

Introduction
The forehead flap is a widely used pedicled flap for nasal, periorbital and forehead reconstruction. It was first described by the Indian physician Sushruta in 500 BCE,1 making it one of the oldest surgical procedures still in use today. It is routinely performed as a staged procedure with initial elevation and inset of the flap and subsequent division of the pedicle representing at least two of these stages. This case presents a variation of the standard staged method of the paramedian forehead flap reconstruction. It uses a double opposing forehead flap in a single-stage reconstruction of a contralateral eyebrow and upper eyelid defect to minimise the need for a second stage of surgery and to hasten the patient’s progression to adjuvant radiotherapy.
Case
A 62-year-old male without significant medical history was referred from a regional centre to a metropolitan tertiary hospital with a biopsy-proven, poorly differentiated squamous cell carcinoma (SCC) of his left eyebrow (Figure 1). The patient smokes 15 cigarettes a day in addition to daily cannabis use.
On examination there was a 5 × 5 cm ulcerated lesion overlying the left eyebrow at the superior border of the orbital rim. It was not fixed to underlying structures and there was no clinical locoregional lymphadenopathy. Despite close proximity of the tumour to the supraorbital nerve, there was no altered sensation over the scalp in the distribution of the supraorbital or supratrochlear nerves.

Preoperative magnetic resonance imaging showed no evidence of perineural invasion. Further radiological staging with head and neck computed tomography did not demonstrate tumour invasion of the frontal bone or its periosteum. Positron emission tomography demonstrated no distant sites of metastasis. The case was discussed at a multidisciplinary meeting and a consensus was reached regarding surgical management.
Surgery
The patient underwent a wide local excision with a 1 cm clinical margin. The lesion was excised with underlying periosteum down to the frontal bone and included upper eyelid skin as part of the inferior margin. The supraorbital nerve was removed en bloc with the tumour as it travelled through the tumour mass. An osteotomy of the supraorbital foramen was undertaken to permit a proximal biopsy of the nerve to test for proximal perineural invasion. Margins of the excision also included the ipsilateral supraorbital vessels. The specimen was oriented with a marking suture and sent for histopathological examination in formaldehyde.
Defect
After excision, the residual defect included a large area of exposed frontal bone including the whole superior orbital rim and upper eyelid soft tissue with the tarsus intact.
Reconstruction
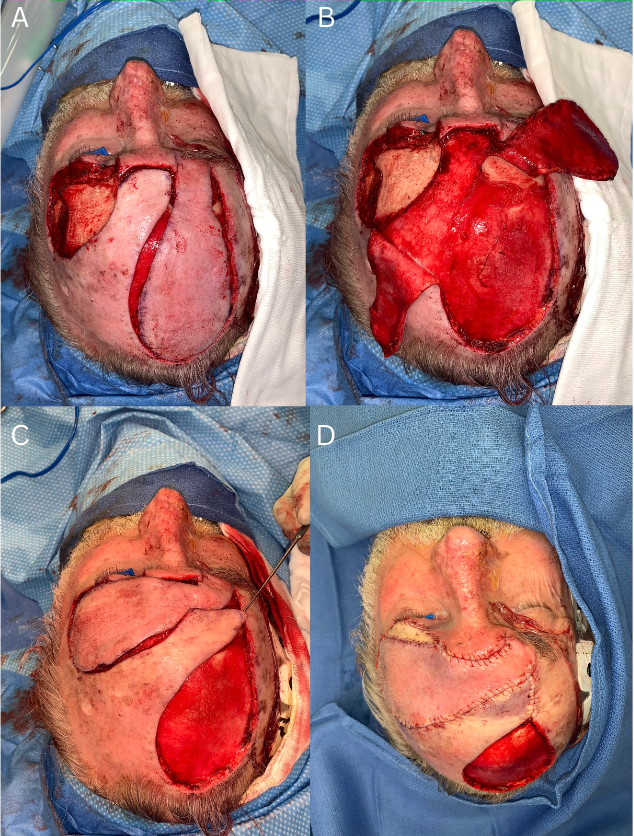
A double opposing forehead flap was raised in the following fashion (Figure 2). A pedicled contralateral forehead flap was raised incorporating hairless scalp with the paddle dissected in the subcutaneous plane at the cranial third, the submuscular plane in the middle third and the subperiosteal plane in the caudal third. There was a 3 cm skin bridge overlying the glabella that was elevated as a superiorly-based, random-pattern scalp flap to allow for single-stage transposition of the forehead flap pedicle and to cover the subperiosteal dissection. The remaining cranial two-thirds of the forehead flap donor site were dressed and allowed to heal by secondary intention following agreement of this approach with the patient preoperatively. A preauricular full thickness skin graft was inset to reconstruct the upper eyelid, following an aesthetic subunit reconstructive approach.

Postoperative course
The patient was admitted to the ward for one night and discharged the following day without incident. Histopathological examination revealed a 10 mm thick, 38 × 34 mm poorly differentiated SCC without perineural, lymphovascular or skeletal muscle invasion. The deep margin was 1.8 mm clear and the radial margins were greater than 5 mm clear. The supraorbital nerve specimen did not show evidence of malignancy.
Postoperative radiotherapy 50 Gy in 25 fractions was administered without complication and the patient was reviewed in the outpatient clinic following completion of his radiotherapy (Figure 3).
A small area of the donor site required a skin graft performed in a secondary procedure. As this was distant to the site of the lesion, it did not affect the patient’s progression to adjuvant radiotherapy.

Discussion
Plastic surgery is a principles-based surgical discipline that does not mandate adherence to predetermined operative ‘recipes’ but rather requires the broad application of reconstructive principles to any surgical defect encountered. The forehead flap is versatile and has a reliable blood supply.2 Its use as a transposition flap to reconstruct intermediate-sized eyebrow and forehead defects has not readily been described in published literature. Tripathy and colleagues described a similar single-stage operation using an islanded forehead flap to reconstruct a glabella and medial eyebrow electrical burn defect.3
In our case, the residual oncological defect was likely to require postoperative radiotherapy and would need robust, vascularised tissue that would be able to withstand the rigours of radiotherapy. The decision to reconstruct this defect with a regional flap in favour of free tissue transfer upholds the reconstructive principle of replacing ‘like with like’.4 The colour and contour match using adjacent tissue is far superior. This flap reconstructs the majority of the defect in accordance with this principle, excluding the two specialised areas within the defect of the eyelid and hair-bearing eyebrow.
In this case, the suitably-sized skin paddle of the contralateral forehead flap was transposed 90 degrees across the midline. This transposition provided a satisfactory aesthetic result with a single-stage procedure. The design of the flap permitted the pedicle to be laid flat on the frontal bone from its origin to the recipient site. This design, when combined with a secondary local flap to facilitate donor site closure, is what permitted this forehead flap reconstruction to occur in a single stage and enabled the timely commencement of postoperative radiotherapy.
Conclusion
The importance of recruiting robust tissue for reconstruction of defects that are likely to require radiotherapy cannot be understated and deserves reiteration. In achieving a single-stage paramedian forehead flap reconstruction, the patient received an aesthetically sensitive reconstruction, timely healing and early postoperative radiotherapy. When tailoring reconstructions to meet the needs of our patients, it is important that we continue to challenge orthodoxy in surgical practice if a better result can be achieved safely, as exemplified by this case.
Patient consent
Patients/guardians have given informed consent to the publication of images and/or data.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship, and/or publication of this article.
Revised: August 21, 2023 AEST