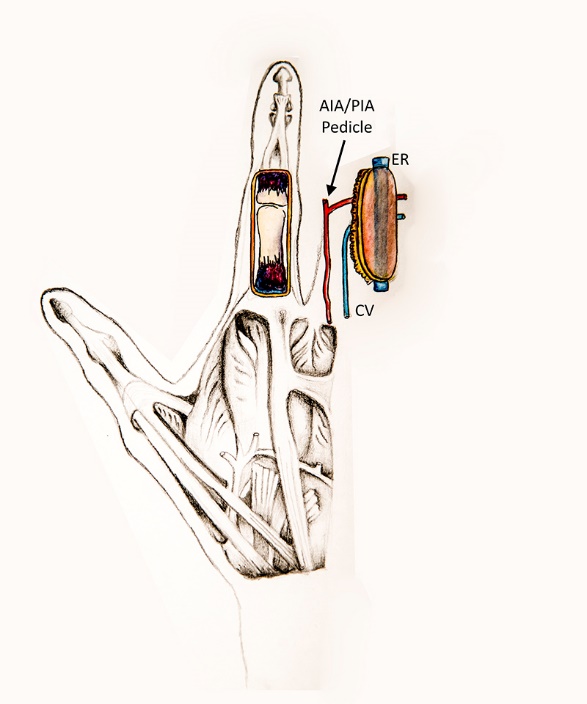
The resultant composite free flap is placed with a 90-degree rotation to fill the extensor tendon defect (Figure 5). The extensor tendon defect is reconstructed with the vascularised tendon graft and a skin paddle inset. The pedicle artery can be anastomosed to the dorsal branch of the radial artery and the veins can be anastomosed to suitable dorsal veins of the hand or digit.
_composite_flap_is_then_placed_with_a_90-degree_rotation_to.jpeg)
This flap is envisaged for both immediate reconstruction of single-digit injuries with composite tissue loss and delayed reconstruction of a persistently stiff finger where extensor tenolysis has failed. It would allow for skin, areolar tissue and tendon to be reconstructed in a single operation. Single-stage reconstruction has been shown to be superior when compared with multiple-staged reconstructions, exhibiting greater articular mobility, earlier return to work and reduced revision rates.11–14
Donor site morbidity is anticipated to be minimal from the flap harvest. The donor site is able to be closed primarily, the flap uses non-axial vessels and the majority of the extensor retinaculum is preserved. In a study by Barr and colleagues8 where extensor retinaculum was excised, patients did not suffer from any donor site morbidity. Brody and Merrell15 also found that if the proximal portion of the extensor retinaculum was removed, the resultant bowstringing and extensor tendon lag were minimal, if not negligible. The flap can also be harvested from the ipsilateral dorsal wrist and hence within the same operative field.
However, when harvesting the pedicle vessel, division of the IOM may be required and consequently the posterior interosseous nerve (PIN) may be affected. The dorsal oblique band of the IOM has been shown to be a secondary stabiliser for the distal radioulnar joint and only limited division should be carried out.16 The terminal PIN sends proprioceptive and nociceptive branches to the distal radioulnar joint and scapholunate ligament.17–19 The significance of this sensory input on wrist stability has been disputed by some study groups.17–19 Nonetheless, efforts should be taken to protect the PIN during pedicle vessel dissection.
This anatomical study is associated with certain limitations. A cadaveric study was conducted and its clinical application has not been tested. The sustainability of the flap, its biomechanical success and donor site morbidity remain to be established.
The radiological studies all evaluated the arterial inflow phase and the reliability of the cutaneous venous drainage of the entire flap is yet to be determined. A disadvantage of this technique is that it is limited to reconstruction of a single digit. Furthermore, patients with a larger body habitus may have excessive subcutaneous bulk, making an excessively thick composite flap. The pedicle length may prove to be challenging for little finger reconstruction.
Conclusion
This study has established the arterial supply to the extensor retinaculum of the wrist by both the AIA and the PIA. Septocutaneous perforators were consistently seen between the fourth and fifth extensor tendon compartments from both the AIA and the PIA. The microvascular anatomy of the proposed composite flap appeared consistent and sufficient to be used for free-tissue transfer. Flap dissection in the cadaver specimens was technically feasible. The described composite flap provides vascularised tissue reconstruction in complex extensor tendon injuries, which has the potential to allow early rehabilitation and recovery.
Acknowledgements
The authors would like to thank Mandhi Allen and Michelle Boutchard: their help in this study was invaluable. Many thanks also to Rhiannon Menzie for her detailed illustrations.
Disclosures
The authors have no conflicts of interest to disclose.
Funding
The School of Medicine at the University of Tasmania, and the Department of Medical Imaging and the Department of Plastic and Reconstructive Surgery at the Royal Hobart Hospital funded this study.
Prior publication
The results of this study have been presented at the 2016 Combined Meeting of the Australian Hand Surgery Society and the American Society for Surgery of the Hand in Sydney, Australia.
Revised: July 14, 2019 AEST