Introduction
This case report presents a challenging clinical scenario of head-neck reconstruction, which involved two separate craniectomy defects secondary to osteoradionecrosis, one of which had a metal prosthesis reconstruction. The initial microvascular flap was compromised by distal necrosis and a novel method of reconstruction was used to salvage the partially necrotic flap in this situation.
Case
A 65-year-old man was referred to the head and neck clinic of our tertiary hospital with a large non-healing left-sided temporoparietal ulcer, with radionecrotic bone at its base. There was no evidence of underlying osteomyelitis. He had previously undergone a wide local excision of a T4a squamous cell carcinoma of his left conchal bowl with local flap reconstruction, approximately 18 months earlier. He then underwent adjuvant radiotherapy to the area. He has had multiple non-melanoma skin cancers excised from his head and neck. He also suffered from radiation-induced temporal lobe cerebritis which resulted in seizures; this was well-controlled with medication. The patient was otherwise in reasonable health.
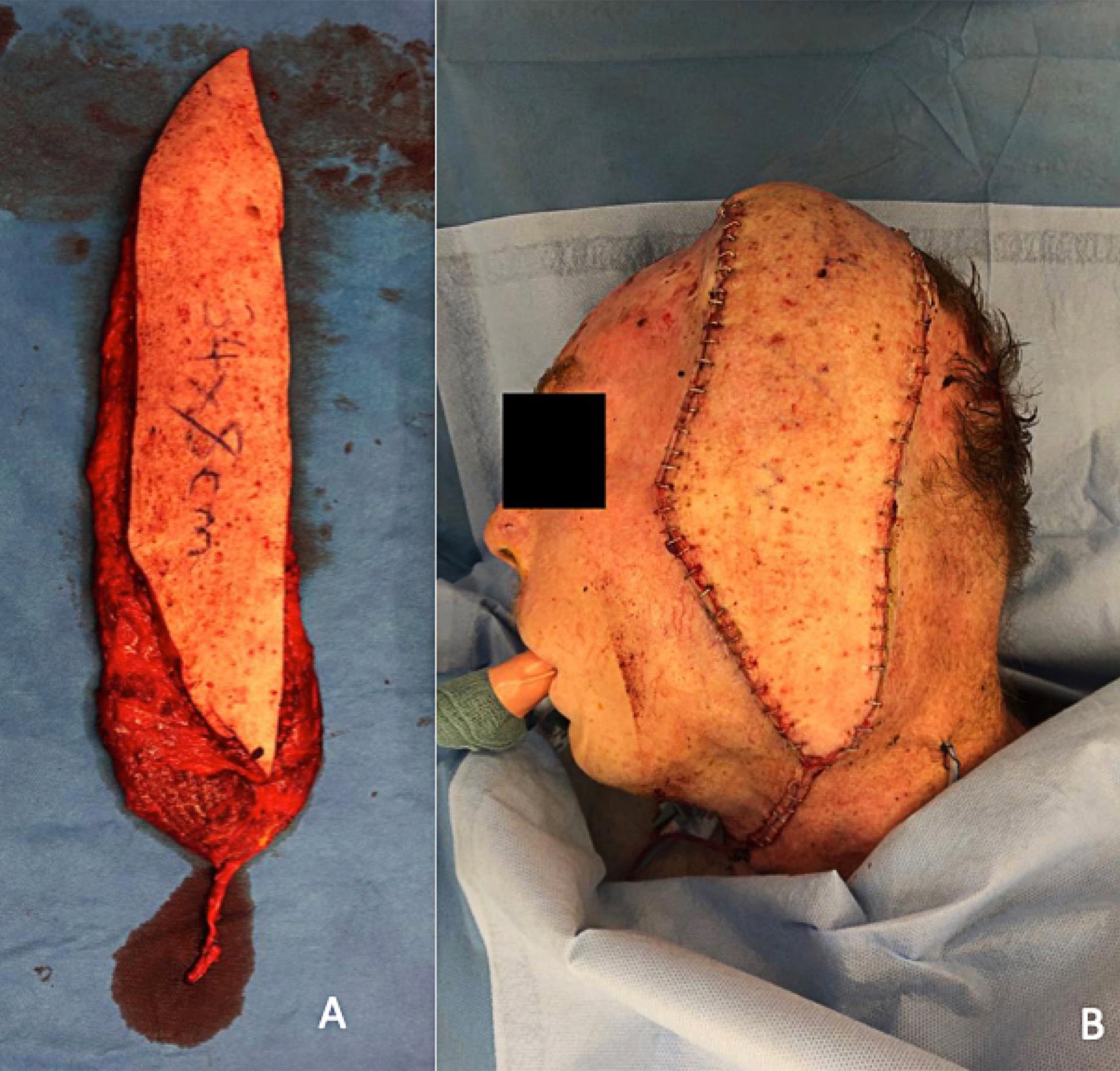
The recommendation of the multidisciplinary head and neck clinic was for surgical excision of this ulcer with free flap reconstruction, which he underwent in early 2019. The excision was performed by the otolaryngology head and neck surgical team. Within the primary soft tissue defect, there were two separate craniectomies performed by the neurosurgical team to remove the radionecrotic bone. The first was at the scalp vertex overlying the superior sagittal sinus. The second was in the temporal region and this site was covered with a titanium mesh plate. The plastic