Introduction
Microsurgical free tissue transfer, or the free flap, describes the dissection and removal of tissue with preservation of its vascular pedicle to reconstruct a complex, distant defect via microsurgical reanastomosis of the flap’s vasculature to recipient site vessels. Early detection of failing free flaps is of the upmost importance as early recognition of flap compromise reduces morbidity and increases salvage rates.1,2 Mechanisms of flap failure are largely due to circulatory dysfunction or microvascular thrombosis,3 lending it to early detection by ultrasonographic techniques (adjuncts). Adjuncts, such as the Cook-Swartz implantable Doppler (Bloomington, Indiana, USA), are cost-effective ways to detect early flap failure with improved salvage rates compared to clinical assessment alone.4–7 At the quaternary centre investigated, both external and implanted Doppler ultrasounds are used to monitor flap viability, particularly in buried orofacial flaps.
Free flaps continue to carry a 1 to 6 per cent failure rate at most institutions, even with the use of adjuncts, causing significant patient morbidity.8 Despite the theoretical and practical advantages of adjunct ways to detect flap failure, clinical assessment remains the gold-standard.1,2,9,10
Our study explores the factors responsible for missed early detection of free flap compromise by clinical and adjunct-based assessment. We speculate that inexperience, a lack of confidence, and paucity of education related to postoperative clinical assessment and use of adjuncts, contribute to suboptimal detection of flap failure. We further hypothesise that these factors are compounded by differences in the postoperative destination of patients, being either the intensive care unit (ICU) or microsurgical wards.
This study aims to determine the effectiveness of formal education on improving confidence in detecting early signs of free flap compromise. Additionally, the study aims to outline an educational model that can be used with frontline staff to best achieve this goal.
Methods
This study was conducted in accordance with the ethical standards of the 1964 Helsinki declaration and its later amendments with approval of the Central Adelaide Local Health Network Human Research Ethics Committee (CALHN HREC R20180903). Informed consent was obtained from all participants.
Our study comprised nursing staff from the ICU and microsurgical wards for plastic and reconstructive surgery and otolaryngology at a quaternary Australian institute involved in the care of free flaps. Nursing staff were recruited to attend an educational seminar by unit email distribution lists and advertisements at previous educational events. The seminar was delivered in presentation format and pertained to key facts in the clinical signs associated with a compromised free flap, technical guidelines for operating implantable and hand-held Doppler, troubleshooting, interpretation of results, and pathways for escalating a worrisome flap.
The cohort was provided with an anonymous standardised questionnaire (Supplementary material 1 and 2) pertaining to:
-
overall experience working with free flaps;
-
confidence level assessing viability of free flaps by clinical, arterial handheld Doppler, and venous Cook-Swartz implantable Doppler techniques; and
-
education administration and provision.
Prior to the survey the cohort was divided at random by seat number. The first group was surveyed before the educational seminar; the second group after the seminar.
Statistical methods
Differences in questionnaire items between cohorts were summarised descriptively with frequencies and percentages.
To generate a measure of overall confidence, each level on the response scale for the three confidence items (clinical, handheld Doppler and implantable Doppler) was assigned a numeric value from 1 through 5 corresponding to the responses of the modified Likert scale. Scores for the three confidence items were added to generate an overall confidence score, for all participants with complete confidence data (that is, no missing data for any of the confidence items). Overall confidence scores had a theoretical range from three to 15. Two participants in the pre-education group were missing data from one of the confidence items. These participants (2/122 = 1.6%) were excluded from the analysis of overall confidence. All participants in the post-education group (n = 51) had complete confidence data.
