Introduction
Epidemiology
Cutaneous squamous cell carcinoma (cSCC) is the world’s second most common skin cancer after basal cell carcinoma (BCC).1 Together they comprise the world’s most common malignancies.2 Compared to BCC, cSCC is more invasive, metastatic and recurrent post-treatment.3 Each year, around 1.8 million people globally are diagnosed with cSCC4; and approximately 15,000 Americans die from cSCC complications, surpassing 10,000 melanoma deaths.5 These figures are estimated due to a relative paucity of data about cSCC management and complications.6–8 Concerningly, the global incidence of cSCC jumped 310 per cent between 1990 and 2017, higher than any other malignancy.4 Ultraviolet radiation from chronic sun exposure is the top risk factor for developing cSCC,9,10 which explains its tendency to appear on the head and neck.11,12 Like most skin cancers, cSCC is more common in people with albinism13 and Caucasians14 proximal to the equator.15,16
Other risk factors include chronic wounds,10 immunosuppression,17,18 dermatoses, previous malignancy, actinic keratosis,11 increasing longevity, male sex, smoking19,20 and other carcinogens.21 Yet, such nuanced variables require further analysis to better understand the 310 per cent incidence leap. For example, should the effect of increasing longevity be teased out from slowing Caucasian population growth and falling smoking rates? Similarly, does enhanced surveillance of elderly skin allow higher reporting of cSCCs that would otherwise be undetected?
Research focus
This paper reviews close/positive margins in cutaneous squamous cell carcinoma of the head and neck (cSCCHN), ensuing recurrence, regional or systemic metastasis, mortality and follow-up management. The aim is to provide clinicians with up-to-date statistical evidence regarding the management of close/positive margins for cSCCHN, hopefully allowing better-informed management plans.
Low-risk versus high-risk cSCC lesions
Low-risk cSCC lesions include well differentiated primary tumours < 2 cm in diameter,22,23 especially in the peripheries.24 High-risk features include close/positive margins6; recurrent disease; radial dimensions > 2 cm,23 depth > 6 mm; invasion of subcutaneous fat, perineural or lymphovascular structures13; and distant metastasis. High-risk locations include the aesthetically and functionally sensitive regions of the head, such as the anatomical H-zone (‘mask area’) which overlaps the midface and ears.21
Excision margins
Surgical excision with clear radial and deep margins is the mainstay of cSCC management and provides lower rates of recurrence and mortality than close/positive margins.6,25,26 Broadly speaking, cSCCHN surgery is divided into standard (traditional) excision and microscopically controlled Mohs surgery. Standard excision is much faster and cheaper to perform than Mohs surgery. However, there is some evidence that the painstaking step-by-step histological analysis during Mohs surgery tends to provide better cosmetic outcomes and preservation of function, and lower rates of recurrence and mortality.27,28
Nevertheless, surgeons can find it difficult to achieve clear margins when seeking to preserve vital aesthetic and functional head and neck components, such as the orbit.11 Thus, it is not uncommon to achieve close or even positive excision margins, which unfortunately are among the worst prognostic factors for a recurrence of cSCC, metastasis and mortality.6,18 This is especially true of cSCCHN with deep margins.7,26,29–32
Ideally, a positive (incomplete, involved or surgical failure) margin can be defined as having tumour cells on histopathology.33 However, it is logical to expand that definition to include a margin of ≤ 1 mm.33–35 This is because histopathology techniques such as bread loafing are imperfect and it is not uncommon to find previously unnoticed microscopic cSCC on follow-up histopathology.34–36 Further, it can be especially difficult to detect microscopic cSCCHN satellites on deep margins.30 To complicate matters, there is considerable overlap in the literature between positive and close margins. For instance, close cSCC margins range from ≤ 1 mm37 to at least < 5 mm.38–40 Therefore, close and positive margins are often grouped as a single entity.41,42 This is not surprising given that close margins are often positive on subsequent histopathology35 and higher rates of recurrence are associated with close/positive margins compared to clear margins.33
In contrast, cSCC clear (negative) excision margins can be deemed free of cSCC on histopathology.43 However, cSCC clear margins are also defined in the literature as ≥ 1 mm,44 or > 4 mm,32 or > 5 mm,23 or > 6 mm,13,23 or > 9 mm23 or ≥ 10 mm.33 This variability is partly influenced by whether the tumour is considered low or high risk. Indeed, the National Comprehensive Cancer Network (NCCN) guidelines recommend that cSCC lesions < 2 cm in diameter in lower risk regions should be excised with 4 mm margins to ensure a 95 per cent likelihood of non-recurrence.23 Whereas lower risk lesions > 2 cm should be afforded a 6 mm margin.23 Yet, in high-risk periorbital and auricular regions, where cSCC is prone to invade subcutaneous tissue, the NCCN recommends a 4 mm margin for tumours < 1 cm, 6 mm for tumours 1–1.9 cm and 9 mm for tumours ≥ 2 cm.23 Given that the definitions of clear and close margins can overlap, the authors will define a clear margin as free of cSCC on histopathology or at least > 4 mm, a minimalist NCCN definition.
