


Introduction
Like no other surgical specialty, plastic surgeons plan much of their surgery by drawing on the skin. A breast surgeon might mark out the incision required for a mastectomy, or an orthopaedic surgeon might intraoperatively ‘site mark’ the position of a screw, but these are a very different exercise to a comprehensive plastic surgical ‘marking up’. Plastic surgical marking up is a cognitively intense process requiring detailed knowledge of anatomy, the forces of tension in the skin, the behaviour of skin once cut and aesthetic expectations. Few outside of plastic surgery understand this, and many misunderstand that marking up differs significantly from site marking. Because of this misconception, providers of the tools for marking up fail to understand why a disposable plastic marking pen is suboptimal. Such pens vary in calibre, weight and quality and consistently fail due to drying up. The interruptions and frustration of having a marking pen fail at the exact time when the surgeon’s focus should be on planning a complex operation are not optimal for patient care or the mental focus of the surgeon. Sommerlad pens and Bonney’s blue ink allow for a consistent weight of the pen in hand, a reliable source of ink, and an ability to vary the thickness of the line drawn by the screw-down nib system.
Gillies commented that the drawing of the flap outline is the first incision.1 Another important use of the surgical marking pen was demonstrated by Strombeck, of breast reduction fame, at the 1971 International Plastic Surgical Meeting.2 He located the definitive point of the nipple with the tip of his middle finger in the inframammary groove, which was the final point of its definitive location. He then used a permanent marker to locate this point on the skin, indicating the site of the areolae reconstruction. Hence, the value of permanent marking with the patient suitably draped, awake in the anaesthetic room and sitting upright.
Other professionals are particular about their drawing tools. We would not expect an architect to be able to substitute their specialist pen with a child’s colouring pencil and still deliver the same quality of plans for a house.
History of surgical inks and the Sommerlad pen
The practice of marking the body with ink for plastic surgery was first described in 1460 by Heinrich von Pfolspeundt, a German surgeon who recorded the details of a rhinoplastic procedure performed by Antonio Branca, an Italian surgeon. He described planning the incisions for an upper arm pedicled flap using ink painted around a leather or parchment template of a nasal defect. This was again described in 1597 by Tagliacozzi, who used ink to mark the incision lines.3
It was not until almost 200 years later in 1794 when an unsigned letter was published in The Gentlemen’s Magazine that surgical ink was mentioned again. This time, it was used to draw a forehead flap using a wax template in the shape of the nasal defect. Numerous compounds were used for surgical marking during this period; ink, tincture of iodine and silver nitrate have all been mentioned.3
The first commercial aniline dye was synthesised in 1856, and soon after, hundreds of synthetic aniline dyes were developed, but three became common skin-marking inks: gentian violet (1861), methylene blue (1876) and brilliant green (1877).3 British gynaecologist Victor Bonney developed ‘violet green antiseptic’ originally as a vaginal prep solution in 1915. It later became known as ‘Bonney’s blue’ and was a popular surgical skin-marking ink in the 1930s.4
The Sommerlad pen was devised for drawing on the mucosa of the lip for cleft lip and palate repair and has gone through different versions. Sommerlad originally co-developed it with an instrument technician at the London Hospital in the 1970s while working as a registrar. It was first made by Downs Surgical, however, the manufacturing quality was variable, the main problem being the production of a tip fine enough for use in marking a delicate procedure such as a cleft lip repair. Subsequent iterations of the Sommerlad pen improved the tip and added protective mechanisms.