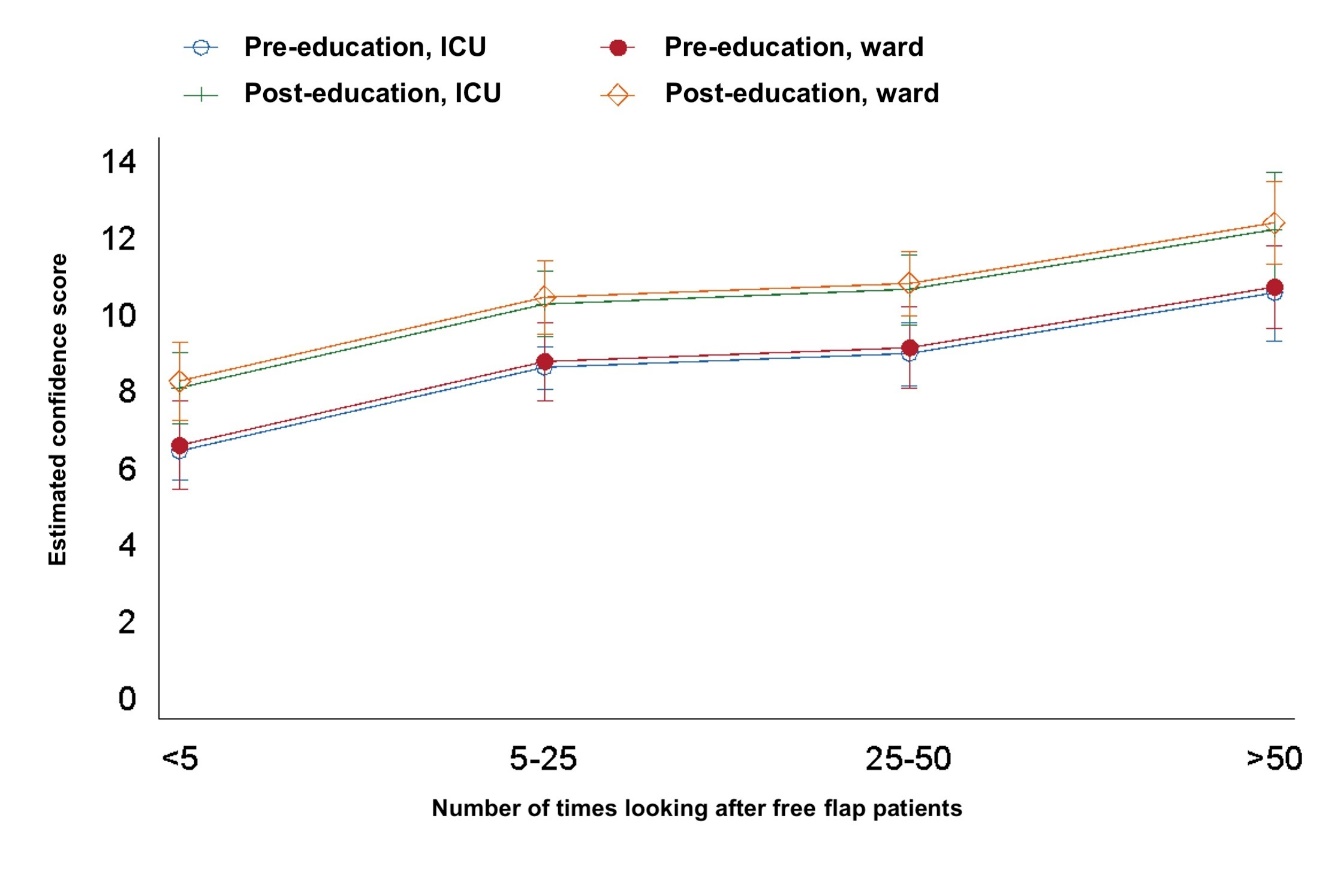
Overall confidence scores between the pre-education and post-education cohorts were compared using linear regression, controlling for both location (ICU versus ward) and reported level of experience in caring for free flap patients (less than 5 patients, 5–25 patients, 25–50 patients, more than 50 patients). The overall confidence score is a Likert scale and may be considered an interval scale that can be analysed using parametric techniques.11–13 Questionnaires were completed anonymously. To investigate whether differences in overall confidence also differed according to level of reported experience caring for free flap patients, a cohort-by-experience-level interaction term was included. Robust standard errors were specified and model adequacy was assessed by visual inspection of residuals.
All statistical analyses were carried out using Stata (Version 15, StataCorp, College Station, Texas, USA). The level of statistical significance was set to 0.05.
Results
Overall, 173 surveys were collected from ICU staff (n = 114) and ward staff (n = 59). Post-education surveys were completed by approximately one-third (n = 51) of the surveyed cohort.
Nearly half of all participants (47%) had identified a failing flap in their career. By location, most ICU staff (51%), and one third of ward staff (35%), had never identified a failing free flap. These flaps were mostly identified to be failing by clinical assessment alone (46%) or using both clinical and adjunct-based assessment (48%). Only one staff member had used adjunct-based assessment alone to identify a failing free flap.