Managing close/positive margins
Surgical re-excision with adequate margins (as noted above) is the gold standard for positive and at-risk close margins in cSCCHN.45 Nevertheless, further surgery is not always feasible, as it may unduly endanger critical head and neck structures; or require a complex reconstruction in an otherwise medically unstable patient.46 Other multidisciplinary meeting planning considerations include patient preference, the difficulty of attending surgical appointments for immobile elderly patients and futility in distant metastases.
In such cases, radiotherapy (RT) is often preferred, either with curative or palliative intent, depending on multidisciplinary review of patient prognosis.13,47 There is also some evidence that adjuvant RT following re-excision may be better than surgery alone.48,49 Dosing fractionations for RT vary depending on patient fitness, the size of the cSCC and whether there is regional disease, perineural invasion or lymph node involvement. For example, in an uncomplicated primary tumour of a diameter < 2 cm, the NCCN recommends that radiation oncologists might consider prescribing 30 Gy in five fractions over two to three weeks.23 In comparison the NCCN recommends that more aggressive cSCC be treated with more intensive and prolonged RT.
Other comparatively less-supported therapies include chemoradiation,50–52 chemotherapy,6,47,53 cryotherapy21,44 and curettage.11,54 Immunotherapy shows promise, but its role is still evolving and thus, requires larger randomised controlled trials and reviews to demonstrate its efficacy.52,55–57 Logically, sun smart behaviour, such as wearing hats, should accompany any treatment modality.58
Methodology
Study selection
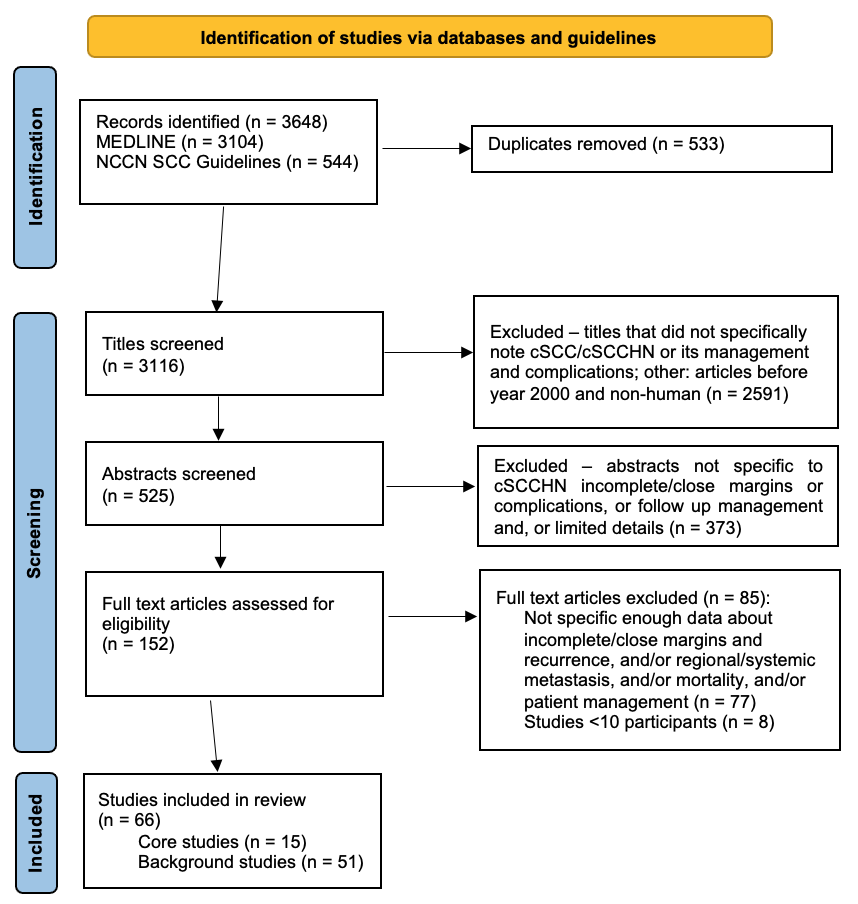