and reconstructive surgical team, led by the senior author (DG), then chose to reconstruct the entire defect with an ipsilateral free musculocutaneous latissimus dorsi (LD) flap measuring 34 cm × 9 cm (skin paddle). Deliberately, muscle was harvested at least 1 cm wider than the skin paddle, inclusive of lateral border of the muscle, along the entire length of the relatively long and narrow flap (Figure 1A). The flap vessels were anastomosed end-to-end onto the facial artery and end-to-side internal jugular vein, within the previously irradiated field. The ischaemic time of the flap was 79 minutes. At the time of closure, the distal triangular end of the flap was trimmed to suit the inset of the flap (Figure 1B). Dermal bleeding observed at the distal edge of the flap was suggestive of good perfusion. There were no intraoperative concerns from, or complications by, any of the teams involved.
_latissimus_dorsi_musculocutaneous_flap__harvested._note_that_muscle_is_included_in_almost.jpeg)
After a successful extubation and uneventful 24 hours in the intensive care unit, the patient returned to the surgical ward and remained under close observation. The flap was monitored hourly for the first 24 hours, every two hours for the following 24 hours, and so on to a maximum of four-hourly flap observations.
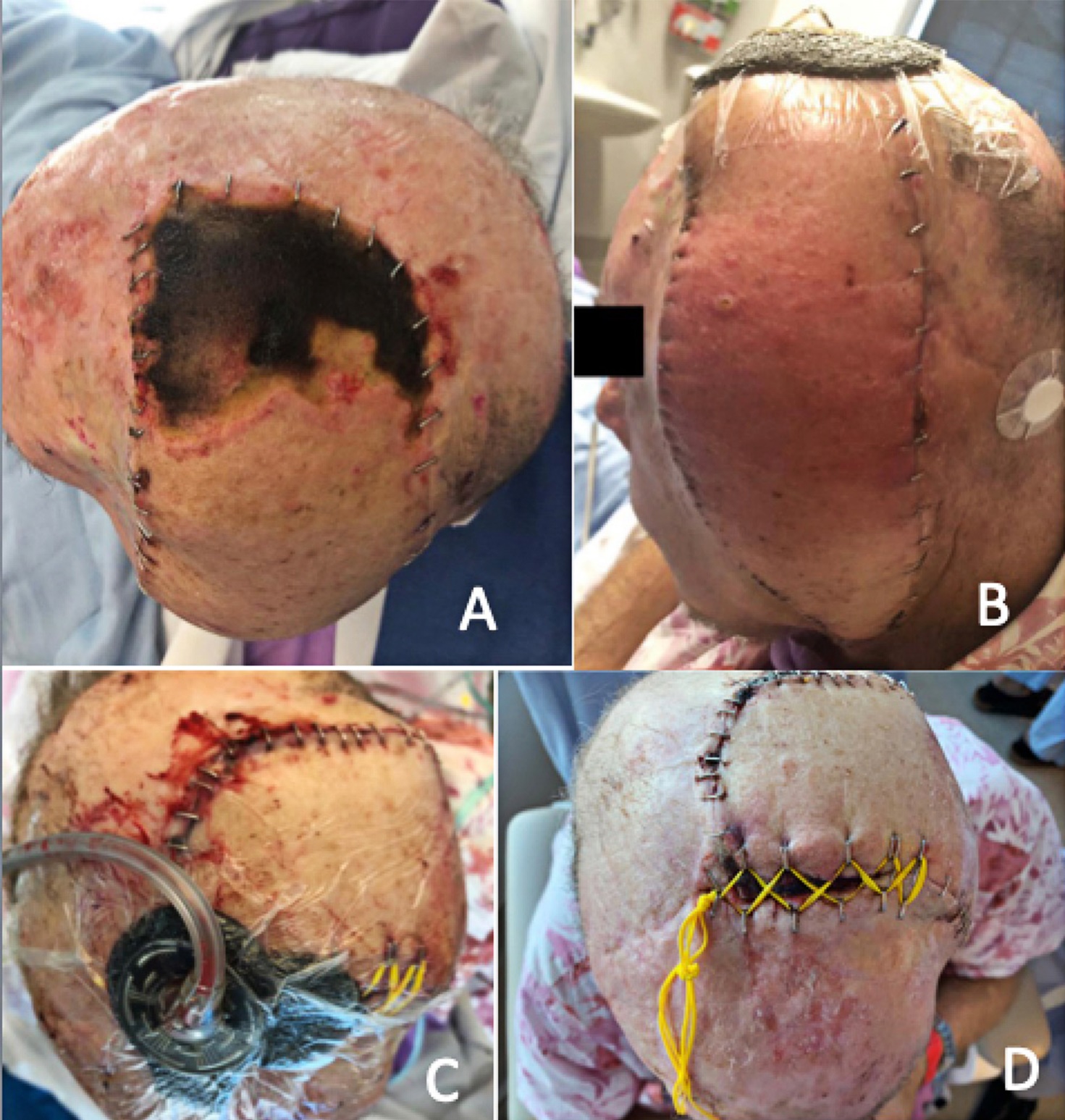
Despite the normal flap appearance of the majority of the flap, and a consistently strong audible pulse using Doppler ultrasound throughout the first postoperative week, the distal portion of the flap gradually became ischaemic (Figure 2A). This posed a significant reconstructive problem that needed an urgent solution. The decision was made to insert a tissue expander (TE) under the flap. Under general anaesthesia, a 250 mL rectangular TE with a remote port was inserted 21 days after the initial free flap surgery. The TE was placed via the anterior inset of the flap under the muscle, directly overlying the titanium mesh reconstruction of the temporal defect, several centimetres away from the ischaemic area of the flap. A thorough lavage of the sub-flap space was performed prior to insertion of the TE. The remote port for inflation was placed under the posterior intact scalp skin. The necrotic portion of the distal flap was not debrided at this stage as the necrosis was dry and there were no signs of local or systemic infection. The donor site of the LD flap healed without any event.
_day_21__prior_to_insertion_of_the_tissue_expander__showing_distal_stable_necrosis_of_the_.jpeg)
Given the high risk of meningitis with the proximity of the necrotic tissue to dura and cerebrospinal fluid, the saline expander was inflated rapidly at 10 mL per day for a week, over and above the base volume of 50 mL. After the first week, 10 mL of saline was used twice a day, for further inflation, for the next few days. The expansion rate was carefully tailored to the assessment of the flap during and after each expansion. Our goal was to achieve adequate expansion as quickly as possible as tolerated by the flap. A total of 220 mL was injected into the expander over a 12-day period. On day 13 postoperatively, the flap over the TE became erythematous (Figure 2B), and so the patient was taken back to theatre for the removal of the expander. During this procedure, the necrotic tissue (measuring 10 cm × 10 cm at that stage) was also debrided, and the free flap was advanced up towards the scalp vertex.