Two-thirds of participants (66%) had experience using adjuncts in more than five free flap patients. Nearly one-third (32%) reported using adjuncts in more than 25 free flap patients. Overall ward staff reported more experience using adjuncts compared to ICU staff, with 58 per cent (n = 34) of ward staff caring for greater than 25 free flap patients, versus 18 per cent (n = 21) of ICU staff. Only 4 per cent (n = 4) of ICU staff reported caring for greater than 50 free flap patients with adjuncts, compared with 29 per cent (n = 17) of ward staff.
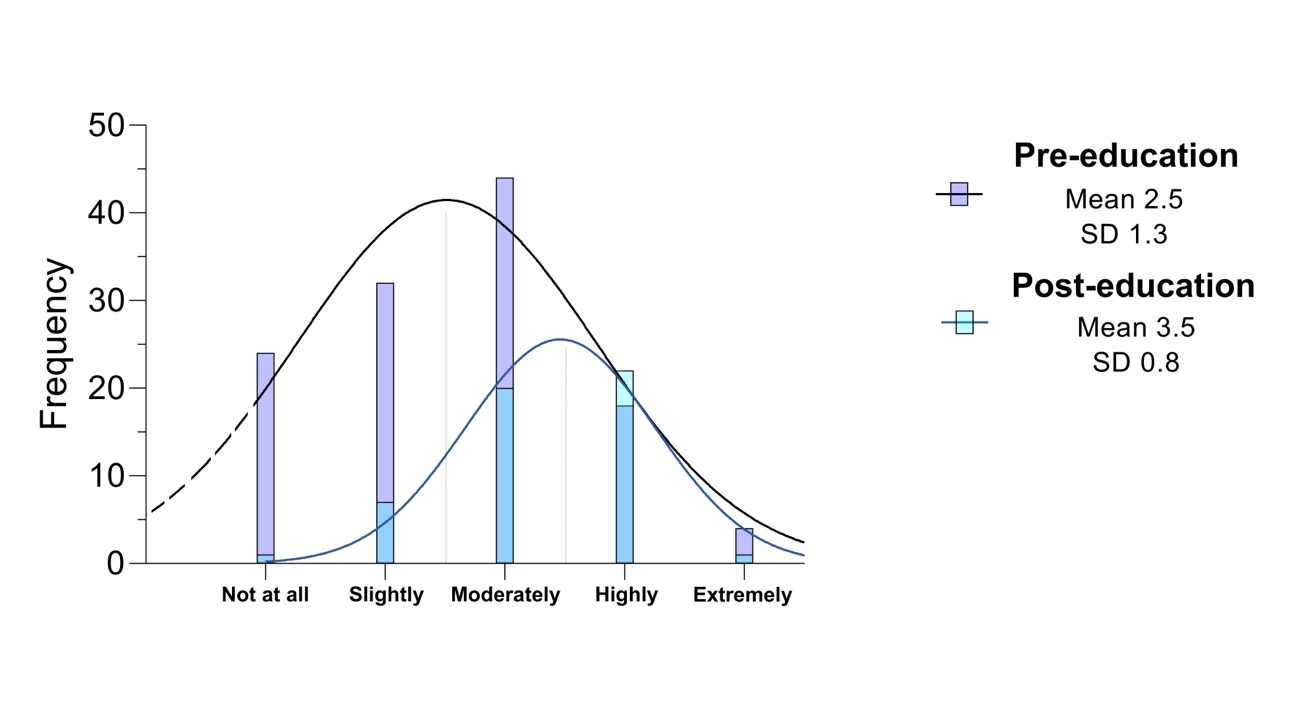
Most of our cohort felt either moderately, highly or extremely confident in assessing a free flap using clinical (73%), venous Doppler (63%) or handheld arterial Doppler (69%) methods. Most participants (59%) agreed that adjuncts help their assessment of a failing free flap but nearly one fifth of participants (17%) argued adjuncts make assessment more difficult. Confidence using clinical (p = 0.007), implanted Doppler (p < 0.0001) or external Doppler ultrasound (p < 0.0001) were globally increased among ward staff compared to ICU staff.
The education session unanimously increased confidence in understanding mechanisms of flap failure (100%, n = 51). Staff reported increased confidence in managing failing free flaps, escalating a failing free flap, and recommending the educational seminar to other nursing staff (98%, n = 50). Mean overall confidence was higher following education (M = 10.0, SD = 2.0), measurable as 1.7 units (95% CI 0.9, 2.5; p < 0.0001) when adjusting for confounding factors.