MEDLINE was initially searched with multiple search strategies for articles from 1946 to July 2021 (Figure 1). Inclusion criteria were meta-analyses, systemic reviews, randomised clinical trials, observational studies, case series, pilot studies or journal articles; management of positive or close excision margins; and studies reporting recurrence, survival, adjuvant therapy and clinical follow-up of at least one year. Further, pertinent references underpinning the NCCN Squamous Cell Skin Cancer Guidelines Version 2.2022 were reviewed.23 Exclusion criteria included articles published before 2000 and those with less than 10 cSCCHN patients.

Definitions
Per the literature outlined above, the authors adopted these definitions:
-
Excision margins:
-
positive margin is cSCCHN cells on histopathology or a margin ≤ 1 mm
-
close margin is ≤ 1 mm to < 5 mm
-
close/positive margin is an overlapping description of close and positive margins
-
clear margin is free of cSCCHN on histopathology or > 4 mm.
-
-
Recurrence is regrowth of cSCCHN following an incomplete excision of cSCCHN.
-
Regional or systemic metastasis is cSCCHN extension into regional structures or systemic spread.
-
Mortality is patient death following close/positive margins in cSCCHN.
Results
Article review and inclusion
Overall, 3104 records were screened in MEDLINE (Figure 1 and Supplementary material 1). A further 544 articles underpinning the NCCN guidelines were identified. From both searches, a total of 152 articles were assessed in full text. Of these articles, 15 met the key inclusion criteria. Altogether, 13,671 unique cSCC lesions were identified for inclusion from those 15 studies after the subtraction of otherwise overcounted lesions (Table 1). A further 52 background articles were included which contextualised the core studies.
Patient demographics
The mean age of patients was around 75 and 69.5 per cent of patients were male. Of the 13,671 cSCC lesions identified, 8681 (61.5%) were cSCCHN. Most studies were drawn from predominantly Caucasian populations. The mean follow-up in the 10 core studies was around 51 months. Patient demographics are summarised in Table 2.