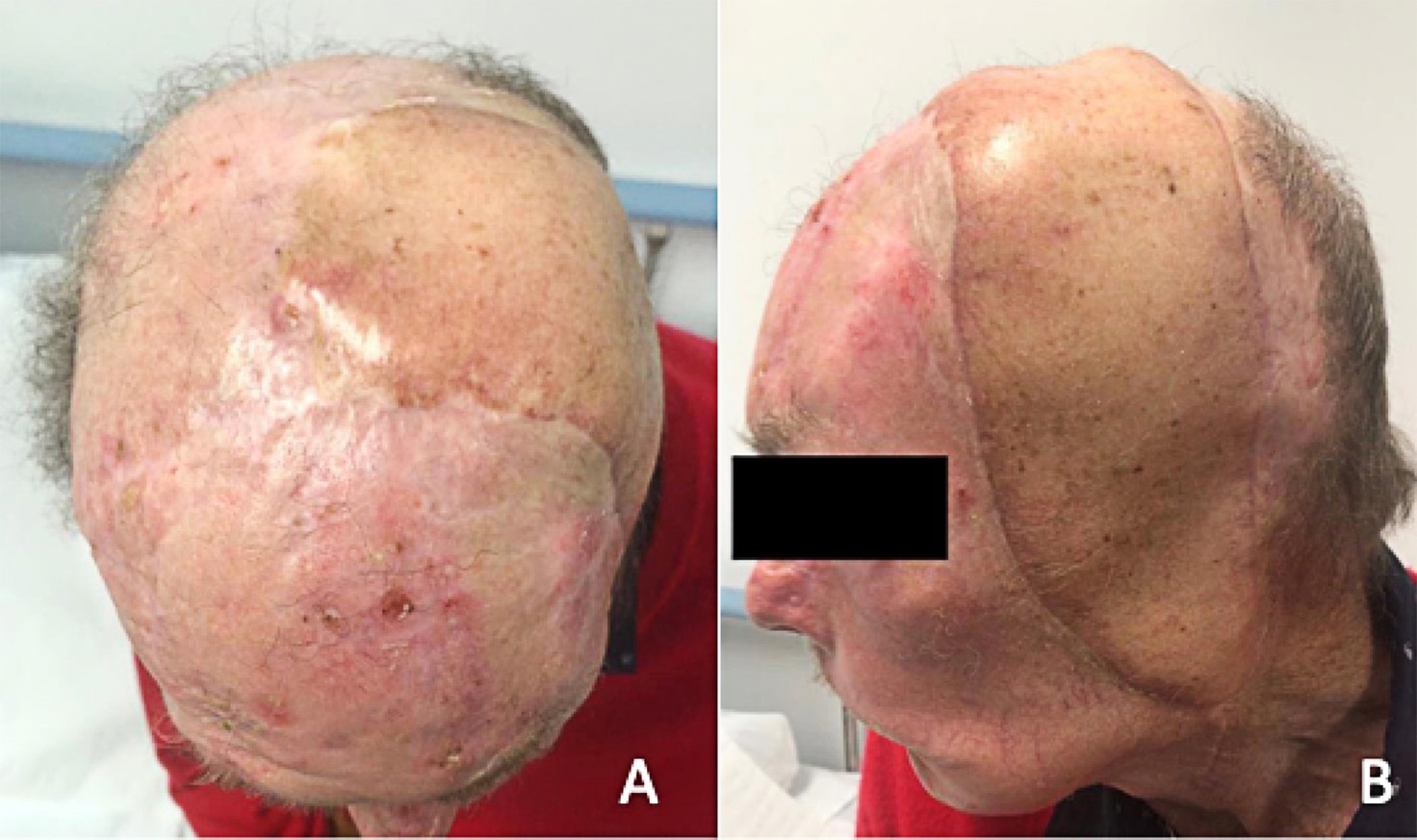
The distal skin edge of the flap did not appose the native skin at the scalp vertex without undue tension. Hence, ‘bootlaced’ suture vessel loops were used to approximate the edges and a closed negative pressure (VAC) dressing was applied (Figure 2C). The patient was discharged home at day 43 following the initial surgery. The bootlace suture straps were sequentially tightened weekly and eventually removed when the skin was able to be sutured closed under local anaesthetic (Figure 2D). The patient was reviewed in the outpatient clinic for follow up at four months after the original surgery (three months after secondary closure of final defect) and stable coverage of his scalp defects was observed (Figures 3A and 3B).