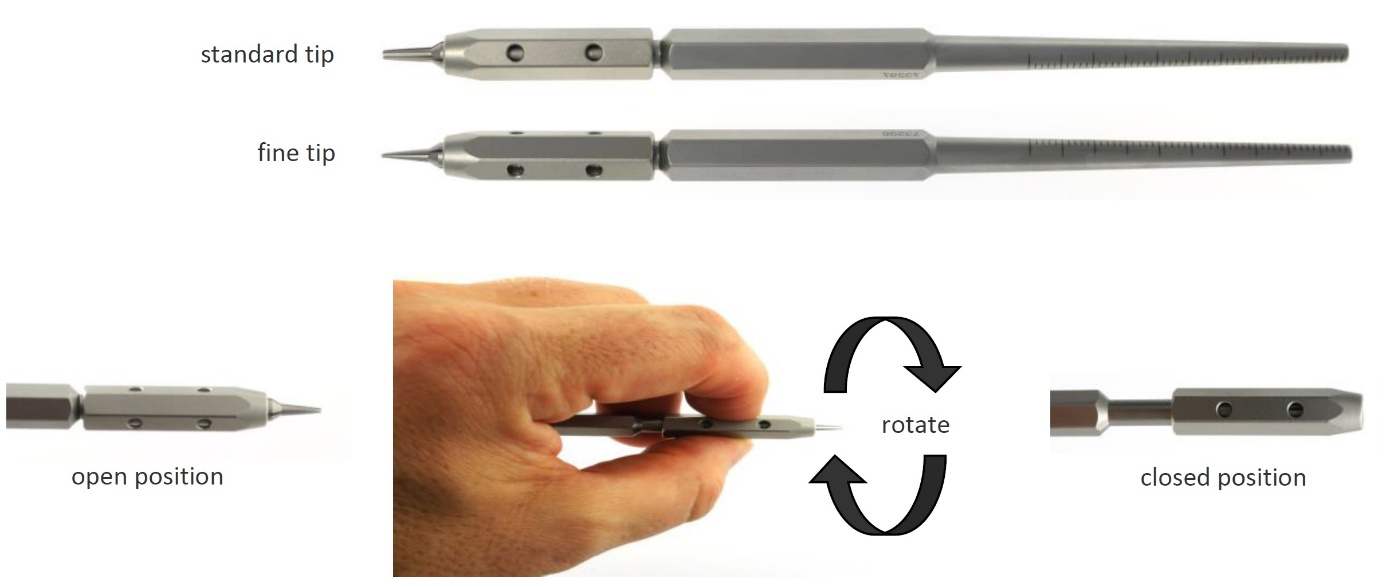
The second generation was produced by Dixons Surgical Instruments Ltd (Figures 1 and 2). In the latest and third-generation design the tip can be protected, if the surgeon remembers to do so, which is a big improvement. The fine version (marketed by S Murray and Co) is the best for drawing precise lines, but the tip remains easily damaged (Figure 3). The evolution of the Sommerlad pen continues; the next generation in development has been designed with a titanium tip.
.jpeg)
.jpeg)

Formulation and safety of surgical inks
The original composition of Bonney’s blue ink is brilliant green (0.5%), gentian violet (0.5%), 95% ethyl alcohol (50%), and water (49%).4 Gentian violet is a dye derived from aniline, which belongs to a chemical class known as di- and triaminophenylmethanes. It is a mixture of crystal violet (crystalline hexamethyl-pararosaniline) and methyl violet (tetramethyl and pentamethyl-pararosaniline). Medical-grade gentian violet contains at least 96 per cent crystal violet.5
There has been a suspicion that gentian violet is a carcinogen. It has antibacterial and antifungal properties and was previously used in treating cutaneous and mucocutaneous candidiasis, and even as an additive in blood products to prevent transfusion-associated Chagas disease.6,7
Chagas disease is caused by the parasite Trypanosoma cruzi, which is transmitted to animals and people by insect vectors and is found only in the Americas. The second most common route of infection is through allogenic blood transfusions in countries where it is endemic. Gentian violet is a trypanomicidal substance and can be added to the blood to aid in the prevention of transfusion-associated Chagas disease.8
The use of gentian violet as a treatment of choice in various dermatological conditions has declined significantly over the past decades due to the availability of alternative antifungal agents and in-vitro mammalian cell studies suggesting that gentian violet has carcinogenic properties.9,10 Two published studies on animal models (rodents) demonstrate potential carcinogenicity. Both studies administered gentian violet in the rodents’ diet at high doses (100, 300 and 600 parts per million), which demonstrated an increase in hepatocellular adenoma, hepatocellular carcinoma, type-A reticulum sarcoma of the urogenital system, Harderian gland adenoma and thyroid follicular cell adenocarcinoma.11,12
Evidence to support the carcinogenic potential of gentian violet in humans is sparse. There are two publications describing the use of gentian violet and cancer, one via blood transfusion and the second a case report of an accidental stabbing with an ink pen. Evidence is lacking and not mentioned in the International Agency for Research on Cancer’s 2022 report.13 A Canadian environmental assessment report on the evidence for the carcinogenicity of gentian violet provided a translation of two publications describing gentian violet and cancer.14,15 The first publication is a retrospective study conducted in a hospital in Brazil, that found 26 out of 37 patients who received blood transfusion treated with gentian violet to prevent Chagas disease had benign or malignant neoplastic lesions. Patients were asked if they recalled receiving a blood transfusion that appeared purple, and there was no mention of confirmation with a blood bank. The location and type of neoplastic lesions were not described. This study had several limitations, including a lack of control subjects and several confounding factors.
The second publication is a German case report describing a 57-year-old man who accidentally stabbed his right hand with an ink pen containing an unknown concentration of methyl violet, an ingredient of gentian violet. He developed lymphocytic leukaemia five months after the incident. There was no mention of the patient’s prior blood count before the incident or the extent of exposure to the gentian violet.
