
Introduction
Accurate diagnosis, and prompt treatment, of a severe necrotising soft-tissue infection is one of the few diagnoses in plastic surgery that, if managed correctly, can be life-saving. A high degree of awareness and medical knowledge of this condition is important for the assessing surgeon who will determine the course of treatment. Early clinical findings of necrotising fasciitis may be limited to pain, mild swelling and redness. However, serial examinations will show failure to respond to antibiotics and progressive systemic signs of sepsis including haemodynamic instability, acidosis, leucocytosis and hyperthermia. The progression of a necrotising soft-tissue infection is variable and multifactorial. Most commonly, it presents with rapid progression and is life-threatening.
Differentiating necrotising infections from other soft-tissue infections can be challenging, especially in the early stages. In addition, other differential diagnoses, including non-infectious conditions, should be considered. Described below is the diagnostic conundrum of a patient presenting with a rare type of cutaneous lymphoma, primary cutaneous gamma-delta T-cell lymphoma (PCGDTL) associated with haemophagocytic lymphohistiocytosis (HLH), mimicking a necrotising soft-tissue infection.
Case
A 21-year-old male presented with one week of high-grade fevers (> 39 ˚C) and right thigh swelling. He was a smoker with no other significant medical history. On admission, the right thigh was painful and indurated. Due to clinical deterioration, concerns were raised for a necrotising soft-tissue infection, for which the patient was urgently taken to theatre.
Intraoperatively, an incision was made over the swollen area on the right thigh. Macroscopic exploration revealed the normal appearance of fascia and skin layers. Multiple biopsies were taken and the wound was dressed with a negative- pressure dressing. Despite continuous medical therapy and the innocuous surgical and pathological findings, the patient became haemodynamically unstable, requiring intensive care and ionotropic support. A second exploration was warranted. This revealed large amounts of grey, non-viable areas of subcutaneous tissue. However, the underlying fascia remained pristine. The abnormal areas of subcutaneous tissue were resected and sent for histopathology, which was reported as unspecific fat necrosis. Tissue and blood cultures showed no evidence of a micro-organism. In intensive care, the patient continued to deteriorate with multi- organ failure and disseminated intravascular coagulation requiring mass blood transfusion. He then gradually stabilised and was transferred to the ward under the multidisciplinary care of plastic surgery, general medicine and infectious diseases.
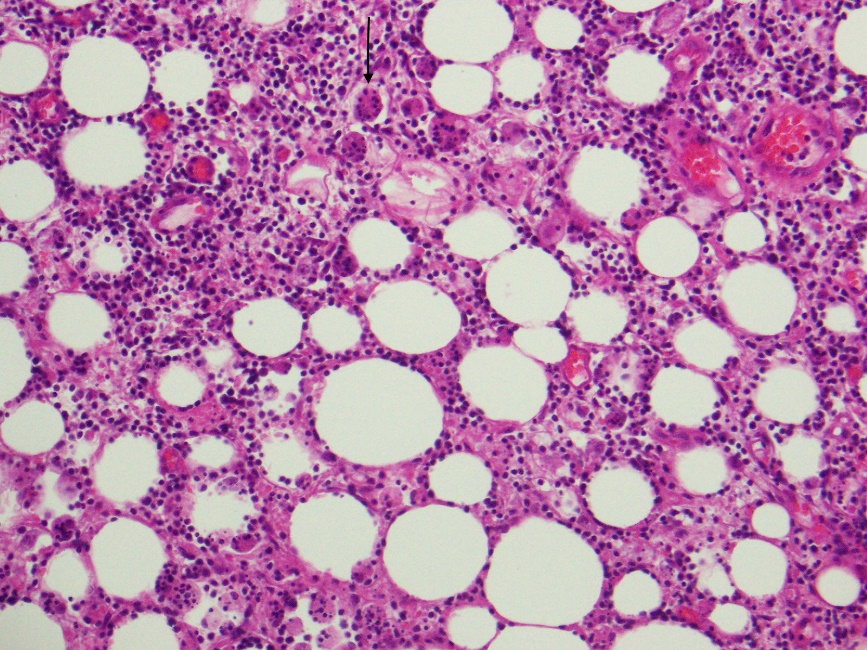
Several weeks into his admission, with ongoing high-grade fevers and negative cultures, the patient developed multiple areas of non-tender plaque-like rash over his torso and limbs (Figure 1). Punch biopsies of the newly formed skin lesions revealed the diagnosis of primary cutaneous gamma-delta T-cell lymphoma (PCGDTL) associated with haemophagocytic lymphohistiocytosis (HLH). In light of this, the initial intraoperative biopsy samples were re-reviewed by expert dermatopathologists who confirmed that PCGDTL was the missed diagnosis (Figure 2). The patient’s symptoms and fever settled once chemotherapy commenced.

Discussion
For this patient, the PCGDTL presented as disseminated subcutaneous deposits with swelling, pain and erythema but intact skin. Primary cutaneous gamma-delta T-cell lymphoma may, in other cases, affect skin integrity, leading to ulceration or necrosis. It is more commonly located on the extremities but can also appear on mucosa and other extra-nodal sites.1,2 The high-grade fevers that our patient experienced can be attributed to HLH, which is due to the uncontrolled activation of the immune system by abnormal proliferation of T-cells and activation of macrophages and histiocytes. The soft-tissue swelling, accompanied by high-grade fever, increasing inflammatory markers and progressive clinical deterioration, mimicked necrotising fasciitis. However, soft- tissue infection was ruled out for our patient as no microorganism was cultured and his symptoms did not improve with antibiotics or surgical debridement.
Repeating and reviewing previous investigations is crucial in the context of unexpected clinical progress with new or ongoing symptoms. Likewise, this case highlights the importance of a multidisciplinary approach in treating complex clinical presentations, which may help clinicians to diagnose rare conditions.
Until recently, PCGDTL was considered a subtype of subcutaneous panniculitis-like T-cell lymphoma (SPLTCL).3 However, due to the aggressive nature, and significantly worse prognosis of the gamma-delta subtype, in 2008 the World Health Organization drew a distinction between the more indolent SPLTCL and PCGDTL.4 The rare and significantly more aggressive PCGDTL represents less than 1 per cent of all primary cutaneous T-cell lymphomas.5 Although our patient was younger, the median age of onset is 60 years, with a range between 25 and 91 years in previous reports.6 As in our patient’s case, PCGDTL may be associated with HLH, especially in the presence of panniculitis-like tumours.1,2 This subtype of T-cell lymphoma has a poor prognosis with a median survival time of only 15 months.1,2 Treatment is with chemotherapy; however, PCGDTL is often resistant to multi-agent chemotherapy. The prognosis is worse when the condition is associated with HLH.
Conclusion
When treating a possible severe soft-tissue infection, clinical vigilance and a multidisciplinary approach are essential to provide the best clinical setting to manage complex cases and are both key when facing diagnostic dilemmas. In addition, another aetiology mimicking infectious conditions, such as a rare primary cutaneous lymphoma, should be considered among the differential diagnoses.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Disclosures
The authors have no conflicts of interest to disclose.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Revised: May 28, 2019 AEST