Close/positive margins
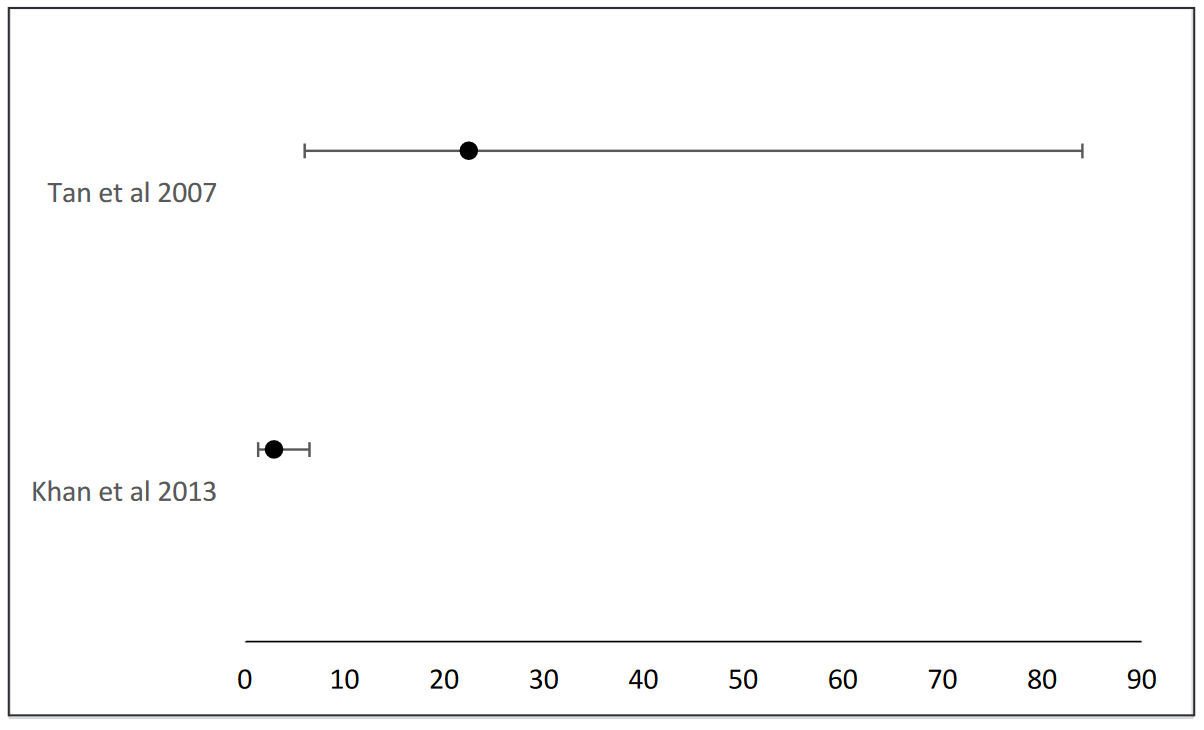
The close/positive excision rate ranged widely from 6.3 to 76 per cent with a pooled average of 17 per cent at 99 per cent CI [15.22, 18.44] (15 studies). The positive excision rate ranged from 4 to 33 per cent with a pooled average of 14.6 per cent at 99 per cent CI [12.97, 16.26] (14 studies). In one study, the rate of positive margins following standard excision was 18 per cent versus 1 per cent for Mohs surgery (van Lee and colleagues).66 The positive excision rate of recurrent lesions was 11.1 per cent (Tan and colleagues)28 and 24 per cent (Khan and colleagues).32 Some further details of rates of initial positive margins vs positive re-excision margins are included in Figure 2.

Positive re-excision risk details drawn from the studies in Figure 2 are:
-
Khan and colleagues32 recorded a 7.6 per cent positive excision rate for cSCC and around a 24 per cent positive re-excision rate for (recurrent) cSCC.
-
Tan and colleagues28 recorded a 6.3 per cent positive excision rate for cSCC and a 60 per cent positive re-excision rate for (recurrent) cSCC.
Anatomical location of margins
The deep margin comprised 73.7 per cent of positive margins at 99 per cent CI [70.85, 76.57] (six studies).32,59–62,64 Of positive margins, 34.5 per cent involved the nose at 99 per cent CI [32.54, 36.52] while 33.14 per cent involved the ear at 99 per cent CI [31.15, 35.13] (seven versus eight studies, respectively).32,54,59–64
Recurrence
Recurrence following close/positive or positive margins varied from 4.2–42 per cent.
The pooled recurrence following close/positive margins was 17 per cent at 99 per cent CI [15.76, 18.16] (10 studies) with a mean follow-up of 51.2 months (eight studies). The pooled recurrence following positive margins was 14.7 per cent at 99 per cent CI [13.51, 15.83] (nine studies) with a mean follow-up of 52.3 months (seven studies).
