Introduction
Palmaris profundus is an anatomical variation, usually found incidentally during carpal tunnel release. Its location deep to the transverse carpal ligament can cause compression of the median nerve. This unusual cause of carpal tunnel syndrome can persist, despite adequate release, and may require resection of the palmaris profundus.
Case
A 79-year-old, right-handed man presented with a 12-month history of bilateral paraesthesia and pain in both hands. He experienced pain particularly when driving and at night, when it woke him from sleep. The left hand was more symptomatic than the right. On examination he had paraesthesia in the median nerve sensory distribution and Phalen’s test was positive. His past history was significant for ischaemic heart disease, prostate cancer and renal impairment.
A nerve conduction study was requested by his general practitioner and this showed decreased sensory latency of the median nerve bilaterally, in keeping with moderate to severe carpal tunnel syndrome.
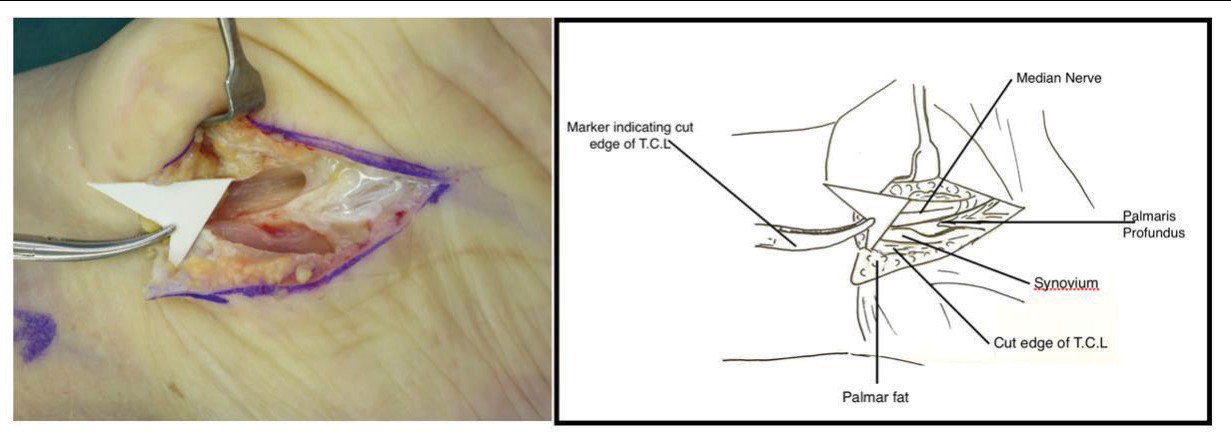
A right open carpal tunnel release was performed. The skin incision and transverse carpal ligament (TCL) were divided in the usual fashion under direct vision. The median nerve was identified and protected. Unusually, an additional tendinous structure was identified deep to the TCL (Figure 1). This structure was radial and volar to the median nerve and appeared to be contained within the same fascial sheath. It then dispersed and became continuous with the deep aspect of the palmar aponeurosis of the hand. Traction on this tendon did not cause either excursion or relaxation of the palmaris longus (PL) tendon and was thus determined to be a separate structure. A more proximal dissection was not clinically indicated and thus not performed.
His left carpal tunnel release was performed some months prior to the right by the same surgeon. He was noted to have normal anatomy on the left. Postoperatively, his carpal tunnel symptoms resolved completely.
Discussion
The palmaris profundus (PP) tendon was described by Frohse and Fränkel in 1908.1 While numerous case reports and anatomical dissections have been described, there has been no comprehensive account of its incidence. Reimann and colleagues found one cadaver with bilateral PP in a dissection of 1600 extremities.2 Although this suggests an incidence of 1 in 800, given the relative paucity of reports, it would appear that it is even less common.
A review of the literature found several case reports, of which approximately a quarter were anatomical studies. As was the case with our patient, most cases of PP were found incidentally during carpal tunnel release. Four cases of bilateral PP were reported.2–4 Of the remainder, the majority were found to be on the right side. With the data available, this would seem to indicate that PP has a right side preponderance of 6:1.
Three subtypes of PP were described by Pirola and colleagues based on its origin: type I arising from the radius, type II arising from the flexor digitorum superficialis fascia and type III arising from the ulna.5 Other origins have been described, including the common flexor origin, the epimysium of the flexor pollicis longus and the PL. In every case where the insertion was reported, the PP attached into the deep aspect of the palmar aponeurosis. PL was noted to be absent in some cases.4–6
Palmaris profundus has been described as ‘musculus comitans nervi mediani’ due to the fact that the tendon of PP appeared to be within the same fascial sheath as the median nerve.7 While almost always volar to the median nerve, PP was usually found on the radial side of the nerve, though in one case it was reported as crossing the nerve from the radial to the ulnar side.6
In two cases, PP was observed and left in situ at the primary operation.8,9 When symptoms did not resolve or recurred, the patients underwent a revision where PP was excised. Both authors reported that each patient’s symptoms resolved following resection of the PP tendon. It is well known that any increase in the volume of the carpal tunnel—be it synovitis, oedema or aberrant structures—causes carpal tunnel syndrome. McClelland and colleagues found that PP impeded endoscopic carpal tunnel release, requiring conversion to an open procedure.10
Conclusion
Palmaris profundus is a rare anatomical variation that can cause carpal tunnel syndrome. It is usually unilateral with a right side preponderance. The origin of the muscle can be variable while its insertion is reliably the deep aspect of the palmar aponeurosis. It is usually found incidentally at the time of carpal tunnel release and may be a cause of failed endoscopic carpal tunnel release. Excision of the aberrant tendon can lead to resolution of the symptoms, whereas leaving it may cause to the patient to require revision surgery.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Disclosures
The authors have no conflicts of interest to disclose.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.