_top_view__four_months_after_the_original_surgery_(three_months_after_secondary_closure_of.jpeg)
Discussion
Pre-expansion of pedicled and free flaps before tissue transfer is well described in the literature. Indications for this include thinning of the flap, increasing its size or facilitating closure of the donor site.1–3 In our case, pre-expansion of the LD flap was not considered feasible because of the relative urgency. It was also not considered necessary as the estimated size of the defect, although long and narrow, was well within the described vascular territory of the LD flap.4,5 Exact planning of the reconstruction with free LD flap was not possible preoperatively as the resection teams were ear nose and throat and neurosurgical. Since, at the time, distal margin of flap after trimming of the tip of the flap showed good perfusion at the edge, no primary vein grafts were considered necessary for elongation of the pedicle.
It is our speculation that the normal post-surgical oedema of the flap caused progressive necrosis of the distal part that was contributed to by the unyielding nature of the underlying cranial bone and titanium mesh. Directly under the necrotic portion of the flap lay the dural layer and the superior sagittal sinus, and so debridement and grafting were unsuitable. The dermal substitutes, such as NovoSorb (PolyNovo Ltd, Port Melbourne, Australia) or Integra Dermal Regeneration Template (Life Sciences Corp, Plainsboro, USA), were considered but, due to the scarred and irradiated bony rim, their ‘take’ was not considered predictable. The local flap options were also unavailable. Since a substantial portion of LD flap was still well perfused, a second free flap option was not considered at this stage and was regarded as a backup option. Re-elevation and advancement of the surviving LD flap was not a practical option as it would have been inadequate to cover the entire defect. Detaching the surviving flap and lengthening the pedicle with vein grafts was not considered safe because of previous extensive scarring and radiation in the neck area.
The published literature suggests that the use of TEs following transplantation is less common. Fan reports the use of a tissue expander to debulk and further reconstruct a free LD flap on the face, 10 months after transplantation.6 Baumeister and colleagues describe a series of three free flaps and one pedicled flap expanded after transplantation, the earliest of which was expanded 4.5 months after the initial transfer.7 As yet, no published reports have described the use of tissue expansion of a free flap in the acute phase following initial tissue transfer. Since the TE in our patient had to be removed before its full expansion, it was not possible to close the defect primarily with re-inset of expanded flap. In this difficult situation with sagittal sinus under the distal edge of flap, a centuries old principle of a slow, sustained TE was used with the bootlace suture technique. This technique is commonly used by other specialties, such as orthopaedic surgery and general surgery, in managing difficult wound closures.8 This area of bootlace suturing was effectively covered with a completely closed VAC dressing to prevent infection.
It is an informal policy of our unit to discuss all major complications with at least one (or more) consultant team member before any major revision surgery or second-shot reconstructions. Our first concern was identifying the problem and preventing such a complication in the future. Under similar circumstances, we would consider loose approximation of flaps over convex bony defects (with primary bootlace suturing of the skin, if necessary), to make allowance for a flap oedema during the first postoperative week.
Following the partial necrosis of the LD flap, we discussed various options and decided that early rapid TE had the lowest risk of major anaesthetic or surgical complications, and possibly the best chance of success, despite the fact that this has not been attempted previously. The most likely risk was a local infection and in our view this was adequately mitigated by the use of a sealed dressing, prophylactic antibiotics and closely supervised management of this inpatient. Because of the successful outcome of this case, we certainly feel confident to use this option again if faced with a similar scenario, if better options were unavailable.
Conclusion
Although this case presents a unique scenario, we believe that the option of early rapid TE can be a useful adjunct in our armamentarium as plastic surgeons. Several parameters need to be favourable for this procedure. These include the availability of an adequate size of unaffected flap for expansion, pliability of the flap deemed for expansion, absence of infection, expected gain in the flap from the TE and clinical judgement for adequacy of expansion for reconstructive need, supervised environment, and backup plan if the TE fails to achieve reconstruction goals.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.
Revised: May 27, 2023 AEST