Recurrence following standard excision versus Mohs surgery was noted in two studies. Genders and colleagues found 5.4 per cent versus 3 per cent (non-significant).33 Van Lee and colleagues found 3 per cent versus zero per cent (non-significant).66
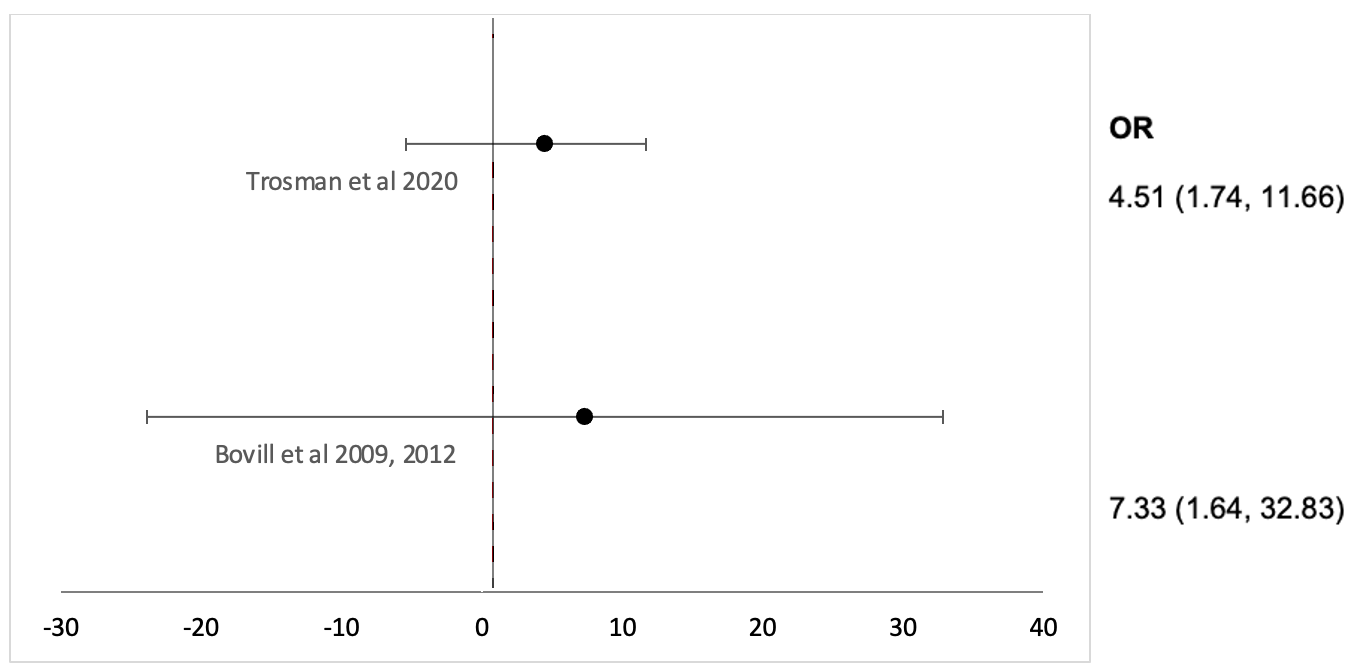
Recurrence after positive re-excision (of margins that were already incompletely excised) varied from 21–62 per cent with a pooled mean of around 35.42 per cent at 99 per cent CI [33, 37.84] (three studies).6,59,60,66 Further details are included in Figure 3.

Recurrence details drawn from the studies in Figure 3 are:
-
Bovill and colleagues59,60 recorded a 5 per cent recurrence following a clear re-excision of an initial positive cSCC excision and a 29 per cent recurrence following a positive re-excision of an initial positive cSCC excision.
-
Trosman and colleagues6 recorded a 26 per cent recurrence following a clear re-excision of an initial positive cSCC excision and a 62 per cent recurrence following a positive re-excision of an initial positive cSCC excision.
Regional or systemic metastasis
Regional orsystemic metastasis following close/positive or positive margins ranged widely from 2.4–100 per cent. The pooled regional or systemic metastasis following close/positive margins was 30.4 per cent at 99 per cent CI [26.15, 34.73] (10 studies) with a mean follow-up of 51 months (seven studies). The pooled regional or systemic metastasis following positive margins was 33.8 per cent at 99 per cent CI [33.77, 33.87] (nine studies) with a mean follow-up of 50 months (six studies). The regional or systemic metastasis for standard excision versus Mohs surgery in one study was 4.5 per cent versus zero per cent (van Lee and colleagues).66
Mortality
Mortality following close/positive margins ranged widely from approximately 10 to 95 per cent with a pooled mean of 46.6 per cent at 99 per cent CI [42.53, 50.65] and a mean follow-up of 60.3 months (four studies).