Gentian violet was classified in 2021 by the International Agency for Research on Cancer as a Group 2B ‘possibly carcinogenic to humans’.13 The stream of evidence ranged from Group 1 as carcinogenic to humans, Group 2A as probably carcinogenic to humans and Group 3 as not classifiable.14 Cases of toxicity in humans remain limited to a small number of case reports of mucosal complications as a result of direct local application or intravesical instillation only.16–23 Several studies investigating the use of gentian violet in dermatological conditions have demonstrated its potential use as a topical agent on the skin with no significant complications.24–28 No adverse reactions to the use of gentian violet as a surgical ink have ever been described. It should be noted that the ink in a typical plastic marker pen contains polyvinyl pyrrolidone, glyceride, methylene blue or crystal violet, which would also fail tests of carcinogenicity in animals in high doses.
Manufacture of Bonney’s blue
It has been increasingly difficult to source Bonney’s blue solution due to concerns about gentian violet being carcinogenic in animal studies.11,12 Gentian violet and brilliant green, the raw ingredients required to manufacture Bonney’s blue solution, are available in powder form. To reconstitute the solution, the powders are dissolved in either distilled water and/or alcohol 96%.
Exposure from the aerosolisation of the powders may present an occupational health and safety risk to pharmacy staff. Despite measures taken to mitigate this risk with personal protective equipment such as a face mask, protective eyewear, gloves and gown, there is a reluctance to prepare this product in hospital pharmacies with manufacturing facilities due to the unknown effects of exposure to humans. There is also no data available on the occupational exposure of gentian violet via dermal contact or inhalation. The advantage of hospital pharmacy manufacture of Bonney’s blue is that the final product can be autoclave sterilised, making it suitable as a surgical marker compared to commercially available ink solutions that are usually non-sterile.
In the commercial market, gentian violet remains the most common ink in many disposable surgical marking pens. Although the ingredients in the pens are often not included on the pen or packaging, safety data sheets for the products are available for surgeons to review. Surgeons should seek gentian violet-free formulations of these pens if they want to avoid its use.29
In Australia, Bonney’s blue solution is currently unavailable as a proprietary product and has to be sourced overseas through suppliers specialising in importing unregistered medicine products. There are proprietary products of Bonney’s blue solution overseas (Delasco, United States and Tayside Pharmaceuticals, Scotland). Consideration via the Special Access Scheme to access unregistered medical goods from overseas has to meet specific criteria required by the Therapeutic Goods Administration in Australia.30 When seeking unregistered products from overseas, it is important to obtain information regarding the formulation and if the product is manufactured in a facility that meets international Good Manufacturing Practice standards.
Environmental considerations
Disposable plastic marking pens are not usually made from recycled plastic. They are rarely recyclable due to contamination with biological material and an internal felt core. They, therefore, become another part of the medical waste landfill.
How can we retain surgical inks with 21st century health and safety rules?
It is essential in the surgical setting that we adhere to using published and described ink formulas. Proprietary formulations lack standardisation, and the compounds used are not always disclosed to the surgeon. If a surgeon is equipped with the knowledge of the ink and its components, then they can use it safely on patients. For example, a surgeon would avoid using inks containing gentian violet on conjunctivae due to mucosal toxicity and avoid using brilliant green as an injectable due to its highly pro-inflammatory nature.
There is no lack of choice with so many different surgical markers available in the market. Commonly available felt-tipped pens are often unable to draw the precise lines required for procedures requiring a high degree of accuracy, particularly plastic surgery procedures. Plastic surgeons need access to reliable ink to follow our markings while performing such precise surgery (Figure 4). A surgeon needs to be focused on the tissues and anatomy rather than the need to constantly re-mark fading lines intraoperatively.

The concerning preliminary findings of in-vitro and animal models are a valuable addition to our knowledge about these compounds. However, overextrapolating and restricting their use on humans as a topical skin marker only removes an essential component of a plastic surgeon’s armamentarium.
Acknowledgements
The authors would like to acknowledge Cameron Phillips who provided feedback on the preparation of the manuscript.
Patient consent
Patients have given informed consent to the publication of images and/or data.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest
The authors have no personal conflicts of interest to disclose. S Murray and Co has provided donations to the charity CLEFT – Bridging the Gap. Brian Sommerlad is the chairman of CLEFT, a charity which funds research into cleft lip and palate and supports cleft teams in low-resource countries.
Revised: May 22, 2023 AEST
Updated: September 24, 2024; dates of submission and acceptance corrected