Discussion
Effective implementation of clinical and adjunct-based assessment methods in the early detection of free flap failure requires proficiency in their use by the multidisciplinary team. Informed and careful postoperative care is essential to the survival of transplanted tissue and preventing significant morbidity. Our study has explored the experiences of frontline users with several important insights. The authors hypothesise that improved nursing staff confidence and expertise in free flap examination with the help of adjuncts will improve early detection, escalation and timely intervention for compromised free flaps, reducing their fail rate and consequent morbidity.
Our study estimates the effect of education on confidence, as a surrogate marker of performance. The positive causal relationship of self-rated confidence and performance is established in both healthcare and non-healthcare settings.14–16 In nursing recruitment confidence is regarded as a key factor17 because confidence is thought to positively impact patient healthcare18 and enhance both safe nursing practices and patient safety.19,20 Curiously, the analysis pertaining to education, self-confidence and performance demonstrates a dependence of confidence on adequate education,21,22 and in general the positive correlation between academic achievement and confidence is robust.23–25 This is complemented by our study where confidence levels were unanimously increased following the educational intervention (Figure 1). High levels of confidence are associated with improved healthcare outcomes and we demonstrate a need for further education.

We demonstrated that a simple educational intervention significantly increased mean participant confidence across all levels of experience. Our seminar was arranged during prescribed nursing teaching hours and provided in four separate sessions. The presentation reflected our local published protocol on the ward-based management of free flaps. We detailed the principles of tissue transfer, established the basis for early free flap failure, and explained the rationale behind ward-based principles of care. These included topics on intravenous fluid therapy, ambient temperature, appropriate oxygenation, anticoagulation and thromboprophylaxis among others. Our presentation defined and delineated the clinical assessment of a free flap, as well as Doppler-based methods of assessment (their use, operation and troubleshooting). We presented scenario-based issues such as venous congestion or arterial occlusion, how these would be identified in the postoperative setting, and the appropriate escalation pathways for a worrisome flap.
Alarmingly, a significant portion of staff feel adjuncts make no difference to the ease of assessing failing free flaps (28%) or make assessments more complicated (17%). This is despite high levels of confidence in using, operating and interpreting flap changes using adjuncts. This finding reflects the current gold-standard of practice that clinical assessment takes priority above all, however the authors also feel this highlights a critical deficiency in education. Explicitly a need for further education was reported by 98 per cent of the cohort (119/121) and we demonstrated worthwhile and significant increases in confidence following our educational seminars (Figure 2). We suspect this is not unique to our centre and this lack of experience and education may contribute to unnecessary morbidity and increased rates of flap-failure. At all experience levels, our data shows education is a useful intervention to increase confidence. Staff who are more confident and experienced in using adjunct-based assessment, as they are in clinical examination, will become more proficient in using adjuncts for early detection of failing free flaps.

Regarding the postoperative destination of free flap patients, our study would suggest that ward staff have significantly more experience and confidence in caring for free flap patients than ICU staff. A greater proportion of ward staff have identified a failing free flap and used adjuncts to detect failures. This highlights an increased need for education in relatively inexperienced users of adjuncts in ICU. On multivariate analysis however, when adjusted for education and experience, there is no significant difference in confidence (p = 0.718) between ward and ICU staff. This result has significant implications determining the optimal postoperative destination and the authors conclude flap monitoring alone is not an indication for ICU admission.
A criticism of our study is the use of single survey in both groups, rather than direct pre-exposure and post-exposure comparison. The authors felt the alternate approach would increase response bias and staff would be compelled to artificially increase their confidence scores following intervention because they were asked to consider their responses twice. Given the large expected cohort size and appropriate randomisation, the authors anticipated the study could demonstrate a meaningful difference with reduced bias using single survey. A prospective study design would be beneficial to identify the extent to which education changes early flap failure salvage. Our study explores one of many factors at play in early free flap salvage.
Conclusion
Our study explores factors responsible for missed early detection of free flap compromise and highlights key deficits in confidence and education in the ward-based care of free flaps. This study demonstrates that a simple, formal educational seminar pertaining to mechanisms of flap failure, teaching on gold-standard assessment principles, use and interpretation of adjuncts, and clear escalation pathways, significantly improves nursing staff confidence in identifying an early failing free flap, at all levels of experience. Our study underscores the role for collaboration, upskilling and shared responsibility among the multidisciplinary surgical team to improve outcomes for free flap patients.
Conflict of interest
The authors have no conflicts of interest to disclose.
Funding declaration
The authors received no financial support for the research, authorship and/or publication of this article.
Revised: September 14, 2023 AEST