Follow-up management
All 15 studies recommended surgical re-excision as the gold standard for close/positive margins in cSCC. Overall, seven studies recommended RT as an adjuvant or alternative if re-excision was infeasible.6,28,32,33,44,61,66 Yet, Rahimi and colleagues found previous RT conferred a 2.0 relative risk (RR) of recurrent cSCC.21 They also found no reduced recurrence from adding chemotherapy to radiation. Trosman and colleagues6 estimated two-year disease-free survival (DFS) for patients (but not significant) as 71 per cent for surgery alone; 65 per cent for surgery plus radiotherapy; and 58 per cent for surgery and chemoradiotherapy.
Altogether, two studies cautiously recommended watchful waiting be considered in select frail elderly patients.62,63 Chiller and colleagues found that pre-excisional curettage reduced cSCC locoregional metastasis (from 33% down to 10%) but did not reduce the risk of positive margins.54
Discussion
It is hoped that our up-to-date statistical evidence will help clinicians and patients make better informed choices when faced with close/positive cSCCHN margins. More broadly, we believe that the exponential increase in deadly cSCC requires a greater investment from health departments to arrest this trend.
Patient demographics
This paper reconfirmed that most cSCC patients are elderly, male7 and from predominantly Caucasian populations. Preventatively, health departments should consider expanding public health campaigns to better target young fair-skinned males to reduce the rapidly expanding burden of cSCCs on healthcare and society.
Close/positive margins
Our 14.6 per cent positive excision rate is similar to Genders and colleagues 13 per cent.33 However, their rate was calculated from studies with heterogeneous or missing definitions of positive margins. Similarly, in Rahimi and colleagues, 30.3 per cent of excision margins were ulcerated, which we believe falls under a positive margin.21 Yet, they grouped a further 55.9 per cent of excision margins as ‘chronic sun damage or precancerous changed cells’. Precancerous cSCC cells are on the cSCC spectrum.21 However, chronic sun damage, while cSCC’s pre-eminent risk factor,9,10 is not cancer. Thus, we conservatively estimated their positive excision rate at 30.3 per cent.
Phillips and colleagues recorded a close/positive margin rate of 76 per cent (0–4 mm).65 Perhaps understandably, they wisely refer to the NCCN guidelines to argue for clear margins ≥ 4–6 mm.
In contrast, Tan and colleagues recommended margins ≥ 5 mm as their 2–5 mm cSCC excision margins yielded a positive excision rate of 6.3 per cent for primary lesions (but 9% for young patients), 11.1 per cent for recurrent lesions and a staggering 60 per cent for re-excision of incompletely excised lesions.28 Similarly, Khan and colleagues32 recorded a positive excision rate of 24 per cent for recurrent lesions. Such findings reinforce the need for adequate margins.
Further, most of our positive excisions involved the deep margin, the nose and ear, which broadly aligned with the literature. The above findings reinforce the need for pursuing clear margins, especially in the H-zone.
Recurrence
Following positive or close/positive excisions, we found a pooled recurrence of 14.7 per cent versus 17 per cent, respectively. However, following a positive re-excision, that figure leapt to 35.4 per cent. Further, there was limited non-significant evidence from two of our studies that Mohs surgery might confer some better outcomes than standard excision, which aligned with some literature.23,27 However, there was incomplete detail about the stratification of cSCC tumours and their respective assignment to either standard excision or Mohs surgery. There was also heterogeneous detail about follow-up and comparative histopathology technique. Therefore, further research could better delineate the efficacy of these surgical techniques as well as tumour and patient selection, standard excision histopathology versus Mohs histopathology reliability, and patient follow-up.
Regional or systemic metastasis
The pooled rate of regional or systemic metastasis following positive versus close/positive margins was 33.8 per cent and 30.4 per cent respectively. These very high rates seem to be best explained by our heterogeneous data. For instance, Rahimi and colleagues recorded a close/positive excision rate of at least 30.3 per cent, but possibly ≥ 80 per cent with an astounding 100 per cent locoregional metastasis of all patients (including clear margins).21 They attribute their high rates to specialising in complex and invasive cSCCHN, which would intuitively confer a higher risk.23
In contrast, Dallari and colleagues’ pilot study (follow-up approximately 24 months) recorded only a 10 per cent metastasis rate after 10 positive excisions and no metastases following six close excisions.62 However, nine out of 10 positive excisions were re-excised with a considerably shorter follow-up than Rahimi and colleagues21 (> five years), which might mask otherwise increased rates of metastasis.
Again, when differentiated between standard excision and Mohs surgery, van Lee and colleagues (follow up 63.7 months) found a regional or systemic metastasis rate after positive excision of 4.5 per cent versus zero per cent respectively.66 However, this evidence is weak and non-significant given that the zero per cent finding for Mohs surgery was drawn from only three cSCCs that were completely re-excised.
Due to heterogenous data, we grouped regional and systemic metastasis together. Further research might elicit more differences between these categories and related complicated cSCCHN and interventions.
Mortality
Pooled mortality (46.6%) following close/positive margins in cSCCHN is only explored in part by four core articles. For instance, Brinkman and colleagues found a significant 4.0 RR for positive versus clear margins.44 While, Phillips and colleagues recorded a 31.2 per cent mortality rate following 59–76 per cent close/positive margins.65 These findings might suggest that positive margins confer an increased burden of mortality. However, none of our core studies adequately detail the contribution of patient comorbidities and old age, which intuitively clouds cSCC’s precise role in mortality. Indeed, Brinkman and colleagues44 conceded that their patients also died of other unstated causes. This paucity of data is reflected in the literature. Therefore, further mortality research is required.
Follow-up management
Our review reconfirmed that surgical re-excision with adequate margins remains the gold standard for managing close/positive margins in cSCCHN. Likewise, surgical excision with adequate margins is also the gold standard when dealing with an initial presentation of cSCCHN. In either case, the importance of adequate margins cannot be overstated, because of the increased rates of further positive re-excision, recurrence, regional or systemic metastasis, and mortality. This is especially critical when dealing with the deep margin, the nose and ear, which are especially at risk of being found positive. Therefore, we reiterate the wisdom of the NCCN guidelines to pursue clear margins of at least ≥ 4 mm for both initial surgery as well as positive margins.
Further, we found some very limited non-significant evidence in two of our studies that Mohs surgery might be associated with lower rates of complicated cSCCHN. However, as noted earlier, due to incomplete data, further research is needed to better delineate its efficacy versus standard excision. There was also limited evidence in only one older study that pre-excisional curettage may help reduce locoregional metastasis.66
Second to surgery, seven studies recommended RT, which should be considered for adjuvant therapy following re-excision or for those unfit for further surgery. However, Trosman and colleagues estimated two-year disease-free survival for surgery alone was better than when RT was added.6 On the other hand, Rahimi and colleagues found that previous RT conferred a twofold risk of cSCC recurrence.21 Alternatively, it may be that patients with higher risk cSCCHN tend to be selected for RT. Such mixed data supports careful multidisciplinary review when preferencing RT.
Like other studies, this study found that both chemoradiotherapy and chemotherapy were less efficacious than re-excision and RT.
Further, none of our core studies examined immunotherapy specifically. However, our initial literature search yielded some hopeful results. Indeed, in Ferrarotto and colleagues, 20 cSCCHN patients received two cycles of neoadjuvant PD-1 inhibition,56 a less morbid modality than re-excision and RT. At 22.6-month follow up, two patients (10%) had recurrence. While such results appear promising, larger immunotherapy trials and reviews are needed in order to facilitate consensus as to its utility.52,55–57
Limitations
Only 61.5 per cent of cSCC lesions were cSCCHN. Our studies were markedly heterogeneous, as reflected in a very wide variation in recurrence and regional or systemic metastasis following close/positive margins. Yet, we were unable to adequately determine disease specific mortality as mechanisms of death were usually not stated.
Conclusion
This review highlights the need for a standardised definition of positive margins, which are associated with worsened risks of positive re-excision, recurrence and regional or distant metastases. However, disease specific mortality could not be adequately determined. When faced with positive margins in cSCCHN, we recommend re-excision, which remains the gold standard. If surgery is not feasible, we recommend RT. Watchful waiting may be acceptable for select frail or palliative patients.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.
Revised: February 13, 2023 AEST; April 28, 2023 AEST; July 24, 2023 AEST